Keywords
HIV patent pool, resource-limited populations, antiretroviral medicines, trade context, manufacturers from middle-income countries, multinationals.
Shaping needs
4.8 billion people live in the developing countries: 43 percent of them rely on less than US$ 2 a day. Communicable diseases disproportionately affect these populations [1,2]. Drug treatments for these diseases may be very expensive, or toxic, or difficult to administer, or ineffective if microbial resistance spreads. With regard to HIV infection, only 5 million infected people (out of 15 million in need) were receiving specific medicines (antiretrovirals- ARVs) in the low- and middle-income countries in 2009, while Sub-Saharan Africa accounts for three-quarters of these figures and HIV resistance against first-line ARVs involves about 20% of patients in three years time from the beginning of treatments [3,4]. Thus, appropriately formulated novel medicines that are safe, affordable and effective are needed.
As the current patent system generates incentives for new drug development in profitable markets only, where originator firms can recoup their research and development (R&D) expenses through sales at monopoly high prices, it does not work for the poor end users in resource-limited countries.
Nonetheless, increasing pressure is registered nowadays for strategies able to promote pharmaceutical innovation and ensure long-term access to treatments by the poorest populations [2,5]. The resolutions of 61st World Health Organization (WHO)’s World Health Assembly included patent pools as part of the whole Global Strategy on Public Health, Innovation and Intellectual Property aimed to increase access to medicines, stimulate R&D related to diseases that disproportionately affect the developing world, and delink R&D costs from the end product prices [1].
A patent pool is created when a number of patents by different owners are pooled and made available on a non-exclusive basis to third parties (for instance, the generic drug manufacturers).
Major commitment to putting the patent pool idea into effect, by initially focusing on ARVs, is shown by UNITAID in its reference field as an international facility to provide long-term funding to increase access to drugs and diagnostics for HIV, malaria and tuberculosis (TB) [6]. As of November 1, 2010, the “Medicines Patent Pool” has transitioned out of UNITAID, and is functioning as a separate legal entity, though UNITAID continues to support it and is funding its operations under a five-year Memorandum of Understanding [7].
From public health and political economy perspectives, a key issue is how to design a suitable trade context for making the patent pool for ARVs both politically feasible and effective in achieving its goals. This paper contributes to debate and discussion of these issues.
A Troublesome Matter for Multinational Manufacturers
The patent pool plan invites patent holders to offer the intellectual property (IP) related to their inventions to the Medicines Patent Pool [7,8]. Any company that wants to use the IP to produce or develop ARVs can seek a license from the pool against the payment of royalties, and may then produce the medicines for use in developing countries (conditional upon meeting agreed quality standards). The plan relies on a voluntary mechanism, meaning its success will depend on the willingness of originator pharmaceutical companies to participate and commit their IP to the pool. Quantified benefits are expected to encompass, through greatly increased competition, substantially lower prices for second and third-line patent pool generated fixed-dose combination (FDC) ARVs1.
So compounded, the pool could help overcome inadequacies limiting the roles currently played by the brand and generic manufacturers in availability and supply of ARVs in resourcelimited countries [9]. Generic, mainly Indian, companies are supplying Sub-Saharan Africa with most of these drugs at prices below those charged by brand enterprises, and until now almost exclusively provided FDCs. Brand companies have supplied almost all newer second/third-line ARVs, stipulated voluntary licenses-VLs2 with generic firms, and pursued differential pricing.
Note that the ability of Indian firms to provide these ARVs is due to the fact that India delayed introduction of pharmaceutical patents until 2005 [10]. This means that most of the first-line drugs demanded throughout the developing world (and recommended by the WHO) are not patented in India. Indeed, the fact that the drugs principally in demand were unencumbered by patents in India was a crucial factor in facilitating the massive scaling up of ARV treatment since the early 2000s.
The coincidental connection between the drugs demanded and the drugs that Indian firms could supply is changing however [11,13]. Newer drugs are subject to patent protection in India and other supplier countries, which will make the supply heavily dependent on brand-name firms’ willingness to supply drugs at low cost or via VLs. There is good reason to believe that, in the absence of generic competition, the sources of supply are unstable. After all, VLs only account for a small fraction of current procurement, while non-enforcement policies have only been implemented selectively and at full discretion of the brand enterprises. Eventually, differential prices of brand products remain (with isolated exceptions) higher than the ones of corresponding generics: frequently, such prices have only been achieved after the threat of compulsory licenses-CLs2, or have sometimes failed to meet the promised country coverage due to delayed drug registration in entitled countries. Taking these realities into account, suited cutting edge ARVs for negotiations with the brand-name pharmaceutical sector were selected and put in the November 2009 UNITAID Patent Pool Implementation Plan [6].
The Medicines Patent Pool plan is generating concern among the originator pharmaceutical companies. They are reluctant to join the plan owing to fears that patent pooling could result in slashed profits of the brand-name industry in middleincome countries where a significant percentage of the population can afford out-of-pocket spending (about 300 million people in India, at least 800 million in China). Inherently, the originator companies suspect that patent pooling could result in an unbalanced surge of innovation, development and research activities undertaken by the middle-income countries’ (mainly India, China, Brazil, South-Africa, Thailand) manufacturers, in cutting edge generic FDC ARVs flooding the wealthy markets, in lost opportunities for VL agreements, as well as in a threat to their overall leadership [13,14]. Issues also involve the geographical scope of the licenses, specifically who will have access to the middle-income country markets; the measures to prevent products from entering high-income markets; the bonus for patent owners (such as regulatory incentives, funding sources, or alternate methods of calculating royalties) to include many of the middle-income countries in the pool licenses [6].
Meanwhile, though the US National Institutes of Health (NIH) recently licensed to the Medicines Patent Pool a royalty-free patent for third-line HIV drug darunavir (DRV), this is not enough to allow a generic low-cost version to be produced since other major manufacturers own different DRV patents [16]
Likely, the brand-name companies’ fears also take into account the economic and balance of power trends in the Asia-Pacific region, where China’s and India’s trade/business paces appear fast [9,17]. These insights look understandable now that Southern industries highly skilled in innovation, manufacturing and marketing are increasingly involved in South-South drug commercialization partnerships and in North-South R&D outsourcing ventures [9, 18-20]. While this environment means that trade competition between wealthy and middle-income countries is around the corner, it relies on moves (from WHO, World Intellectual Property Organization-WIPO, US President’s Emergency Plan for AIDS Relief-PEPFAR, European Union-EU) and on mounting circumstances, such as enforced CLs by middle-income countries, Patent Offices’ resistance to “evergreening” drug patent applications3, which reinforce each other and recommend the originator companies improve their policies to avoid their privileges being put in jeopardy [1, 2, 9, 13, 17, 21-31]. These changes add to the cost-saving ARVs bulk purchasing agreements achieved by Clinton HIV/AIDS Initiative (CHAI)-UNITAID/Global Fund coalitions with the generic manufacturers; the in progress setting of country-owned plants for generic ARV, malarial and TB drugs in Sub-Saharan Africa; and the multiplying free trade areas set up by the developing countries to enhance trade with one another [13, 17, 20, 32, 33].
Taken together, these realities translate as backing to the core interests of leading generic manufacturers and could result, should the originators refuse to join the patent pool, in CLs charged with constraining royalty clauses and tighter room for negotiations.
Overall, the conflicting matters reported here can actually prevent the multinational manufacturers from participating in the Medicines Patent Pool plan and may well support urgency for a new trade context formulated to reverse their reluctance to join. To this aim, partnerships between originator companies are needed first to make cutting edge brand fixed-dose combination (FDC) ARVs promptly available, and secondly, to allow patent pool agreements to be negotiated straight afterwards. Clauses that exclude middle-income countries from sharing in the patent pool must be rejected.
Partnerships for Cutting Edge Fixed-Dose Brand HIV Drug Combinations
Partnerships between originator companies are required in order to produce innovatory second/third-line brand FDC ARVs and then to allow patent pool agreements to be negotiated immediately afterwards. This would allow the brand-name manufacturers to keep R&D standards and marketing power, while profiting by additional joint venture opportunities, circumventing the need for further incentives to join the patent pool, and avoiding risks of CLs. Without counting, from an ethical perspective, the gain in prestige and corporate social responsibility for making up-to-date, adherence-enhancing drug formulations available while meeting pressures from the global health community.
The suggestion above looks ready to be implemented. Deals between originator companies have, indeed, been struck as far as joint manufacturing and production of second/thirdline brand FDC ARVs are concerned: for instance, the GlaxoSmithKline- Pfizer tie-up to merge HIV businesses into the new company ViiV Healthcare; and the Bristol Myers Squibb-Gilead venture for efavirenz (EFV)/emtricitabine (FTC)/tenofovir (TDF) FDC ATRIPLA® [13, 34]. These ventures would expectedly create additional partnerships now that a heat-stable 100 mg tablet version of Abbott ritonavir-RTV (which is the only sanctioned booster protease inhibitor-PI drug to be taken in conjunction with other PIs to enhance effectiveness) has been approved by both the European Medicines Agency (EMA) and the US Food and Drug Administration [35]. The expectations for additional brand partnerships would make even more sense by considering that several new ARVs and a novel booster drug are currently in the brand industry pipelines, while Tibotec is working with Gilead to produce a rilpivirine (RPV)/TDF/FTC once-daily FDC tablet up to competing with Bristol Myers Squibb-Gilead FDC ATRIPLA®) (Table 1) [36].
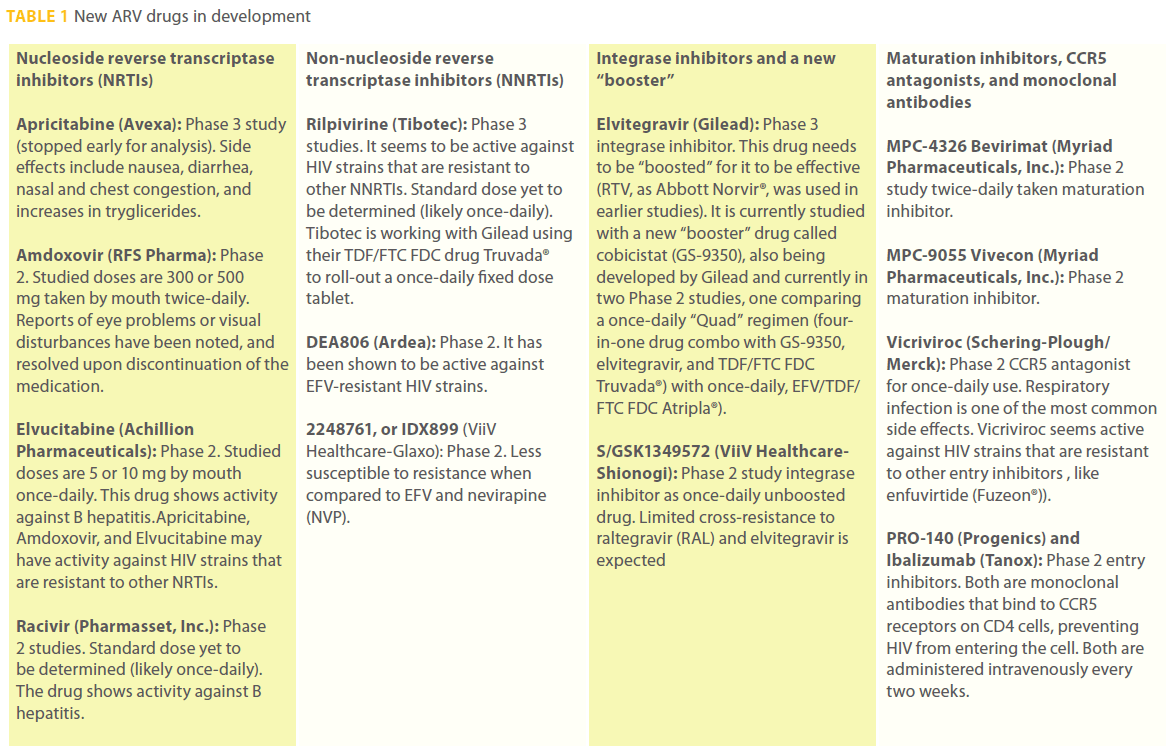
Table 1: New ARV drugs in development
These insights look intriguing in light of the breakthrough FDC ARVs recently brought out by the middle-income country (mainly Indian) generic manufacturers. Most of these generic formulations are reported in Table 2, wherein we can notice 1) that patent pools for first-line FDC ARVs are no longer needed in the developing countries, 2) that a number of FDC or copackaged ARVs (not available yet from brand companies) are rolled out only by the generic manufacturers [32, 37]. Among these, TDF/lamivudine (3TC)+ atazanavir (ATV)+heat stable RTV (by Mylan/Matrix) and TDF/FTC/EFV (by Matrix, Emcure and Cipla) deserve special mention as a forerunner formulation and copy of the blockbuster brand FDC ATRIPLA®, respectively.
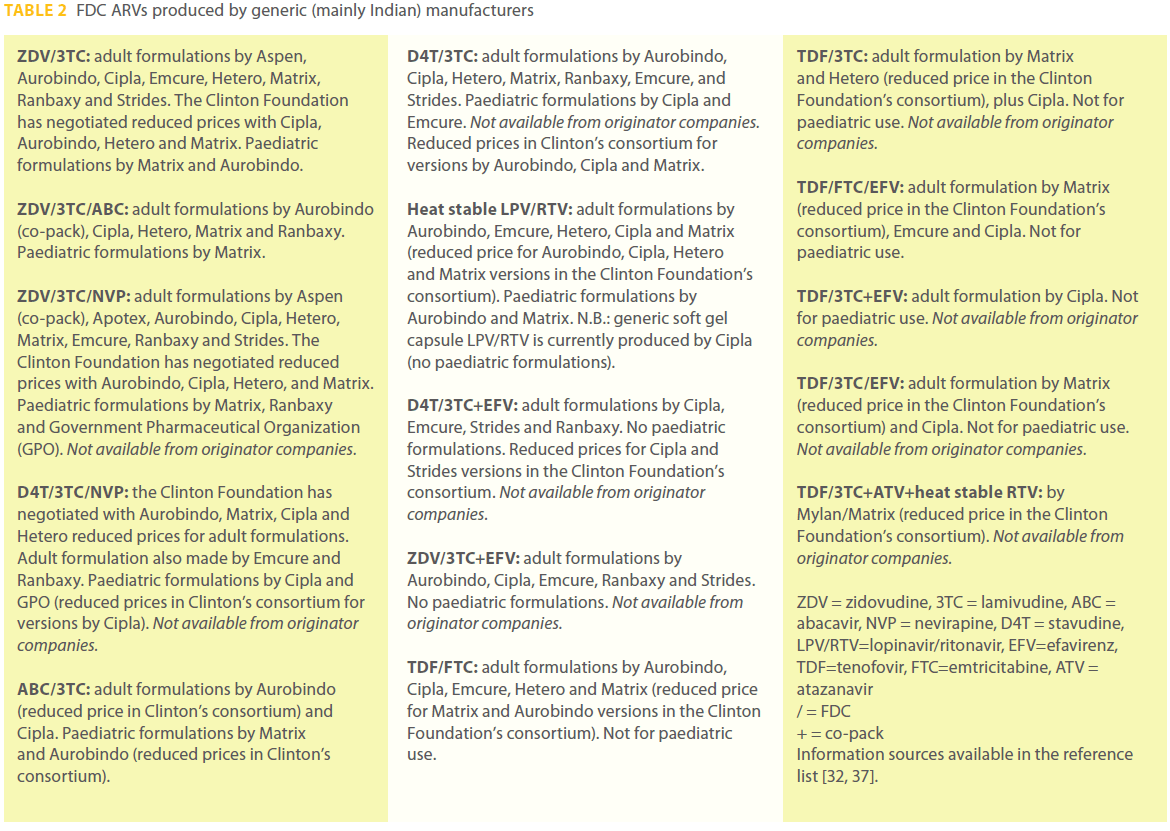
Table 2: FDC ARVs produced by generic (mainly Indian) manufacturers
The instances just cited would urge Bristol Myers Squibb-Gilead to enter patent pool as far as their FDC ATRIPLA® is concerned. Again, they would strongly advise Abbott, Bristol Myers Squibb and Gilead to soon partner and manufacture a ATV/heat stable RTV/TDF/FTC FDC to resist the forerunner Mylan/Matrix formulation (wherein 3TC and FTC are interchangeable).
Overall, these moves would allow the originators to maintain competitiveness as far as purchasing agreements with CHAIUNITAID/ Global Fund coalitions to supply the under-served markets with new FDC ARVs are concerned.
Aside from the quoted cases, the entire issue here seems enough to advise the brand corporations to straightaway enter into partnership and roll out cutting edge FDC ARVs, provided the requirements below are carried into effect:
• once-daily (alternatively, twice-daily) combinations.
• partnerships not exceeding two (three max) patent owners.
• formulations suitable for hot climate, poorly electric power equipped countries.
• alignment with DHHS, EACS and WHO ARV treatment guidelines [38-40].
As per the insights above, cutting edge FDCs should include at least those listed in Table 3. Among them, once-daily either RPV/TDF/FTC (Gilead-Tibotec) or elvitegravir (ELV)/cobicistat (GS-9350)/TDF/FTC (Gilead) play as expected options in the near future.
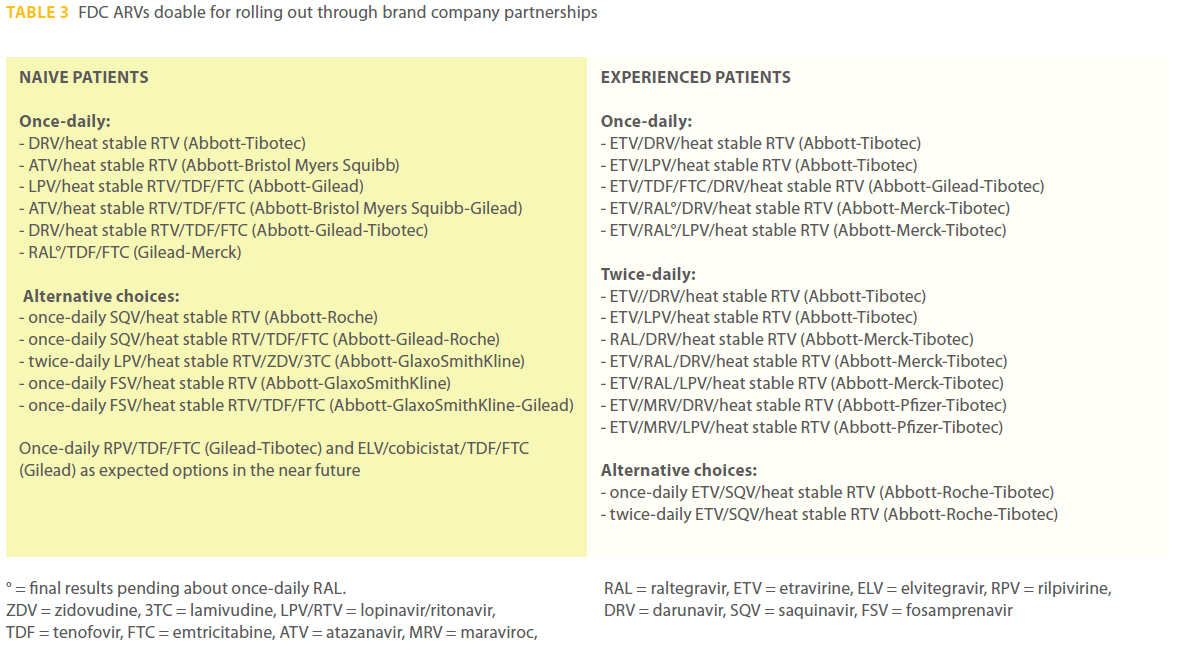
Table 3: FDC ARVs doable for rolling out through brand company partnerships
Non-Exclusion of Middle-Income Countries from the patent pool
In this context, clauses that exclude middle-income countries (World Bank defined) from sharing in the patent pool should be rejected. Indeed, the inclusion or exclusion of middle-income countries is a key issue that merits further discussion. Given the large and growing markets in such countries, the originator firms are reluctant to participate in a patent pool that allows generic drugs derived from the patent pool’s molecules to be sold in such countries. These firms want middleincome countries to be excluded in order to retain exclusive rights in such countries. Yet if the originator firms get their way and middle-income countries are excluded, it is difficult to see how the patent pool can be successful. One reason for this is that, while middle-income countries are home to almost all leading generic industries, many of them have high levels of HIV prevalence and thus high demand for cutting edge ARVs. The exclusion of middle-income countries would, therefore, exclude their own population from the patent pool market. Worse, this would severely affect the low-income countries as these are lacking in manufacturers qualified to meet home market needs with quality assured medicines. Excluding India, would mean excluding Africa given that Indian ARV manufacturers have substantially covered the African market needs [12]. So, it is odd to create a mechanism for scaling up treatment that, by design, would fail to address the treatment needs of the millions of people with HIV in the low- and middle-income countries.
A second reason for the importance of middle-income countries has to do with market structure. It is imperative that generic companies have an incentive to participate, to conduct R&D on molecules in the pool and develop appropriate formulations of generic FDCs to supply developing countries, and then sell them at low prices through UNITAID (and other organizations that pool procurement, such as the Clinton Foundation). The incentives to do so are a function of the size of the potential markets, i.e. the volume of sales that could make an exceptionally low-margin activity seem worthwhile, and if middle-income countries are excluded the patent pool may fail to promise enough demand to make it worthwhile for generic firms to participate [41]. This is a key – and perhaps irresolvable – conflict, and in designing the patent pool it is important that the price paid for originator firms’ participation not be so high as to make the patent pool ineffective.
Another important issue regards whether or not patent pooloriginated generic ARVs can be sold in the high-income country markets. Here we see the same trade-offs: originator firms will not want to contribute important molecules if doing so will reduce their sales in core, developed country markets; generic firms may not find participation worthwhile if they cannot sell products in markets with larger volumes. One possibility is to align the prices of these generic formulations with the corresponding brand ones in wealthy markets, so that generic firms cannot undercut originators in these markets. The loss of market share this could imply for the brand companies would be offset by retained leadership, royalty revenues from patent pool negotiations with generic firms, profitable new joint venture opportunities, and the avoidance of major threats to their profits. Of course, this solution risks introducing a perverse set of incentives for generic firms, encouraging them to dedicate finite resources and production capacity to selling drugs at high prices in already-served high-income markets rather than focus on serving low-income markets. Thus, it may make the most amount of sense – economically and politically – to allow generic firms to export to middle-income countries but prohibit them from exporting to high-income countries.
Expected Benefits
The trade context explored here can help speed up the participation of originator pharmaceutical companies in the Medicines Patent Pool plan and make it politically feasible and effective in achieving its goals. This context seems to be equipped to uphold fairly balanced needs/market-driven dynamics pro health in the drug trading policies facing generic and brand competitors. Additionally, it potentially tackles in an appropriate way the directions of evolution in emerging markets, while bringing benefits to the resource-limited populations, the multinational drug corporations and the pharmaceutical manufacturers from middle-income countries [9,42].
Conclusions
This study mixes analysis of health needs and of changing dimensions in both legislation and the pharmaceutical industry, with a political economy focus that considers the interests and capacities of key entities involved in global HIV treatment. This approach could compensate for a limitation of the study related to its attempt to analyze the future while the patent pool story is still unfolding. So compounded, this study presents feasible proposals in the current debate, without pretending to definitely address or overcome the conflicting issues.
Competing interests
The author declares that there are no competing interests.
Acknowledgments
The author is indebted to Dr. Kenneth C. Shadlen, Department of International Development, London School of Economics, London, UK for his valuable criticism on the study design and intellectual content. Thanks are expressed to Dr. Javier Guzman, Policy Cures London International Development Centre, London, UK for his constructive comments, and to Dr. Sergio Lo Caputo, Infectious Diseases Clinic, S.S. Annunziata Hospital, Firenze, Italy for expert advice on Table 3 contents.
Voluntary License - Agreement with the patent’s owner for manufacturing and marketing. Notwithstanding royalty rates imposition on generic firms, these licenses only imply straightforward agreements between companies; they do not require changes in national legislation, while including non-exclusivity, openings towards technology transfer, access to owner’s data for branded drugs as well as permission for export.
Compulsory License - When a poor country government allows to manufacture domestically or to import copies of patented drugs at prices much cheaper than those imposed by the patent holder and without his consent. Both importing and exporting countries need to have enabling legislation in place (a corresponding CL for export has to be issued by the exporting country). Prior negotiation with the patent owner for VL first is required except for situations including extreme health crisis and not-for-profit government use. Royalties to the patent owner are encompassed by CL rules.
1 FDC ARVs are multiple antiretroviral drugs combined into a single pill. They may combine different classes of ARVs or contain only a single class. These combinations allow people living with HIV to reduce the risk of developing virus resistance to treatments, while making life easier and increasing adherence by reducing the number of pills to be taken each day.
2 World Health Organization’s TRIPS (Trade-Related Aspects of Intellectual Property Rights) flexibilities: https://www.wto.org/English/tratop_e/ trips_e/intel2_e.htm
3 Most common in the pharmaceutical industry, “evergreening” patent application refers to the strategy of getting multiple patents that cover different aspects of the same product, usually by obtaining patents on improved versions of existing medicines.
References
- Sixty-first World Health Assembly: Global strategy and plan of action on public health, innovation and intellectual property (24 May 2008). Available https://www.who.int/gb/ebwha/pdf_files/ A61/A61_R21-en.pdf Accessed 5 May 2010.
- Mara K (21 May 2010). World Health Assembly creates new initiative for R&D financing. Intellectual Property Watch. Available https://www.ip-watch.org/weblog/2010/05/21/worldhealth- assembly-creates-new-initi.... Accessed 25 May 2010.
- WHO report (September 2010). Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. Available https://www.who.int/hiv/pub/2010progressreport/summary_ en.pdf Accessed 5 October 2010.
- Dionisio D (2010). Pooling ARV Drug Patents: A Pro-Access Fitting Strategy? Open AIDS Journal 4:1-3. Available https:// www.bentham.org/open/toaidj/openaccess2.htm Accessed 5 February 2011.
- Dionisio D (8 December 2009). HIV/AIDS Treatment Access Policies: Emerging Incentives for Pro-Poor Changes to IP? Intellectual Property Watch. Available https://www.ip-watch. org/weblog/2009/12/08/hivaids-treatment- access-policiesemerging- incentives-for-pro-poor-changes-to-ip/ Accessed 20 May 2010.
- UNITAID (November 2009). Patent Pool Implementation Plan Executive Summary. Available https://www.unitaid.eu/images/ meetings/ForWebsite_UNITAID_Patent_Pool_Implementation_ Plan_-_Executive_Summary.pdf Accessed 5 May 2010.
- UNITAID (November 2010). The Medicines Patent Pool is moving. Available https://www.medicinespatentpool.org/ https://www.unitaid.eu/en/20101108304/News/the-Medicines- Patent-Pool-is-Moving.html Accessed 10 February 2011.
- UNITAID (8 June 2010). Executive Board Session on Patent Pool. Available https://www.unitaid.eu/en/20100608263/News/FINALPHASE- OF-AIDS-MEDICINES-PATENT-POOL-ACCOMPLISHED.html Accessed 10 June 2010.
- Dionisio D, Fabbri C, Messeri D (2008). HIV drug policies and South markets: settling controversies. Therapy 5: 707-717. Available https://www.futuremedicine.com/doi/ abs/10.2217/14750708.5.5.707 Accessed 10 February 2011.
- Indian Revised Patent Law (2005). Available https://www. patentoffice.nic.in/ipr/patent/patent_2005.pdf Accessed 10 June 2010.
- Shadlen KC (forthcoming 2011). Is AIDS Treatment Sustainable? In Global Governance of HIV/AIDS: Intellectual Property and Access to Essential Medicines. Edited by Obijiofor Aginam, John Harrington and Peter K. Yu. Edward Elgar.
- Waning B, Diedrichsen E, Moon S (2010). A lifeline to treatment: the role of Indian generic manufacturers in supplying antiretroviral medicines to developing countries. Journal of the International AIDS Society 13: 35. Available https://www. jiasociety.org/content/13/1/35 Accessed 9 February 2011.
- Dionisio D (2011). India: intellectual property and HIV therapy for the developing world. Future Virology 6: 1-3. Available https:// www.futuremedicine.com/toc/fvl/6/1 Accessed 10 February 2011.
- Chauduri S (2010). R&D for development of new drugs for neglected diseases in India. International Journal of Technology and Globalisation 5: 61-75. Available https://www.inderscience. com/browse/index.php?journalID=104&year=2010&vol=5&iss ue=1/2 Accessed 9 February 2011.
- Jack A (15 December 2009). HIV pool adds to pressure on drug groups. Financial Times. Available www.hivatlas.org/.../17514- hiv-pool-adds-pressure-drug-groups Accessed 5 May 2010.
- UNITAID release (30 September 2010). US National Institutes of Health (NIH) first to share patents with Medecines Patent Pool. Available https://www.unitaid.eu/index2.php?option=com_cont ent&task=view&id=290&pop=1... Accessed 5 October 2010.
- Dionisio D (3 February 2011). Access to medicines: possible boost from a new balance of power in the Asia-Pacific region. IQsensato. Available https://www.iqsensato.org/blog/2011/02/03/ access-to-medicines-in-the-asia-pacific-region/ Accessed 9 February 2011.
- Engardio P (4 September 2008). Chinese Scientists Build Big Pharma Back Home. BusinessWeek . Available https:// www.businessweek.com/print/magazine/content/08_37/ b4099052479887.htm Accessed 20 May 2010.
- Engardio P, Weintraub A (4 September 2008). Outsourcing the Drug Industry. BusinessWeek. Available https://www. businessweek.com/print/magazine/content/08_37/ b4099048471329.htm Accessed 20 May 2010.
- Thorsteinsdottir H, Melon CC, Ray M, Chakkalackal S, Li M, Cooper JE, et al (2010). South-South entrepreneurial collaboration in health biotech. Nature Biotechnology 28: 407- 416. Available https://www.nature.com/nbt/journal/v28/n5/abs/ nbt0510-407.html Accessed 9 February 2011.
- WHO report (May 2010). Sixty-third World Health Assembly closes after passing multiple resolutions. Available https:// www.who.int/mediacentre/news/releases/2010/wha_ closes_20100521/en/index.html Accessed 11 February 2011.
- International Centre for Trade and Sustainable Development (28 April 2010). Developing countries launch new coalition at WIPO. Available https://ictsd.org/i/news/bridgesweekly/74748/ Accessed 20 May 2010.
- FDA News Release (6 October 2009). FDA marks 100th HIV/AIDS drug authorized for purchase under PEPFAR. Available https:// www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ ucm185416.htm Accessed 20 May 2010.
- Mara K (11 March 2010). European Generics Industry calls for “urgent patent reform”. Intellectual Property Watch. Available https://www.ip-watch.org/weblog/2010/03/11/europeangenerics- industry-calls-for-urg... Accessed 5 May 2010.
- Written Declaration on UNITAID HIV/AIDS Patent pool supported by 195 MEPs (19 October 2009). Available https:// www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP// NONSGML+WDECL+P7-DCL-2009-0055+0+DOC+PDF+V0// FR&language=FR Accessed 5 May 2010.
- Cronin D (28 January 2010). New Parliament Group monitors EU trade pacts’ impact on poor’s medicines access. Intellectual Property Watch. Available https://www.ip-watch.org/ weblog/2010/01/28/new-parliament-group-monitors-eu-trad... Accessed 20 May 2010.
- Council of the European Union (10 May 2010). Council conclusions on the EU role in global health. 3011th Foreign Affairs Council meeting, Brussels. Available https://www.eu-un.europa. eu/articles/es/article_9727_es.htm Accessed 20 May 2010.
- EuropeAid (2010). EU/WHO partnership on GSPA. Available https://www.onetec.be/global_health/doc/EU-WHO_GSPA_ info%20sheet_final.pdf Accessed 4 June 2010.
- European Parliament (2010). Resolution on progress towards the achievement of the Millennium Development Goals. Available https://www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP// TEXT+TA+P7-TA-2010-0210+0+DOC+XML+V0//EN&language=EN Accessed 5 July 2010.
- Saez C (22 April 2010). Ecuador grants first compulsory licence for HIV drug. Intellectual Property Watch. Available https:// www.ip-watch.org/weblog/2010/04/22/ecuador-grants-firstcompulsory- licence.... Accessed 5 May 2010.
- Medecins Sans Frontieres (7 January 2011). India rejects patents for two key AIDS drugs. Available https://www.msfaccess.org/ Accessed 10 January 2011.
- Medecins Sans Frontieres (Campaign for Access to Essential Medicines) (July 2010). Untangling the web of antiretroviral price reductions: 13th edition. Available www.msfaccess.org Accessed 13 July 2010.
- Dionisio D, Khanna AR, Nicolaou S, Raghavan V, Juneja S, Sengupta A, et a (2008). For-profit policies and equitable access to antiretroviral drugs in resource-limited countries. Future HIV Therapy 2: 25-36. Available https://www.futuremedicine.com/ toc/fht/2/1 Accessed 10 January 2011.
- Kaiser Daily HIV/AIDS Report (16 April 2009). GSK, Pfizer announce combined HIV/AIDS drug business. Available https://www.kaisernetwork.org/daily_reports/print_report. cfm?DR_ID=58033&dr_cat=1 Accessed 20 May 2010.
- Medecins Sans Frontieres Campaign for Access to Essential Medicines (December 2009). Heat-stable ritonavir approved: years of medical double standards and stranglehold by Abbott come to an end. Available https://www.msfaccess.org/main/ access-patents/heat-stable-ritonavir-approved/ Accessed 5 May 2010.
- Mehta S (2010). Coming Down The Line. Positively Aware March/April issue: 59-60. Available https://positivelyaware. com/2010/10_02/coming_down_the_line.shtml Accessed 5 May 2010.
- WHO list of prequalified medicinal products (2010). Available https://apps.who.int/prequal/ Accessed 5 December 2010.
- Department of Health and Human Services (DHHS) (1 December 2009). Guidelines for the use of antiretroviral agents in HIV- 1-infected adults and adolescents. Panel on Antiretroviral Guidelines for Adults and Adolescents. Available https://www. aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf Accessed 5 May 2010.
- European AIDS Cinical Society-EACS (November 2009). Guidelines for Clinical Management and Treatment of HIV Inected Adults in Europe, Version 5. Available https://www. europeanaidsclinicalsociety.org/guidelinespdf/1_Treatment_of_ HIV_Infected_Adults.pdf Accessed 5 May 2010.
- WHO (2010 revision). Antiretroviral therapy for HIV infection in adults and adolescents. Available https://www.who.int/hiv/pub/ arv/adult2010/en/index.html Accessed 5 December 2010.
- Shadlen KC (2007). The political economy of AIDS treatment: intellectual property and the transformation of generic supply. International Studies Quarterly 51: 559-581.
- Waning B, Kaplan W, Fox MP, Boyd-Boffa M, King AC, Lawrence DA, et al (2010). Temporal trends in generic and brand prices of antiretroviral medicines procured with donor funds in developing countries. Journal of Generic Medicines 7:159-175. Available https://www.palgrave-journals.com/jgm/journal/v7/n2/ full/jgm20106a.html Accessed 11 January 2011.
2526
References
- Sixty-first World Health Assembly: Global strategy and plan of action on public health, innovation and intellectual property (24 May 2008). Available https://www.who.int/gb/ebwha/pdf_files/ A61/A61_R21-en.pdf Accessed 5 May 2010.
- Mara K (21 May 2010). World Health Assembly creates new initiative for R&D financing. Intellectual Property Watch. Available https://www.ip-watch.org/weblog/2010/05/21/worldhealth- assembly-creates-new-initi.... Accessed 25 May 2010.
- WHO report (September 2010). Towards universal access: scaling up priority HIV/AIDS interventions in the health sector. Available https://www.who.int/hiv/pub/2010progressreport/summary_ en.pdf Accessed 5 October 2010.
- Dionisio D (2010). Pooling ARV Drug Patents: A Pro-Access Fitting Strategy? Open AIDS Journal 4:1-3. Available https:// www.bentham.org/open/toaidj/openaccess2.htm Accessed 5 February 2011.
- Dionisio D (8 December 2009). HIV/AIDS Treatment Access Policies: Emerging Incentives for Pro-Poor Changes to IP? Intellectual Property Watch. Available https://www.ip-watch. org/weblog/2009/12/08/hivaids-treatment- access-policiesemerging- incentives-for-pro-poor-changes-to-ip/ Accessed 20 May 2010.
- UNITAID (November 2009). Patent Pool Implementation Plan Executive Summary. Available https://www.unitaid.eu/images/ meetings/ForWebsite_UNITAID_Patent_Pool_Implementation_ Plan_-_Executive_Summary.pdf Accessed 5 May 2010.
- UNITAID (November 2010). The Medicines Patent Pool is moving. Available https://www.medicinespatentpool.org/ https://www.unitaid.eu/en/20101108304/News/the-Medicines- Patent-Pool-is-Moving.html Accessed 10 February 2011.
- UNITAID (8 June 2010). Executive Board Session on Patent Pool. Available https://www.unitaid.eu/en/20100608263/News/FINALPHASE- OF-AIDS-MEDICINES-PATENT-POOL-ACCOMPLISHED.html Accessed 10 June 2010.
- Dionisio D, Fabbri C, Messeri D (2008). HIV drug policies and South markets: settling controversies. Therapy 5: 707-717. Available https://www.futuremedicine.com/doi/ abs/10.2217/14750708.5.5.707 Accessed 10 February 2011.
- Indian Revised Patent Law (2005). Available https://www. patentoffice.nic.in/ipr/patent/patent_2005.pdf Accessed 10 June 2010.
- Shadlen KC (forthcoming 2011). Is AIDS Treatment Sustainable? In Global Governance of HIV/AIDS: Intellectual Property and Access to Essential Medicines. Edited by Obijiofor Aginam, John Harrington and Peter K. Yu. Edward Elgar.
- Waning B, Diedrichsen E, Moon S (2010). A lifeline to treatment: the role of Indian generic manufacturers in supplying antiretroviral medicines to developing countries. Journal of the International AIDS Society 13: 35. Available https://www. jiasociety.org/content/13/1/35 Accessed 9 February 2011.
- Dionisio D (2011). India: intellectual property and HIV therapy for the developing world. Future Virology 6: 1-3. Available https:// www.futuremedicine.com/toc/fvl/6/1 Accessed 10 February 2011.
- Chauduri S (2010). R&D for development of new drugs for neglected diseases in India. International Journal of Technology and Globalisation 5: 61-75. Available https://www.inderscience. com/browse/index.php?journalID=104&year=2010&vol=5&iss ue=1/2 Accessed 9 February 2011.
- Jack A (15 December 2009). HIV pool adds to pressure on drug groups. Financial Times. Available www.hivatlas.org/.../17514- hiv-pool-adds-pressure-drug-groups Accessed 5 May 2010.
- UNITAID release (30 September 2010). US National Institutes of Health (NIH) first to share patents with Medecines Patent Pool. Available https://www.unitaid.eu/index2.php?option=com_cont ent&task=view&id=290&pop=1... Accessed 5 October 2010.
- Dionisio D (3 February 2011). Access to medicines: possible boost from a new balance of power in the Asia-Pacific region. IQsensato. Available https://www.iqsensato.org/blog/2011/02/03/ access-to-medicines-in-the-asia-pacific-region/ Accessed 9 February 2011.
- Engardio P (4 September 2008). Chinese Scientists Build Big Pharma Back Home. BusinessWeek . Available https:// www.businessweek.com/print/magazine/content/08_37/ b4099052479887.htm Accessed 20 May 2010.
- Engardio P, Weintraub A (4 September 2008). Outsourcing the Drug Industry. BusinessWeek. Available https://www. businessweek.com/print/magazine/content/08_37/ b4099048471329.htm Accessed 20 May 2010.
- Thorsteinsdottir H, Melon CC, Ray M, Chakkalackal S, Li M, Cooper JE, et al (2010). South-South entrepreneurial collaboration in health biotech. Nature Biotechnology 28: 407- 416. Available https://www.nature.com/nbt/journal/v28/n5/abs/ nbt0510-407.html Accessed 9 February 2011.
- WHO report (May 2010). Sixty-third World Health Assembly closes after passing multiple resolutions. Available https:// www.who.int/mediacentre/news/releases/2010/wha_ closes_20100521/en/index.html Accessed 11 February 2011.
- International Centre for Trade and Sustainable Development (28 April 2010). Developing countries launch new coalition at WIPO. Available https://ictsd.org/i/news/bridgesweekly/74748/ Accessed 20 May 2010.
- FDA News Release (6 October 2009). FDA marks 100th HIV/AIDS drug authorized for purchase under PEPFAR. Available https:// www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ ucm185416.htm Accessed 20 May 2010.
- Mara K (11 March 2010). European Generics Industry calls for “urgent patent reform”. Intellectual Property Watch. Available https://www.ip-watch.org/weblog/2010/03/11/europeangenerics- industry-calls-for-urg... Accessed 5 May 2010.
- Written Declaration on UNITAID HIV/AIDS Patent pool supported by 195 MEPs (19 October 2009). Available https:// www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP// NONSGML+WDECL+P7-DCL-2009-0055+0+DOC+PDF+V0// FR&language=FR Accessed 5 May 2010.
- Cronin D (28 January 2010). New Parliament Group monitors EU trade pacts’ impact on poor’s medicines access. Intellectual Property Watch. Available https://www.ip-watch.org/ weblog/2010/01/28/new-parliament-group-monitors-eu-trad... Accessed 20 May 2010.
- Council of the European Union (10 May 2010). Council conclusions on the EU role in global health. 3011th Foreign Affairs Council meeting, Brussels. Available https://www.eu-un.europa. eu/articles/es/article_9727_es.htm Accessed 20 May 2010.
- EuropeAid (2010). EU/WHO partnership on GSPA. Available https://www.onetec.be/global_health/doc/EU-WHO_GSPA_ info%20sheet_final.pdf Accessed 4 June 2010.
- European Parliament (2010). Resolution on progress towards the achievement of the Millennium Development Goals. Available https://www.europarl.europa.eu/sides/getDoc.do?pubRef=-//EP// TEXT+TA+P7-TA-2010-0210+0+DOC+XML+V0//EN&language=EN Accessed 5 July 2010.
- Saez C (22 April 2010). Ecuador grants first compulsory licence for HIV drug. Intellectual Property Watch. Available https:// www.ip-watch.org/weblog/2010/04/22/ecuador-grants-firstcompulsory- licence.... Accessed 5 May 2010.
- Medecins Sans Frontieres (7 January 2011). India rejects patents for two key AIDS drugs. Available https://www.msfaccess.org/ Accessed 10 January 2011.
- Medecins Sans Frontieres (Campaign for Access to Essential Medicines) (July 2010). Untangling the web of antiretroviral price reductions: 13th edition. Available www.msfaccess.org Accessed 13 July 2010.
- Dionisio D, Khanna AR, Nicolaou S, Raghavan V, Juneja S, Sengupta A, et a (2008). For-profit policies and equitable access to antiretroviral drugs in resource-limited countries. Future HIV Therapy 2: 25-36. Available https://www.futuremedicine.com/ toc/fht/2/1 Accessed 10 January 2011.
- Kaiser Daily HIV/AIDS Report (16 April 2009). GSK, Pfizer announce combined HIV/AIDS drug business. Available https://www.kaisernetwork.org/daily_reports/print_report. cfm?DR_ID=58033&dr_cat=1 Accessed 20 May 2010.
- Medecins Sans Frontieres Campaign for Access to Essential Medicines (December 2009). Heat-stable ritonavir approved: years of medical double standards and stranglehold by Abbott come to an end. Available https://www.msfaccess.org/main/ access-patents/heat-stable-ritonavir-approved/ Accessed 5 May 2010.
- Mehta S (2010). Coming Down The Line. Positively Aware March/April issue: 59-60. Available https://positivelyaware. com/2010/10_02/coming_down_the_line.shtml Accessed 5 May 2010.
- WHO list of prequalified medicinal products (2010). Available https://apps.who.int/prequal/ Accessed 5 December 2010.
- Department of Health and Human Services (DHHS) (1 December 2009). Guidelines for the use of antiretroviral agents in HIV- 1-infected adults and adolescents. Panel on Antiretroviral Guidelines for Adults and Adolescents. Available https://www. aidsinfo.nih.gov/ContentFiles/AdultandAdolescentGL.pdf Accessed 5 May 2010.
- European AIDS Cinical Society-EACS (November 2009). Guidelines for Clinical Management and Treatment of HIV Inected Adults in Europe, Version 5. Available https://www. europeanaidsclinicalsociety.org/guidelinespdf/1_Treatment_of_ HIV_Infected_Adults.pdf Accessed 5 May 2010.
- WHO (2010 revision). Antiretroviral therapy for HIV infection in adults and adolescents. Available https://www.who.int/hiv/pub/ arv/adult2010/en/index.html Accessed 5 December 2010.
- Shadlen KC (2007). The political economy of AIDS treatment: intellectual property and the transformation of generic supply. International Studies Quarterly 51: 559-581.
- Waning B, Kaplan W, Fox MP, Boyd-Boffa M, King AC, Lawrence DA, et al (2010). Temporal trends in generic and brand prices of antiretroviral medicines procured with donor funds in developing countries. Journal of Generic Medicines 7:159-175. Available https://www.palgrave-journals.com/jgm/journal/v7/n2/ full/jgm20106a.html Accessed 11 January 2011.

