Luzi Mario1*, Refi Giada1,Scerrati Massimo2 and Capucci Alessandro1
1Clinica di Cardiologia, Università Politecnica delle Marche, Ancona, Italia.
2Clinica di Neurochirurgia, Università Politecnica delle Marche, Ancona, Italia.
*Corresponding Author:
Dr. Mario Luzi
Clinica di Cardiologia, Università Politecnica delle Marche
Ancona, Italia, Via Conca 71, 60131
Torrette di Ancona, Ancona, Italy
Tel: +390715964474
E-mail: marioluzi@virgilio.it
Citation: Mario L, Giada R, Massimo S, et al. A Huge J Wave in Mild-Hypothermic Patient with Acute Brain Injury. J Neurol Neurosci. 2016, 6:3. doi: 10.21767/2171-6625.100023
Received Date: July 23, 2015; Accepted Date: October 02, 2015; Published Date: October 05, 2015
Keywords
Mild-Hypothermic, Acute Brain Injury; Electrocardiogram (ECG); Computerized Tomography (CT)
Introduction
The Osborn wave is a deflection immediately following the QRS complex of the surface ECG. When partially buried in the R wave, the J wave appears as J-point elevation or ST-segment elevation.
In the historical view, different names have been used for this wave in the medical literature, such as “camel-hump sign”, “late delta wave”, “hathook junction”, “hypothermic wave”, “J point wave”, “K wave”, “H wave” and “current of injury”.
Although there is no definite consensus about terminology of this wave, either “Osborn wave” or “J wave” are the most commonly used names for this wave in the current clinical and experimental cardiology. The Osborn wave can be generally observed in hypothermic patients [1-4].
Several lines of evidence have suggested that the cellular mechanism of Osborn wave appears to be related to an epicardialendocardial voltage gradient associated with the presence of a prominent epicardial action potential notch. A highly significant correlation was shown between the amplitude of the epicardial notch and the amplitude of the Osborn wave recorded during several interventions, including: hypothermia, premature stimulation, block of Ito by 4-aminopyridine, hypercalcemia or ischaemic condition. In 1959, Emslie-Smith et al. [5] found differences in the endocardial and epicardial responses of the ventricular myocardium to cold, and the Osborn wave was more prominent in the epicardial than endocardial leads. In 1988, Litovsky and Antzelevitch [6] proposed a difference in the electrophysiology of the ventricular epicardium and endocardium as the basis for the Osborn waves. The 4-aminopyridine sensitive transient outward current (Ito) was shown to be prominent in canine ventricular epicardium, but not in the endocardium. The more conspicuous notched configuration of the epicardial action potential was supposed to produce a transmural voltage gradient during ventricular activation that manifested as the Osborn wave in the ECG.
Beyond hypothermia, other conditions have been reported to cause Osborn waves, such as hypercalcemia [7], brain injury [8], subarachnoid haemorrhage [9], cardiopulmonary arrest from oversedation [10], vasospastic angina [11], or idiopathic ventricular fibrillation [12-14].
Case Report
A 51-year-old man was admitted to the emergency department of our hospital because of loss of consciousness with tonic clonic seizures and fall to the ground followed by consciousness recovery. He had a history of diabetes mellitus, HCV-related liver disease.
On the first examination his heart rate was 68 bpm and his blood pressure was 130/80 mmHg and body temperature of 37.9°C. Cardiovascular physical examination showed rhythmic cardiac tones, no cardiac murmurs, physiological vesicular murmur, absence of pulmonary stasis and legs edema. The following laboratory – tests were abnormal: AST( 184 U/l), gamma-GT (73 U/l), amilase 326 U/l, LDH (941 U/l), CPK 13047 U/l), myoglobin (>10000 ng/ml) and CK-MB ( 13.8 ng/ml) troponin I (0.39 ng/ml), calcium ( 6.7 mg/dl), albumin ( 2.8 mg/dl).
Potassium, magnesium, chlorine, sodium, creatinine were all in the normal range.
The cranial CT showed intraparenchymal hematoma with minimal subarachnoid haemorrhage (Figure 1). Then he was intubated (CGS=11) and referred to neurosurgical decompressive craniectomia. During the hospitalization, after the neurosurgical intervention, the intracranial pressure (PICm) was in range, between 4 mmHg and 12 mmHg and the body temperature ranged between 35.5°C e 37.9°C.
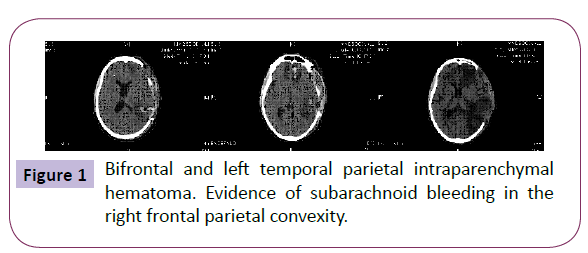
Figure 1: Bifrontal and left temporal parietal intraparenchymal hematoma. Evidence of subarachnoid bleeding in the right frontal parietal convexity.
A 12 lead ECG revealed sinus rhythm, normal PR interval, ST depression in V1- V4 leads with T- negative waves in all leads except for aVR. QTc measured 720 msec (Figure 2).
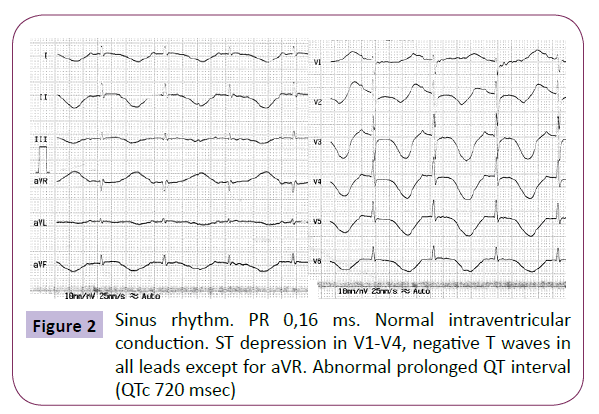
Figure 2: Sinus rhythm. PR 0,16 ms. Normal intraventricular conduction. ST depression in V1-V4, negative T waves in all leads except for aVR. Abnormal prolonged QT interval (QTc 720 msec)
During the night the patient experienced episode of ventricular tachycardia (no strips available) that required lidocaine, magnesium infusion and even 3 DC shocks.
After sinus rhythm restoration the 12 lead ECG showed the presence of a huge Osborn wave in all leads with normal PR and reduced QTc of 520 msec (Figure 3).
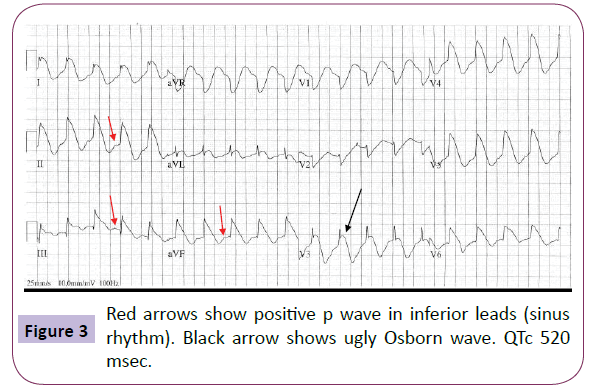
Figure 3: Red arrows show positive p wave in inferior leads (sinus rhythm). Black arrow shows ugly Osborn wave. QTc 520 msec.
At the hospital discharge, eleven days later, ECG had returned to normal (Figure 4).
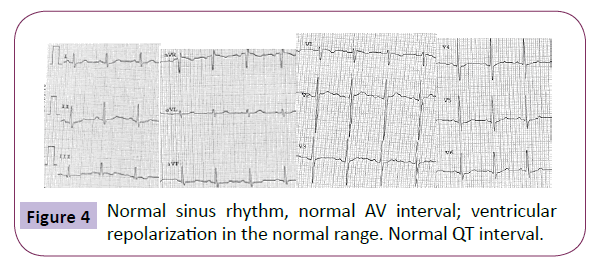
Figure 4: Normal sinus rhythm, normal AV interval; ventricular repolarization in the normal range. Normal QT interval.
Discussion
In 1953, Osborn [15] studied the effect of hypothermia on the respiratory and cardiac functions in dogs. Experimentally-induced hypothermia caused the development of a distinct deflection at the J point on the ECG, which he called “current of injury”. Osborn considered acidemia induced by hypothermia as a primary cause of that wave, because it disappeared when the arterial pH was normalized by hyperventilation during the same degree of cooling [15]. Osborn waves of hypothermia are most commonly observed in leads II, III, aVF, V5, and V6. They tend to appear in all leads when the hypothermia is severe and, conversely, in fewer leads during less severe hypothermia. However, variations and exceptions of both of these tendencies have been noted. In general, the lower the body temperature the largest the amplitude and duration of the Osborn wave. However, not all patients with hypothermia manifest an Osborn wave, the correlation being approximately 80%. The amplitude and duration of the Osborn wave diminishes during the rewarming process, and in some cases a small notch persists after recovery.
The prominent J wave is considered pathognomonic of severe hypothermia [16,17], although it has also been described in other clinical entities not associated with hypothermia, such as hypercalcemia, Brugada syndrome, cardiac arrest, and dysfunction of cervical sympathetic system, our patient did not have these conditions except for subarachnoid hemorrhage.
Non hypothermic J wave is an infrequent electrocardiographic manifestation of subarachnoid hemorrhage and of acute brain injury [18,19].
In our case the presence of a mild hypothermia and brain injury led to significant alterations of ventricular repolarization. However there is a discrepancy between the mild transient hypothermia with minimal subarachnoid hemorrhage and the severe alterations of ventricular repolarization.
The electrocardiographic changes of hypothermia, even if accompanied by increases in cardiac cytolysis enzymes, must always be evaluated in the clinical context, taking into account the many causes of false diagnosis of ischemia. The hypothermia eventually related to acute or subacute cerebral problem must be considered among the causes of false diagnosis of myocardial ischemia.
The electrocardiographic changes that occur in certain situations should not be confused with ischemic changes.
A sustained ventricular tachycardia leading to cardiac arrest could be a complication to be considered especially when, as in our case, there is a concomitant very long and transient QTc. A strict monitoring of ECG and of the clinical and biochemical parameters together with a progressive rewarming is sufficient to normalized the clinical picture and highly contribute to save a life.
7175
References
- Gussak I, Bjerregaard P, Egan TM, Chaitman BR (1995) ECG phenomenon called the J wave:history, pathophysiology, and clinical significance. J Electrocardiol 28: 49-58.
- Thompson R, Rich J, Chmelik F, Nelson W (1977) Evolutionary changes in the electrocardiogramof severe progressive hypothermia. J Electrocardiol 10: 67-70.
- Okada M, Nishimura F, Yoshino H, Kimura M, Ogino T (1983) The J wave in accidentalhypothermia. J Electrocardiol 16: 23-28.
- EmslieSD, Salden GE, Stirling GR (1959)The significance of changes in theelectrocardiogram in hypothermia. Br Heart J 21: 343.
- Litovsky SH, Antzelevitch C (1988) Transient outward current prominent in canine ventricularepicardium but not endocardium. Circ Res 62: 116-126.
- Sridharan MR, Horan LG (1984) Electrocardiographic J wave of hypercalcemia. Am J CardiolIndian Pacing and Electrophysiology Journal 54: 672-673.
- Hersch C (1961) Electrocardiographic changes in head injuries. Circulation 23: 853-860.
- De Sweit J (1972) Changes simulating hypothermia in the electrocardiogram in subarachnoidhemorrhage. J Electrocardiol 5: 93-95.
- Jain U, Wallis DE, Shah K, Blakeman BM, Moran JF (1990) Electrocardiographic J waves afterresusitation from cardiac arrest. Chest 98: 1294-1296.
- Maruyama M, Atarashi H, Ino T, Kishida H (2002) Osborn waves associated with ventricularfibrillation in a patient with vasospastic angina. J CardiovascElectrophysiol 13: 486-489.
- Aizawa Y, Tamura M, Chinushi M, Naitoh N, Uchiyama H, et al. (1993) Idiopathic ventricular fibrillation and bradycardia-dependent intraventricular block. AmHeart J 126: 1473-1474.
- Takeuchi T, Sato N, Kawamura Y, Takahashi F, Sato M, et al. (2003) A case of a short-coupled variant of Torsades de Pointes with electricalstorm. PACE 26: 632-636.
- Kalla H, Yan GX, Marinchak R (2000) Ventricular fibrillation in a patient with prominent J(Osborn) waves and ST segment elevation in the inferior electrocardiographic leads: a Brugadasyndrome variant? J CardiovascElectrophysiol 11: 95-98.
- Osborn JJ (1953) Experimental hypothermia: Respiratory and blood pH changes in relation tocardiac function. Am J Physiol 175: 389-398.
- Satoshi K, Ichiro I (2007) Prominent J wave in Accidental Hypothermia. Mayo Clinic Proc December 82: 1449.
- Veronica AM, Holli AB, John AE (2010) Hypothermia-related Elctrocardiographic Abnormalities: Osborn Waves. Anesthesiology112: 6
- Millewska AGP, Rudzka M (2009) J-wave formation in patients with acute intracranial hypertension. J Electrocardiol 42:420-423.
- Antzelevitch C, Yan GX (2009) J wave syndromes. Heart Rhythm 7:549-558.

