LACS Dahanayake1*, A Jasinghe2 and HHDNP Opatha3
1Senior Registrar in Medical Administration, Institute of Medicine, University of Colombo, Director of Research (former), Education, Training and Research Unit, Ministry of Health, Nutrition and Indigenous Medicine of Sri Lanka, Visiting Research Fellow, The University of York, Heslington, The United Kingdom
2Director General of Health Services, Ministry of Health, Nutrition & Indigenous Medicine of Sri Lanka, Sri Lanka
3Department of Human Resource Management, Faculty of Management Studies and Commerce, University of Sri Jayewardenepura, Sri Lanka
- *Corresponding Author:
- LACS Dahanayake
Senior Registrar in Medical Administration
Postgraduate Institute of Medicine, University of Colombo
Director of Research (former), Education, Training and Research Unit
Ministry of Health, Nutrition and Indigenous Medicine of Sri Lanka
Visiting Research Fellow, The University of York, Heslington, The United Kingdom
Tel: 07464266903
E-mail: lcsd502@york.ac.uk
Received date: January 12, 2019; Accepted date: January 29, 2019;; Published date: February 5, 2019
Citation: Dahanayake LACS, Jasinghe A, Opatha HHDNP (2019) A Managerial Intervention to Strengthen the Healthy Organizational Culture in Major Health Care Facilities of Sri Lanka. Health Syst Policy Res Vol. 6 No.1: 79.
Copyright: © 2019 Dahanayake LACS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Healthy organizational culture; McGregor’s theory X and theory Y; The consideration and initiation spectrum; The leader-subordinate relationship; Assertiveness; Transactional analysis; Negotiation skills
Introduction
Hospitals are high-risk organizations as they deal with life and death of human beings around the clock. The purpose of existence of a hospital is to cure patients with its optimal capacity while ensuring patient safety. Therefore, a healthy organizational culture is a significant prerequisite to ensure patient safety processes in a hospital setup. A healthy organizational culture treats employees of the organization as one of the most necessary recourses and attempts to enhance employees' wellbeing. Motivated, happy, productive health care worker is a key determinant of error-free, certain, efficient patient care services. Therefore, it is evident base reporting that patient safety culture can easily be built upon by well-developed, sustainable, healthy organizational culture [1-3].
There are three major dimensions of healthy organizational culture; the level of leaders’ attitude orientation about subordinates (Douglas McGregor’s Theory X and Theory Y), the degree of leaders’ Consideration and Initiating spectrum and the leader-subordinate relationship. Leaders are supposed to have appropriate attitudes about subordinates, to exhibit an optimal level of both Consideration and Initiation behaviours, and to maintain a strong superior-subordinate relationship to build a healthy organizational culture in their entity [4,5].
In general, there are two major mechanisms that leaders can use to embed a culture; primary embedding mechanism and secondary embedding mechanism. Above all, leaders’ conflict management competencies determine the state or degree of healthy organizational culture of an organization and hence it is a major primary embedding mechanism [6,7].
The objective of this Research project is to study the effectiveness of a newly designed conflict management interventional program for enhancing the healthy organizational culture of Nursing Heads in the National Hospital of Sri Lanka [8-10].
Design
As far as this interventional study is concerned, a conflict management program plays a significant role in creating right competencies within the unit of analysis that is individual level: nursing head in respect of conflict management. If leaders have right competencies of conflict management, they understand that dysfunctional conflicts need to be avoided; subordinates need to be valued; getting things done with subordinates and through subordinates collaboratively is indispensable and engage in actions that will avoid or minimize the occurrence of dysfunctional conflicts. Thus, the conflict management program, which is expected to be developed under this study, is considered as the independent variable while healthy organizational culture is considered as the dependent variable [11-13].
The study area selected for this research project is National Hospital of Sri Lanka (NHSL). National Hospital of Sri Lanka is the biggest tertiary care center in Sri Lanka as well as South East Asia. The study population in this research project is nursing heads as the study was conducted by using control and experimental groups (Figure 1).
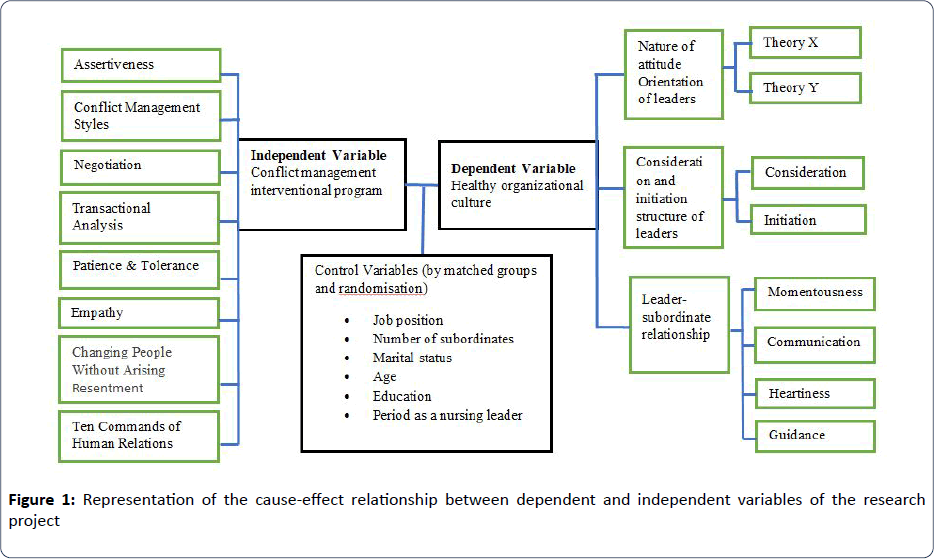
Figure 1: Representation of the cause-effect relationship between dependent and independent variables of the research project
Methods
This study consisted of four main stages.
During stage 1
The working definition of HOC was formulated, and The HOC Description Questionnaire consisted of 3 main dimensions, and 30 sub-dimensions were developed. The Perceived level of HOC of Nursing Heads was assessed as the pre-interventional survey using this study instrument.
During stage 2
The key leadership competencies concerning conflict management and three dimensions of HOC were identified, the gaps of these competencies were measured using eight point competency index test, and the intervention was designed to fill the identified gaps of given competencies. The methods used to design included the best possible intervention literature review, Delphi technique among subject experts, key informative interviews with Chief Nursing Officer and Nursing Sisters, Focal group discussions among unit leaders and experts’ opinions. Then the Manual on Eight Point Conflict Management Program for nursing leaders was written, and implementation plan consisted with preparing action plans, arranging logistics, preparing workshop agenda and budgeting workshops were finalized [14-18].
During stage 3
The control and experimental groups of nursing heads in NHSL Sri Lanka were separated by simple randomization. Then only the experimental group was exposed to a series of newly designed Leadership Skill Building Workshops based on the newly written manual. The total number of working hours was 22 (Table 1).
| Point |
Principle / competency |
Applications/ Skill Builders/ Tools/ Techniques |
| Point 01 |
Assertiveness |
Assertiveness Inventory |
| DESI Model |
| Assertiveness game |
| Pictorial analysis |
| |
| Point 02 |
Five Styles of Conflict Management |
Conflict Management Style Index |
| Techniques to apply conflict management styles in working place |
| Role play on the understanding link between assertiveness, cooperation and effective conflict management techniques |
| Point 03 |
Negotiation Skills |
Steps to achieve integrated negotiation |
| Strategies to negotiate with labour unions |
| Negotiate with peer leaders in implementing new projects |
| Negotiate with subordinates in grievance settlements |
| Role play on ethics in negotiation |
| Classic story |
| Point 04 |
Transactional Analysis |
Exploring own ego status |
| Apply change model to embed the Adult ego status |
| Role play- Life Positions |
| Demonstration-complementary transaction, crossed transaction, ulterior transaction |
| Pictorial display-Relationship between life positions, ego status and conflict management style |
| Sharing latest workplace conflict and replay with the application of transactional theory |
| Point 05 |
Patience and Tolerance |
Explore the Patience and Tolerance Index |
| Role Play- "There is no limit for the patients." |
| A classic story about patience |
| Point 06 |
Empathy |
Traits of an empathetic leader |
| Emotional Intelligence |
| Self-evaluating tool for empathy |
| Critical Incident |
| Point 07 |
Changing People without arising Resentment |
Apply nine recommendations of Carnegie to Workplace |
| Point 08 |
Ten Commandments of Human Relations |
Skill builder: freezing- unfreezing model to embedded ten recommendations in leaders |
| Total Working Hours - 22 hours of a nursing head. |
Table 1: Brief illustration of key elements of newly designed eight- point conflict management program for strengthening healthy organizational culture of major health.
Care facilities-stage 4
Post-interventional surveys, the last stage (stage 4) of the study was conducted by reapplying the HOC Description Questionnaire and competency index to both experimental and control groups following this intervention package.
Results
The quantitative measures of pre and post-interventional survey exhibit that there is a significant improvement of percentages of the higher levels of HOC, such as good and strong in the experimental group after the intervention. However, the levels of control group were poor or low during the study period (Table 2).
| Study Group |
Perceived Level of the strength of the parameter |
Dimensions of Healthy Organizational culture |
Level of the Perceived level of Healthy Organizational Culture |
| Leader’s attitude orientation toward theory Y |
Leaders behaviour between Consideration and Initiation Spectrum |
The degree of Leader- Subordinate Relationship |
| Number |
% |
Number |
% |
Number |
% |
Number |
% |
| Before Intervention |
| Experimental Group |
Poor |
20 |
43.48 |
18 |
39.14 |
19 |
41.30 |
22 |
47.80 |
| Low |
15 |
32.62 |
17 |
36.96 |
11 |
23.91 |
12 |
26.10 |
| Satisfactory |
9 |
19.56 |
9 |
19.56 |
14 |
30.43 |
10 |
21.70 |
| Good |
2 |
4.34 |
1 |
2.17 |
1 |
2.17 |
1 |
2.20 |
| Strong |
0 |
0.00 |
1 |
2.17 |
1 |
2.17 |
1 |
2.20 |
| Total |
46 |
100 |
46 |
100 |
46 |
100 |
46 |
100 |
| Control Group |
Poor |
19 |
41.30 |
17 |
36.96 |
21 |
45.65 |
21 |
45.60 |
| Low |
16 |
34.78 |
18 |
39.14 |
9 |
19.56 |
11 |
23.90 |
| Satisfactory |
10 |
21.70 |
8 |
17.39 |
14 |
30.43 |
11 |
23.90 |
| Good |
1 |
2.17 |
2 |
4.34 |
1 |
2.17 |
2 |
4.40 |
| Strong |
0 |
0.00 |
1 |
2.17 |
1 |
2.1 |
1 |
2.20 |
| Total |
46 |
100 |
46 |
100 |
46 |
100 |
46 |
100 |
| After Intervention |
| Experimental Group |
Poor |
3 |
6.52 |
2 |
4.34 |
1 |
2.17 |
2 |
4.40 |
| Low |
3 |
6.52 |
4 |
8.69 |
1 |
2.17 |
2 |
4.40 |
| Satisfactory |
10 |
39.14 |
9 |
19.56 |
10 |
21.70 |
10 |
21.70 |
| Good |
18 |
39.13 |
18 |
39.13 |
22 |
47.82 |
20 |
43.50 |
| Strong |
12 |
26.09 |
13 |
28.26 |
12 |
26.09 |
12 |
26.10 |
| Total |
46 |
100 |
46 |
100 |
46 |
100 |
46 |
100 |
| Control Group |
Poor |
20 |
43.47 |
18 |
39.13 |
21 |
45.65 |
19 |
41.30 |
| Low |
12 |
26.09 |
14 |
30.43 |
11 |
23.91 |
13 |
28.20 |
| Satisfactory |
8 |
17.39 |
10 |
21.74 |
9 |
19.56 |
9 |
19.60 |
| Good |
5 |
10.87 |
3 |
6.52 |
3 |
6.52 |
4 |
8.70 |
| Strong |
1 |
2.17 |
1 |
2.17 |
2 |
4.34 |
1 |
2.20 |
| Total |
46 |
100 |
46 |
100 |
46 |
100 |
46 |
100 |
Table 2: Frequency distribution of level of perceived level of healthy organizational culture and its dimensions before and after the newly designed Eight Point Conflict Management Interventional Program by experimental group and control group of nursing leaders in HSL.
Discussion
There is renewed interest in policymakers, health care managers and practitioners in the importance of developing organizational cultures in health care settings. Culture is a representation of values, beliefs and styles of employers, main stakeholders, employees of an organization [19-21].
Hospitals are high-risk organizations, where culture should ensure the quality and safety of patient care. Therefore, the survival and growth of hospitals rely on policies and practices towards strengthening towards best matching organizational cultures. The healthy organizational culture is the best suitable culture for the major curative center’s where leaders have to manage and maintain shared leadership styles with professionals, especially clinical experts. HOC is the fundamental culture that values human resource as the most critical assets of the organization [11,22]. Toxic organizational cultures are organizational cultures in which people feel that they are not valued and Healthy organizational cultures are ones in which people feel that they are valued [3]. HOC has dignity and critical importance given to employees in the organization by being the opposite of toxic organizational culture. HOC treats employees of the organization as the most important resource (at least one of the most important resources) and attempts to enhance employees’ wellbeing [23-25].
This study identified the multidimensional quantitative measurements to determine the level of HOC. This HOC Description Questionnaire consists of 3 main dimensions and 30 sub-dimensions, and it measures the leaders' perceived level of HOC of major curative settings [26-28]. The intervention package consisted of dimensions toward strengthening leadership competencies of leaders in curative setups; directors, clinical consultants and nursing leaders. Assertiveness, Five Styles of conflict management, Negotiation skills, Transactional analysis, Patience and Tolerance, Empathy, changing people without arising resentment and Ten commandments of human relations are the identified best possible competencies to develop HOC [29-31].
The study was conducted at the biggest tertiary care institute of Southeast Asia; National Hospital of Sri Lanka at the randomised controlled environment. The study population was limited to nursing leaders of the hospital due to time, technical and financial constraints.
The results showed a significant level of improvement of all three dimensions of HOC; leader's attitude orientation toward theory Y, leaders' behaviour towards consideration and initiation spectrums and the degree of leader-subordinate relationship. The computed value for satisfactory, good and excellent levels of HOC has improved from 26.1% to 91.3% following the intervention. The intervention took place within twenty-two working hours of the experimental group [17,32-34].
Conclusion and Implication
This interventional study was a success story of enhancing organizational culture among nursing leaders in The National Hospital, Sri Lanka. This framework can be adapted and researched in any other major health care institute. Further, medical administrators and clinical leaders are the other study groups to be targeted and tested.
The manuals had been developed to implement all eight competencies under the intervention. Those can be adapted to developing leadership curium of curative sector leaders following feasibility studies to establish the much healthier culture in the hospitals.
Further research should be developed to understand the values, attitudes and human relationship factors contributing to strengthening healthy organizational culture. The studies consisting of both quantitative and qualitative methods will fill the gaps seen in quantitative studies [35-37].
24038
References
- Eppard R (2004) Transformational and transactional leadership styles as they predict constructive culture and defensive culture.
- Greenberg (2007) Behavior in Organizations. (8thedn), Pearson Prentice Hal, New York.
- Opatha H (2015) What are key dimensions of a Healthy Organizational Culture?
- McGregor D (1957) Theory X and Theory Y;The Human Side of Management. In: Human side of enterprise.
- Tsai Y (2011) Relationship between organizational culture, leadership behaviors and conflict management theories.
- Longe O (2015) Impact of Workplace Conflict Management on Organizational Performance: A Case of Nigerian Manufacturing Firm. J Manage Strat 6.
- Alberti R, Emmons M (1995) Your Perfect right: A guide to assertive living, San Luis Obispo: Impact Publishers.
- Amernet (2010) Creating a culture of quality and patient safety-intalere.
- Akif L A, Futa MS (2013) The relationship between job stress and nurses performance in Jordanian. Asian J Business Manage 5: 267-275
- Sharma S (2010) Examining the relationship between organizational culture and leadership skills. Journal of the Indian Academy of Applied Psychology 36: 97-105.
- Scott T, Mannion R, Davies H, Marshell M (2003) The quantitative measurement of organizational culture in health care. Health Serv Res 38: 923-945.
- Opatha H (2015) Organizational Behaviour; The Human Side of Work (1st edn), Colombo: Feather Printing Service.
- Abramson J (2000) Survey Methods in Community Medicine: Churchill Livingstone. Am J Epidemiol 152.
- Bellou V (2008) Identifying organizational culture and subcultures within Greek public hospitals. J Health Organ Manag 22: 496-509.
- Nelson DL, Quiick JC (1997) Organizational behavior; human behaviour at work. New York: West Publising Company.
- Opatha H (2015) Organizational culture. In: organizational behaviour, the human side of work. Colombo: 549-550.
- Lober M (2012) Job Satisfaction of nurses and identified factors of job satisfaction. Croat Med J 53: 263-270
- Ghorbani M, Razavi N (2011) The study of the relationship between organizational culture and conflict management. Middle East J Sci Res 10: 711-714.
- Opatha H (2015) What are best possible tools, techniques and virtues to be practice by Leaders to Embedding a Healthy Organizational culture.
- Ng L, Johnson A, Nguyen H, Groth M (2014) Workplace culture improvements; a report of the workplace planning and development branch of the NSW Ministry of Health, Syndey: Ministry of Health, NSW.
- Timothy A (2004) The forgotten ones? The validity of consideration and initiating structure in leadership research. "J Appl Psychol 89: 36-51
- Umaserkaran (2010) Research methods for business. John Willey & Sons Ltd, United Kingdom
- Murray (2009) Module 4; Assertiveness Skill for the virtual workshop series and self-study program-training module.
- Mullins L (2011) Improving organizational performance. Management and organizational behavior (7thedn), Pearson Education Limited, England.
- Mackenzie (1995) Surveying the organizational culture in the public sector. J Healthc Manag 9: 69-77.
- Vauclair CM (2009) Measuring cultural value at the individual level; considering morality in cross cultural value research. Rev. Adm. Mackenzie 10: 3.
- Tsai Y (2011) Relationship between Organizational Culture, Leadership Behaviours and Job Satisfaction. BMC Health Serv Res 11: 98.
- Zazzali LJ, Alexandar AJ, Shortell MS, Burns RL (2007) Organizational culture and physicians satisfaction with dimensions of group practices HSR. Health Serv Res 42: 1150-1176.
- Gentry AW, Webber JT, Sadri G (2015) Empathy in the workplace; a tool for effective leadership. WHITE PAPER
- Graban (2012) Improving quality, patient safety and employee engagement (2nd edn),CRS press.
- Lwanga S (1991) Sample Size determination in health studies. Geneva: WHO.
- WHO (2009) Human Factors in Patient Safety, Geneva: World Health Organization.
- Mallak L, Lyth D, Oslan S (2003) Culture, the built environment and health care organizational performance. J Service Theory Prac 13: 27-38.

