Mohammad Reza Younesi1, Samira Louni Aligoudarzi2, Marzieh Lashgari3, Hoda mazaheri4, Mohamad Javad Tari4, Razieh Bigdeli4 and Vahid Asgary4,5*
1Hematology Department, Allied Medical School, Tehran University of Medical Sciences, Tehran, Iran
2Hematology Laboratory, Oncology Ward, Shariati Hospital, Tehran, Iran
3Biochemistry Laboratory, Imam Khomeini Hospital Complex, Vali-e-Asr Hospital, Tehran, Iran
4Research and Development Laboratory, Javid Biotechnology Company, Incubator of Pasteur Institute of Iran, Tehran, Iran
5Department of Immunology, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
*Corresponding Author:
Vahid Asgary
Research and Development Laboratory, Javid Biotechnology Company, Incubator of Pasteur Institute of Iran, Tehran, Iran
Tel: +982166176745
Fax: +982166976717
E-mail: vahid.asgary@yahoo.com
Received date: 27 May 2016; Accepted date: 15 June 2016; Published date: 18 June 2016
Citation: Younesi MR, Aligoudarzi SL, Lashgari M, et al. A Prospective Study of Serum Carcinoembryonic Antigen in Patients with Newly Diagnosed Colorectal Cancer and Healthy Individuals. Ann clin Lab Res. 2016, 4:2.
Keywords
Carcinoembryonic antigen, Tumor marker, Colorectal cancer
Introduction
Tumor markers are usually proteins or glycoproteins produced by the body in response to cancerous growth or by the cancer tissue that are possible to detect in serum, urine, or tissue samples. This group of protein is also observed in many healthy individuals, so it is not their presence in serum but their quantity that makes tumor markers useful (Park 2013) [1]. Carcinoembryonic antigen is a 200kDa glycoprotein produced during human embryo-fetal development, but the production of CEA after birth is considered as an abnormal sign that implicates malignancies especially colorectal cancer (CRC). The word "carcinoembryonic" or "oncofetal" antigen reflects the fact that CEA is produced by developing fetus and by some cancers (Beauchemin 2013, Kin 2013) [2,3]. Also CEA values can be elevated in benign conditions such GI infection, peptic ulcer, inflammatory bowel disease, pancreatitis, hypothyroidism, cirrhosis, biliary obstruction as well as in associated malignancies such as lung, gastric, medullary, thyroid, head and neck, cervical, and hepatic cancers, lymphomas and melanoma [4-7]. On the other hand, some studies have shown that in some cancers the incidence of CEA can predict the onset of the disease ahead of the clinical symptoms of the disease itself, and this observation is considered unique among some other laboratory tests [8]. In contrast, some studies have indicated that the measurement of serum CEA levels is not valuable in screening for any malignancy including colorectal cancer or in the diagnostic evaluation of an indeterminate disease [9]. CEA assay is an inexpensive and easy to perform test; however, repeated measurements to monitor disease, follow up and the response to therapy contribute to higher costs and increase laboratory workload. The aim of this study is to investigate the status of serum CEA values and evaluation of cigarette smoking, age and sex effects on elevated carcinoembryonic antigen levels among the apparently healthy individuals and patients with newly diagnosed colorectal cancer.
Material and Methods
Patients and samples
The data for this prospective study were collected during a period of three years between May 2011 and 2014 among cases in Tehran. Participants were selected from Tehran because the composition of its population represents a proper example for studies about the general Iranian public. Written consent was obtained from each participant, and the study was approved by the medical ethics committee of Tehran University of Medical Sciences. Inclusion criteria for healthy subjects included absence of infection and signing the approval form. In addition, the patients with early stage of colorectal cancer should provide complete medical history including laboratory tests and clinical examination documents signed by a physician with expertise in oncologic conditions. Exclusion criteria were as follows: incomplete blood draw or hemolyzed samples, subjects with a prior or current neoplastic disease or the presence of a serious disease of any other etiology apart from CRC. In our study, the specimens of 675 subjects including 414 females and 261 males referred to the above laboratory were obtained, and were subject to CEA serum level assay. In addition, 125 patients with colorectal cancer formed the other group. All the patients were in an early stage of CRC before and during the same drug regimen therapy.
Measuring CEA serum levels
Blood was obtained from the patients by venipuncture technique without any anticoagulant for serum, and the tubes were code-named to observe the anonymity of patients, and the serum was immediately prepared by high-speed centrifugation (2500 × g). After exclusion of two samples due to hemolysis, the quantitative measurement of serum CEA was performed on fresh serum samples by Radio Immuno Assay (Beckman Coulter/Immunotech), a highly sensitive and specific immunologic method of quantifying the concentration of an antigen in a solution that relies on a radioactively labeled antibody specific for the antigen. According to the manufacture guidelines, the upper limit of 5 ng/ml CEA concentration was accepted as normal, and the upper limit of 7 ng/ml was accepted for smokers.
Statistical analysis
Results were reported as mean ± standard deviation (SD) for quantitative variables and percentages for categorical variables. Obtained data of the study was analyzed by Statistical Package for Social Science (SPSS) software. Statistical independent t test was used to evaluate the significance of differences between groups in mean of continuous variables. P<0.05 was considered statistically significant. The upper reference values were defined as the 95 percentile of the normal values in each group.
Results
For inclusion in the study, a group of 800 cases (mean age 55 years, range 1-91) without any neoplastic disease other than CRC were potentially eligible.
Table 1 shows the distribution of CEA values was significantly higher in colorectal cases than apparently healthy cases (P<0.001).
| Groups |
Total No |
No: With
<5ng/ml |
No: With
5-7ng/ml |
No: With
>7ng/ml |
Average CEA level* |
cases
At Risk |
Significant difference# |
| Patients |
125 |
0 |
0 |
125 (100%) |
47 (ng/ml) |
125 (100%) |
- |
| Healthy individuals |
675 |
550 (81.48%) |
31 (4.58%) |
94 (13.92%) |
6.3 (ng/ml) |
125 (18.51%) |
Yes (P<0.001) |
| Smoker patients |
4 |
0 |
0 |
4 (100%) |
24 (ng/ml) |
4 (100%) |
Yes (P<0.01) |
Table 1: Comparison of CEA serum levels between patients, healthy individuals, smoker patients and smoker healthy individuals. (Significant difference is compared to patients groups).
Effects of smoking on the results of CEA are shown in Table 2. Statistical analysis shows that the level of CEA in smokers has increased significantly, compared to nonsmokers (P<0.05).
| |
Non smoker |
Smoker |
Significant |
| No. |
207 |
54 |
Yes (P<0.05) |
| CEA level average |
5.42 ng/ml |
11.32 ng/ml |
Table 2: Effect of smocking on CEA serum level in male healthy individual
Comparison among mean of CEA levels in three age groups including individuals with mean age under 30 years, between 30 and 60 years and upper 60 years old respectively as groups 1, 2 and 3 showed significantly elevated CEA levels in over 60 years individuals (P<0.05) (Table 3 and Figure 1).
| |
Total |
Lower than 30 years |
Between 30 to 60 years |
More than 60 years |
| No. |
675 |
48 |
352 |
275 |
| Male/Female |
261/414 |
19/29 |
129/223 |
113/162 |
| Average CEA level |
6.3 ng/ml |
4.8 ng/ml |
5.1 ng/ml |
8.1 ng/ml |
Table 3: Comparison of CEA serum levels between less than 30 years, between 30 and 60 years and upper 60 years old individuals.
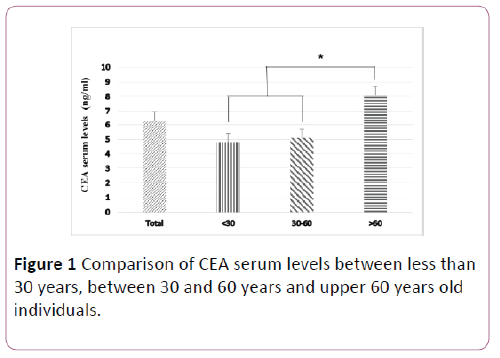
Figure 1: Comparison of CEA serum levels between less than 30 years, between 30 and 60 years and upper 60 years old individuals.
As shown in Table 4 and Figure 2, from a group of 261 healthy male subjects, 202 (39.77%) have CEA levels lower than 5 ng, 13 individuals (98.4%) have CEA levels between 5-7 ng and 46 (61.17%) have CEA levels more than 7 ng.
| Gender |
Total No |
No: With
<5 ng/ml |
No: With
5-7 ng/ml |
No: With
>7 ng/ml |
No. of cases
At Risk |
| Male |
261 |
202 |
13 |
46 |
59 (22.59%) |
| Female |
414 |
348 |
18 |
48 |
66 (15.24%) |
| Total |
675 |
550 |
31 |
94 |
125 (18.51%) |
Table 4: Effect of gender on CEA serum level in healthy individual.
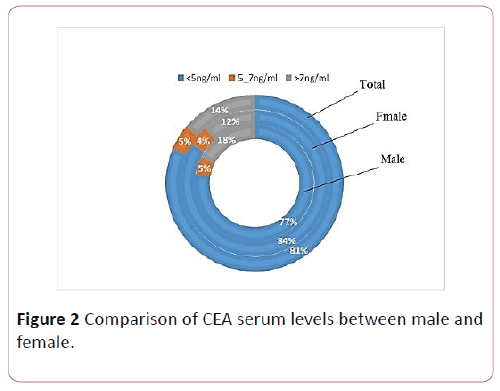
Figure 2: Comparison of CEA serum levels between male and female.
Also from a group of 414 female subjects, 348 (76.84%) have CEA levels lower than 5 ng, 18 (34.4%) have CEA levels between 5-7 and 48 (90.10%) have CEA levels more than 7 ng. Generally there is no difference between the CEA serum level in male and female subjects. In males and females, respectively, 59 (59.22%) and 66 patients (24.15%) are in the danger zone.
Figure 3 discusses the comparison of serum CEA levels between groups of healthy subjects over 60 years, healthy people who smoke, smokers with colorectal cancer and patients with colorectal cancer. The results show that serum levels in patients with colorectal cancer was significantly increased compared to the other three groups. It also shows that CEA in patients with colorectal smokers compared to healthy smokers and healthy people over the age of 60 is significantly higher. Statistically there is no also a significant difference between healthy smokers and healthy people over the age of 60 who smoke.
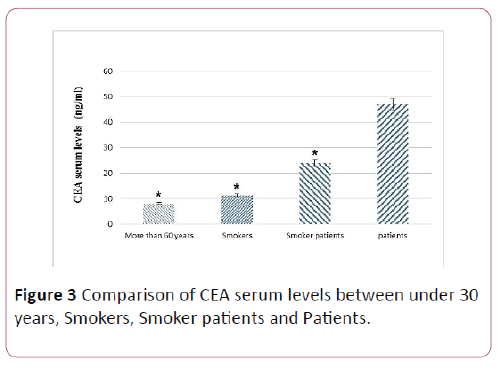
Figure 3: Comparison of CEA serum levels between under 30 years, Smokers, Smoker patients and Patients.
Discussion
Tumor markers are useful alarming tools when disease cannot be assessed, determined and firmly diagnosed by standard criteria. CEA is a tumor marker especially overexpressed in colorectal cancer, and there are many contradictory findings about sensitivity and usefulness of this tumor marker. It must be consider that assessment of CEA levels in serum has a major role in following and monitoring of patients for relapse after intended therapeutic program of CRC [8,10]. But there are several reports about unspecific elevated levels of CEA in apparently healthy smokers and elderly individuals or in some benign conditions such as liver and gastrointestinal system inflammations of any cause. Furthermore it is demonstrated that CEA serum levels increase in head and neck cancer, lung cancer, melanoma, lymphoma and many other malignancies [11-15]. Hence, there are contradictory findings and postulations about sensitivity, usefulness, diagnostic specificity and predictive value of CEA as a tumor marker.
In this study, we examined serum levels of CEA in patients with colorectal cancer and the results were compared with healthy subjects. For this experience, 125 patients who were newly diagnosed with colorectal cancer were examined and the results of the CEA levels were over 7 ng/ml. The average level of CEA in serum was reported to be 47 ng/ml in patients. This is while the 675 healthy subjects had a mean of 6.3 ng/ml and the average level of CEA in serum was normal and only 13.9% individuals from this group showed CEA levels of more than 7 ng/ml. In other words, these results suggest increased levels of CEA in the first stages of the disease and it can be used as an effective and rapid diagnostic tool, especially in the early stages. But the interesting thing is that the average CEA level in the serum of 13.9% health individuals were higher than 7 ng/ml, and 18.5% of individuals are in the danger zone. These results support the findings of several other studies reporting different factors causing high levels of CEA. So healthy subjects were divided in different groups of sex, age and smoking or non-smokers and then the level of CEA were examined. The result showed that, as in other studies, smoking increases the serum CEA levels in healthy individuals. We observed that the levels of CEA were higher in smokers group in comparison with nonsmokers in male. The results depicted that the level of CEA in smokers was 11.32 ng/ml, and that the CEA level in all smokers are in the danger zone, while in nonsmokers it is 5.42 ng/ml. But comparing the CEA levels in smokers with people who have the disease, shows that there is difference in the CEA levels between the two groups.
Also, in this study, healthy subjects were divided into three groups aging below 30 years, between 30 and 60 years and above 60 years and we observed that the average level of CEA in patients under 60 years were normal and equal to 5.1 ng/ml. However, the serum levels of CEA in patients above 60 years of age were higher than other people and increased to 8.1 ng/ml. Increased levels of CEA in these patients seems to be related to non-specific damage to various organs of the body due to aging [12]. The study also showed that gender has no effect on the level of CEA and that CEA levels in 77% and 84% of females and males, respectively, are in the normal range. Only 13% and 16% of females and males, respectively are in risk zone, which could be due to either age or because of smoking. Yet the latter cause in female population does not seem to be a major factor, as in the Iranian community, women rarely smoke. These results clearly show that when CEA is considered as a tumor marker, the patient's history related to smoking and age should be considered as well and when smokers or people aged higher than 60 are tested for levels of CEA, the threshold should be considered higher than normal. For both groups, the average level of CEA is higher than 7 ng/ml.
Conclusion
In general, this study showed that CEA serum level in addition to the colorectal cancer patients in elderly and cigarettes people also increases. It was also found that in smokers, especially smoking patients measuring CEA is not valuable. Amongst many contradictory results, the measurement of CEA is a useful method for screening, diagnosis; follow-up and treatment of CRC but Physiological influences that need to be considered in interpreting the results include effects of aging and smoking. Also other diagnostic tools, should be considered for patients with elevated levels of CEA, such as colonoscopy, chest, abdominal and pelvic CT scans and physical examination before treatment, because our findings indicate that many benign and malignancy conditions are associated with elevated CEA values, which may lead to misunderstanding of the CEA levels.
Acknowledgement
The authors are grateful to the people who worked in Hematology Laboratory of Shariati Hospital and Javid Biotechnology Company (JBC) for helpful assistance during the experiment. No sources of funding were used to assist in this study. All of the authors have declared that no competing interests exist.
9821
References
- Park Y, Kim YR, Hwang MS, Kim HS (2013) Evaluation on the Stability of Pooled Sera for External Quality Assessment of Tumor Marker Assays. Journal of Laboratory Medicine and Quality Assurance 35: 47-55.
- Beauchemin N, Arabzadeh A (2013) Carcinoembryonic antigen-related cell adhesion molecules (CEACAMs) in cancer progression and metastasis. Cancer and Metastasis Reviews 32: 643-671.
- Kin C, Kidess E, Poultsides GA, Visser BC, Jeffrey SS (2013) Colorectal cancer diagnostics: biomarkers, cell-free DNA, circulating tumor cells and defining heterogeneous populations by single-cell analysis. Expert review of molecular diagnostics 13: 581-599.
- Jones C, Badger S, Epanomeratikis E, McKie L, Diamond T, et al. (2012) Role of carcinoembryonic antigen as a marker for colorectal liver metastases. Br J Biomed Sci 70: 47-50.
- Sigari N, Mohsenpour B, Nikkhoo B, Ghaderi B, Afkhamzadeh A, et al (2014) Determination of the Best Prognostic Value of Serum Tumor Markers in Patients with Suspected Lung Cancer in an Iranian Population. Clin Lab 60: 23-27.
- Tada Y, Yoshikawa T, Sawada Y, Sakai M, Shirakawa H, et al. (2013) Analysis of cytotoxic T lymphocytes from a patient with hepatocellular carcinoma who showed a clinical response to vaccination with a glypican-3-derived peptide. Int J Oncol 43:1019-1026.
- Takeuchi Y, Shirai T, Sakurai S, Mikamo M, Fujii M, et al. (2013) Allergic bronchopulmonary aspergillosis presenting with a pulmonary mass mimicking lung cancer. Respirology Case Reports. 1: 5-7.
- Chen W, Liu Q, Tan S-Y, Jiang YH (2013) Association between carcinoembryonic antigen, carbohydrate antigen 19-9 and body mass index in colorectal cancer patients. Molecular and Clinical Oncology 1:879-886.
- Oliver AJ, Jimenez-Luna C, Melguizo C, Prados J, Caba O, et al. (2013) New Biomarkers for Colon Cancer Diagnosis: A Review of Recent Patents. Recent Patents on Biomarkers 3:110-119.
- Vargas GM, Sheffield KM, Parmar AD, Han Y, Brown KM, et al. (2013) Physician follow-up and observation of guidelines in the post treatment surveillance of colorectal cancer. Surgery. 154:244-255.
- Krzystek-Korpacka M, Diakowska D, Neubauer K, Gamian A (2013) Circulating midkine in malignant and non-malignant colorectal diseases. Cytokine 64:158-164.
- Lopez LA, Del VillarV, Ulla M, Fernandez F, Fernandez LA, Santos I, et al. (1996) Prevalence of abnormal levels of serum tumour markers in elderly people. Age and ageing 25:45-50.
- Ozeki N, Fukui T, Kawaguchi K, Ito S, Usami N, et al. (2013) F-082 Significance of serum carcinoembryonic antigen at the follow-up of completely resected non-small cell lung cancer. Interactive Cardio Vascular and Thoracic Surgery. 17 (suppl 1):S1-S62.
- Sajid KM, Chaouachi K, Mahmood R (2008) Hookah smoking and cancer. Carcinoembryonic Antigen (CEA) levels in exclusive/ever hookah smokers. Harm Reduct J 5:1-14.
- Sajid KM, Parveen R, Sabih D, Chaouachi K, Naeem A, et al. (2007) Carcinoembryonic antigen (CEA) levels in hookah smokers, cigarette smokers and non-smokers. J Pak Med Assoc 57:595-599.


