Keywords
Diabetes mellitus; Hyperglycemia; Metabolic disarray; Hypoglycemic agents; Herbal formulations
Introduction
A group of metabolic ailments exemplified through hyperglycemia termed as diabetes mellitus fallouts from deficiency in insulin discharge, insulin attainment, or equally [1]. Pancreas, positioned after the abdomen is an appendage where insulin is prepared. The pancreas hold bunch of cells named islets. Inside the islets, beta cells build insulin and liberate it into the blood (Figure 1) [2].
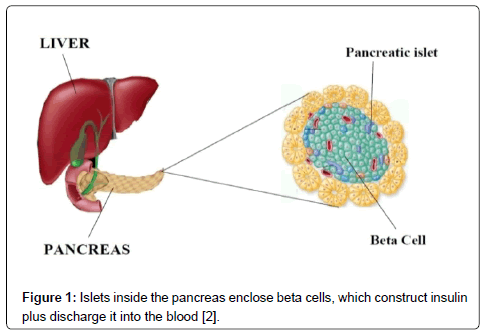
Figure 1: Islets inside the pancreas enclose beta cells, which construct insulin plus discharge it into the blood [2].
Glucose assembles up within the blood as an alternative of being captivated through cells inside the body if β- cells don’t generate adequate insulin, or the body doesn’t retort to the insulin that is there, directing to prediabetes or diabetes. Prediabetes is a form during which blood glucose intensity or A1C levels-which reveal normal blood glucose levels-are elevated than usual but not high enough to be analyzed as diabetes. In diabetes, the body’s cells be famished of vigor regardless of lofty blood glucose intensity [2].
Diabetes is provoked via as well as linked by means of metabolic impediment that can afterward escort toward untimely fatality [3]. The persistent hyperglycemia of diabetes be related by durable injury, dysfunction, as well as failure of diverse organs, mainly the eyes, kidneys, nerves, heart, and blood vessels [1].
Etymology
The terms "Diabetes" and “Mellitus” are derivative of Greek “Diabetes” denote "a passer throughout a siphon" while the "Mellitus" denotes "sweet". It is reflection that the Greeks name it so owing to the extreme amount of urine formed via diabetics attracted flies and bees [3].
Classification
Diabetes is deviated into two groups: type 1 diabetes and type 2 diabetes. A third type diabetes is Gestational diabetes, its occur only in pregnancy [2].
Type 1 diabetes (moderate generation of insulin) [4,5]
yyA lifetime (chronic) ailment with elevated intensity of sugar (glucose) in the blood [6].
yyThe production of insulin is faulty hence glucose cannot travel inside the cells [5].
yyType 1 diabetes is occurring at any age. Most often the disease is detected in children, teenagers or young adults [6].
yyThe rate of cell damage is somewhat inconsistent in this type of diabetes being hasty in some persons (chiefly infants and children) and deliberates in others (primarily adults). Several patients, mostly kids and youngsters may begin with ketoacidosis as the first symptom of the disease. Others comprise reserved fasting hyperglycemia that can speedily alter to stern hyperglycemia and/or ketoacidosis in the occupancy of disease or other strain [1].
Type 2 diabetes (weakened reaction to insulin or β-cell dysfunction) [4]
yyThe disease consists of a group of dysfunctions exemplified by hyperglycemia and ensuing from the mixture of resistance to insulin action, insufficient insulin secretion, and extreme or improper glucagon secretion [7].
yyGreatly frequent and accounts for 90-95% of all diabetes.
yyAdults are chiefly affected though newly Type 2 has commenced developing in kids.
yyThere is a sturdy connection between Type 2 diabetes, physical inactivity and fatness [5].
Gestational diabetes
yyA disease defined by glucose hypersensitivity of inconsistent sternness with beginning of initial identification in pregnancy.
yyHyperglycemia in pregnancy is found to be related through diverse motherly as well as prenatal undesirable outcome. Their offspring will contain a lifetime raise possibility of glucose fanaticism, stoutness plus metabolic disorder while the mother will contain an elevated threat of metabolic disorder and diabetes in the future [8].
Symptoms
a) Indistinct visualization [5]
b) Abnormal dehydration [5]
c) Recurrent urination [5]
d) Slow-healing incisions [5]
e) Baffling weariness [5]
f) Hasty mass loss (Type 1 diabetes) [5]
g) Erectile dysfunction [5]
h) Lack of sensation or itching in hands or feet [5]
Pathophysiology
Insulin is the key hormone to control the uptake of glucose from the blood into various cells of the body, chiefly liver, muscle, as well as adipose tissue. Therefore, its deficiency or the tactlessness of its receptors depicts a vital task in the entire type of diabetes mellitus. Beta cells (β-cells), found in the islets of Langerhans in the pancreas, release insulin into the blood in response to rising levels of blood glucose, typically after eating. About two third of the body's cells use insulin for glucose absorption from the blood for use as fuel, for conversion to other needed molecules, or for storage. Decreased insulin release from the beta cells and the breakdown of glycogen to glucose is an outcome of lower glucose levels. The hormone glucagon primarily controls this process, which acts in the converse manner to insulin. If the amount of insulin available is insufficient, if cells respond poorly to the effects of insulin (insulin insensitivity or insulin resistance), or if the insulin itself is defective, then glucose will not be absorbed properly by the body cells that require it, and it will not be stored appropriately in the liver and muscles. The net result is steadily elevated intensity of blood glucose, reduced protein synthesis, plus additional metabolic derangements, such as acidosis. while the glucose concentration in the blood vestiges elevated above time, the kidneys will achieve a portal of reabsorption, excretion in the urine (glycosuria) (Figures 2 and 3) [9].

Figure 2: Schematic diagram representing pathophysiology of type-1 diabetes [10].
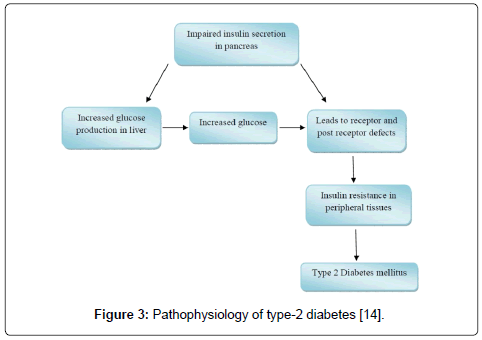
Figure 3: Pathophysiology of type-2 diabetes [14].
Etiology
Causes related to type-1 diabetes
i. Hereditary vulnerability: Genetics plays an essential part in determining who is likely to develop type 1 diabetes. Genes are passed down from biological parent to child. Genes carry instructions for making proteins that are needed for the body’s cells to function. Variations in genes that affect more than 1 percent of a population group are called gene variants (Figure 4) [1].
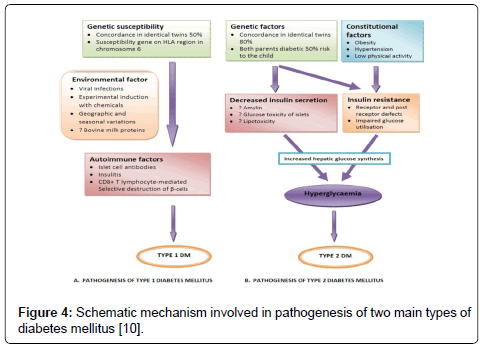
Figure 4: Schematic mechanism involved in pathogenesis of two main types of diabetes mellitus [10].
ii. Certain gene variants that carry instructions for making proteins called human leukocyte antigens (HLAs) on white blood cells are linked to the risk of developing type 1 diabetes. Some combinations of HLA gene variants predict that a person will be at higher risk for type 1 diabetes, while other combinations are protective or have no effect on risk [2].
iii. Autoimmune damage of Beta Cells: In this form of diabetes, T cells hit and demolish beta cells. The course of action starts well earlier than diabetes sign emerges and persists following identification. Type 1 diabetes is not identified frequently until major beta cells have by now been damaged. At this peak, an individual wants every day insulin therapy to stay alive [2].
iv. Ecological aspects: Ecological aspects such as foodstuffs, viruses and pollutants might play a part in the advancement of type 1 diabetes, although the precise character of their function has not been resolute. Few speculations propose that ecological features prompt the autoimmune damage of beta cells in people with a hereditary vulnerability to diabetes. Further hypothesis imply that ecological features play an enduring part in diabetes, yet subsequent to diagnosis [2].
Causes related to Type-2 diabetes
i. Hereditary vulnerability: Genes play a major piece in propensity to type 2 diabetes. Comprising definite genes or mixture of genes might augment or lessen a person’s danger for possessing the ailment. The role of genes is recommended by the elevated pace of type 2 diabetes in families and identical twins and extensive deviation in diabetes predominance through traditions. Learnings have revealed that variants of the TCF7L2 gene enhance vulnerability to type 2 diabetes [2].
ii. Fatness and Physical Sluggishness: Physical sluggishness and fatness are stoutly linked via growth of type 2 diabetes. When these hazardous features are nearby the people who are genetically susceptible to type 2 diabetes are more vulnerable. Difference among caloric ingestion along with physical activity can lead to fatness which cause insulin resistance and is frequent within public with type 2 diabetes. Fundamental heaviness, within which an individual have surplus abdominal fat, is a foremost hazard issue not merely for insulin resistance as well as type 2 diabetes however also for heart plus blood vessel ailment furthermore termed cardiovascular disease (CVD). This surplus “abdomen stout” produces hormones along with additional materials that be able to cause dangerous unremitting consequences inside the body like harm to blood vessels [2].
iii. Insulin Resistance: An ordinary situation in public who are heavy or overweight contain surplus abdominal fat, as well as are not bodily energetic. Muscle, fat, as well as liver cells impede reacting correctly toward insulin, forcing the pancreas to balance through generating superfluous insulin. Blood glucose intensity resides within the usual array, as long as β- cells are capable to generate adequate insulin. However, as insulin production wane since β- cell dysfunction, glucose intensity increases foremost to pre-diabetes or diabetes [2].
iv. Irregular Glucose Production through the Liver: An abnormal increase in glucose production by the liver also contributes to high blood glucose levels in some people with diabetes. Generally, the pancreas discharges the hormone glucagon when blood glucose as well as insulin intensity is small. The liver is stimulated by glucagon and produces glucose which is released into the bloodstream. Glucagon levels drop, when blood glucose and insulin levels are high after a meal and the liver stores surplus glucose intended for later, as needed. In several populaces with diabetes, glucagon intensity resides elevated than required. Elevated glucagon intensity cause the liver to generate unwanted glucose, which throw in to elevated blood glucose intensity [2].
Complications
Acute [10,11]
a) Diabetic ketoacidosis
b) Hyperglycemia hyperosmolar state
c) Hypoglycemia
d) Diabetic blackout
e) Erectile Dysfunction
f) Respiratory contagion
g) Periodontal sickness
Chronic [12]
a) Diabetic retinopathy
b) Diabetic nephropathy
c) Diabetic neuropathy
Diagnosis
Following tests are employed in diagnosing of diabetes:
a) Random plasma test: This is the simplest test that requires no fasting prior to the test. Blood glucose of 200 or more than 200 mg/ dl possibly specify diabetes but have to be confirmed again [12].
b) Fasting plasma glucose test: The test requires eight hours fasting. More than 126 mg/dl blood glucose on two or more tests carried out on diverse days confirm a diabetes diagnosis [12].
c) Oral glucose tolerance test: This test is carried out when random plasma glucose test is 160-200 mg/dl and the fasting plasma test is 110-125 mg/dl. This blood test estimates body’s response to glucose is estimated. Fasting of at least eight but not more than 16 hrs is required in this test. Fasting glucose intensity is resolute furthermore provide 75 gm of glucose, 100 gm for pregnant women. Every 30 minutes to one hr for two or three hrs the blood is tested. If the glucose level at two hrs is less than 140 mg/dl, then this test is normal. A diabetes diagnosis is confirmed with the fasting level of 126 mg/dl or greater and two-hour glucose level of 200 mg/dl or Higher [12].
d) HbA1C (A1C or glycated hemoglobin test): This test can be used for the diagnosis of both prediabetes and diabetes. Average blood glucose control for the past 2 to 3 months is measured. Moreover, this test is more convenient as no fasting is required. When the A1C is 6.5% or higher, diabetes is diagnosed [13,14].
e) Fructosamine test: The main component of plasma proteins is albumin. Since albumin too includes open amino clusters, nonenzymatic response among glucose within plasma occurs. Thus, glycated albumin be able to equally serve up like a indicator to examine blood glucose. Glycated albumin is generally taken to present a fair measure of regular blood glucose concentration greater than a time of 1 to 3 weeks [12].
Management
Diabetes mellitus being a persistent ailment for which there is no identified treatment excluding very explicit situation. Maintaining blood sugar levels since close toward normal being the attention towards management, exclusive of causing stumpy blood sugar. This be able to generally consummate by means of a well diet, work out, mass loss, along with employment of suitable drugs (insulin during the case of type 1 diabetes; oral drugs, as well as probably insulin, during type 2 diabetes) [9].
Apparently, the cornerstone in the management of diabetes mellitus is life style. In the prevention of diabetes and cardiovascular disease life style management is recognized as being an essential part. The dietetic managing of diabetes mellitus being an accompaniment of lifestyle management and has a affirmative result on long term fitness along with quality of life. Dietetic managing seeks on best metabolic control with creating equilibrium among food ingestion, bodily motion in addition to medicine in the direction of evading problems. The dietary objective in type 2 diabetes is for improved glycemic and lipid levels and weight loss as appropriate [3].
Treatment
Medicines employed to extravagance diabetes act consequently through lessening blood sugar levels. Here are a number of diverse classes of anti-diabetic medicines (Figure 5) [9].
a) Action on pancreas through jamming K+ ions in β-cells to stimulate insulin emission: Meglitinides, Sulphonylureas.
b) Reduce Gluconeogenesis by action on liver: Biguanide and Thiazolidine diones.
c) Action on muscle along with adipose tissue to enhance marginal glucose uptake: Biguanide Metformin.
d) Insulin sensitivity is augmented through activation of receptors: Thiazolidine diones.
e) Delays glucose absorption by acting on intestine: α-glucosidase inhibitors.

Figure 5: Diagram depicting different physiological target of synthetic drugs [15].
Herbal Treatment for Diabetes
Herbal drugs have been employed from the time of the beginning of human beings on this earth and as a consequence is approximately as old as time itself [15]. Even though here are numerous synthetic medications designed for patients, however it is the reality that it has in no way been account that someone had recovered completely from diabetes. The present oral hypoglycemic agents generate adverse consequence. Therefore, during the recent times great consideration have been aimed on the antidiabetic potential of therapeutic foliage plus their herbal formulation in the management of ailment [16]. Substitute to these synthetic agents various herbal plants with hypoglycemic assets are identified since crosswise the planet. 21,000 plants have been listed by the World Health Organization (WHO), which are utilized for therapeutic rationale around the world [17-24]. Several therapeutic plants with possible antidiabetic actions accounted with their promising mode of action have been listed below (Table 1) [16].
| Botanical Name |
Common Name |
Part Used |
Active Constituent |
Mode of Action |
| Aegle marmelos [16] |
Bael[18] |
Leaf[19] |
Aegelin[24] |
Augments consumption of glucose each via straight stimulation of glucose uptake otherwise via the arbitration of improved insulin discharge and have strong antioxidant activity, which can account for the hypoglycemic potential [16] |
| Allium cepa [16] |
Onion[20] |
Bulb[21] |
Quercetin[24] |
Lessens oxidative strain as well as conserve pancreatic beta cell reliability[24] |
| Azadirachta indica [23] |
Neem[22] |
Leaf and bark[23] |
Quercetin, rutin, and nimbidin[23] |
β cells rejuvenation[16] |
| Brassica juncea [16] |
Indian mustard[24] |
Seed [24] |
Isothiocyanate glycosidesingrin[15] |
Hepatic glycogen and glycogenesis mass is increased and the activity of glycogen phosphorylase and gluconeogenic enzymes is repressed, directs the reduction in glycogenolysis and gluconeogenesis[16] |
| Cajanus cajan [20] |
Pigeonpea[21] |
Leaves[21] |
Two globulins, cajanin and concajanin[20] |
Plasma glucose extent is lowered[16] |
| Eucalyptus globules [22] |
Blue gum[23] |
Leaves[22] |
Polyphenols,proanthocyanidins, anthocyanins[22] |
Hamper α-glucosidase[23] |
| Aloe vera [24] |
Aloe[25] |
Gel from leaves[25] |
Barbaloin[26] |
Stimulate production and/or discharge of insulin from pancreatic beta cells[17] |
| Catharanthus roseus [16] |
Madagascar periwinkle[17] |
Leaf[16] |
Indole alkaloid (vincristine)[15] |
Raise mobilization of glucose [16] |
Cryptolepis
Sanguinolenta [15] |
Anantmul [15] |
Stem[18] |
Cryptolepine[15] |
Glucose uptake is enhanced by 3T3-L1 cells[15] |
| Olea europia [15] |
Olive[15] |
Leaf [19] |
Oleuropeoside [15] |
Potentiates glucose, stimulation of insulin discharge and escalates peripheral uptake of glucose[15] |
Table 1: Herbal plants possessing antidiabetic activity with their mode of action.
Polyherbal Formulation for Diabetes
Dihar
•A polyherbal formulation holding eight diverse herbs Syzygium cumini, Momordica charantia, Emblica officinalis, Gymnema sylvestre, Enicostemm, Azadirachta indica, Tinospora cordifolia and Curcuma longa.
•Literatures revealed that combination of these eight herbs shows effective Anti-hyperglycemic activity in Streptozotocin (STZ,45 mg/kg iv single dose) induced type 1 diabetic rats.
Diasol
•Holds plant extracts of Eugenia jambolana, Foenum graceum, Terminalia chebula, Quercus, infectoria, Cuminum cyminum, Taraxacum officinale, Emblica officinalis, Gymnea sylvestre, Phyllanthus nerui and Enicostemma littorale.
•Previous investigation showed Diasol produced 63.4% reduction of blood glucose level in a dose of 125 and 250 mg/kg b.w i.p and proved to be effective antidiabetic polyherbal formulation.
Dia-Care
•Containing Sanjeevan Mool; Himej, Jambu beej, Kadu, Namejav, Neem chal is a herbal formulation alleged to be efficient for together Type 1, Type 2 diabetes surrounded by 90 days of treatment and heals within 18 months.
•With 1/2 glass of water, approx. 5 grams (1 tea spoon) powder is blend stirred well set aside overnight and filtered. The filtrate is taken in the morning on empty stomach.
Diabeta
•A formulation obtainable in the capsule type is an anti-diabetic among mixture of verified anti-diabetic equipped with strong immunomodulators, antihyperlipidemics, anti-stress and hepatoprotective of plant source include Gymnema sylvestre, Vinca rosea, Curcuma longa, Azadirachta indica, Pterocarpus marsupium, Momordica charantia, Syzygium cumini, Acacia arabica, Tinospora cordifolia, and Zingiber officinale.
Karmin plus
•Holds Momordica charantia, Azadirachta indica, Picrorrhiza kurroa, Ocimum sanctum and Zinziber officinale is a local polyherbal formulation.
•Banger et al. estimated its antidiabetic action and established that on two dosage stage by 200 mg/kg and 400 mg/kg body weight product confirmed efficacy for antidiabetic action [16].
Conclusion
In recent years, diabetes has become a major health problem worldwide, affecting people across all ages, sex, ethnicities, and races, and its prevalence has been increasing at an alarming rate. The associated complications of synthetic drugs have lead to a shift towards locating natural resources showing anti diabetic activity. Thus, many different plants have been used individually or in formulations for treatment of diabetes and its complications. The above-mentioned plants have been considered for their possible hypoglycemic actions and the researchers have carried out some preliminary investigations. It is important to know the active component and their molecular interaction, which will help to analyze therapeutic efficacy of the product and also to standardize the product. Efforts are now being made to investigate mechanism of action of some of these plants using model systems.
Conflict of Interest
The authors declare that there is no conflict of interest.
Acknowledgements
I take this privilege and pleasure to acknowledge the contributions of many individuals who have been inspirational and supportive throughout my review undertaken and endowed me with the most precious knowledge to see success in my endeavor. My review bears the imprint of all those people.
20405
References
- Diagnosis and Classification of Diabetes Mellitus (2004) American Diabetes Association Diabetes Care 27: S1.
- Causes of Diabetes, National Institute of Diabetes and Digestive and Kidney Diseases.
- Piero MN, Nzaro GM, Njagi JM (2015) Diabetes mellitus-a devastating metabolic disorder. Asian Journal of Biomedical and Pharmaceutical Sciences 5: 1.
- Lin Y, Zhongjie S(2010) Current views on type 2 diabetes. Journal of Endocrinology 204: 1-11.
- Type 2 Diabetes Mellitus: Practice Essentials, Background, Pathophysiology.
- Cheung KW, Wong SF (2013) Gestational diabetes mellitus update and review of literature. Reproductive System & Sexual Disorders.
- Baynes J (2015) Diabetes & MetabolismClassification, Pathophysiology, Diagnosis and Management of Diabetes Mellitus Diabetes Metab6:5
- Ozougwu JC (2013) The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. Journal of Physiology and Pathophysiology 4: 46-57.
- Chawla R, Thakur P, Chowdhry A, Jaiswal S, Sharma A, et al. (2013) Evidence based herbal drug standardization approach in coping with challenges of holistic management of diabetes: a dreadful lifestyle disorder of 21st century. Journal of Diabetes & Metabolic Disorders 12: 35.
- Srivastava S, Lal VK, Pant KK (2012) Polyherbal formulations based on Indian medicinal plants as antidiabetic phytotherapeutics. Phytopharmacology 2: 1-15.
- Dwivedi C, Daspaul S (2013) Antidiabetic herbal drugs and polyherbal formulation used for diabetes: A review. J Phytopharmacol 2: 44-51.
- Sabu MC, Ramadasan K (2004) Antidiabetic activity of Aegle marmelos and its relationship with its antioxidant properties. Indian Journal of Physiology and Pharmacology 48: 81-88.
- Shibly AZ, Zohora FT, Islam MS, Islam MR (2015) A comprehensive review on ethno pharmacological antidiabetic potential of traditional ayurvedic plants of Bangladesh. Journal of Pharmacognosy and Phytochemistry,p: 4.
- Satyanarayana K, Sravanthi K, Shaker IA, Ponnulakshmi R (2015) Molecular approach to identify antidiabetic potential of Azadirachtaindica. Journal of Ayurveda and Integrative Medicine 6: 165.
- Maity P, Hansda D, Bandyopadhyay U, Mishra DK (2009) Biological activities of crude extracts and chemical constituents of Bael, Aegle marmelos (L.) Corr. Indian J ExpBiol 47: 849-861.
- Sunarwidhi L, Anggit L, Sudarsono S, Agung EN (2014) Hypoglycemic effect of combination of Azadirachtaindica A. Juss. and Gynuraprocumbens (Lour.) Merr. ethanolic extracts standardized by rutin and quercetin in alloxan-induced hyperglycemic rats. Advanced Pharmaceutical Bulletin 2: 613.
- Arumugam G, Manjula P, Paari N (2013) A review: Anti diabetic medicinal plants used for diabetes mellitus. Journal of Acute Disease 2: 196-200.
- Pal K, Dilipkumar R (2011) Biological activities and medicinal properties of Cajanuscajan (L) Millsp. Journal of Advanced Pharmaceutical Technology & Research 2: 207.
- Birjatinder S, Sarabjit K (2012) Review of Cajanuscajan as important medicinal plant. International Journal of Natural Product Science 1:140.
- Dey K,Baishakhi L, Analava M (2013) Chemo-profiling of eucalyptus and study of its hypoglycemic potential. 4: 170-176.
- Bunyapraphatsara N (1996) Antidiabetic activity of Aloe vera L. juice II. Clinical trial in diabetes mellitus patients in combination with glibenclamide. Phytomedicine 3: 245-248.
- Patel DK, Patel K, Tahilyani V (2012) Barbaloin: a concise report of its pharmacological and analytical aspects. Asian Pacific Journal of Tropical Biomedicine 2: 835-838.
- Ajayi AF (2012) Effect of ethanolic extract of Cryptolepissanguinolenta stem on in vivo and in vitro glucose absorption and transport: mechanism of its antidiabetic activity. Indian Journal of Endocrinology and Metabolism 16: 91.
- Eidi A, Eidi M, Darzi R (2009) Antidiabetic effect of Olea europaea L. in normal and diabetic rats. Phytotherapy Research 23: 347-350.


