Keywords
Skill-birth attendants; Bangladesh; Health system
Introduction
Bangladesh is a socio-ecologically vulnerable country, which has made some visible progress in the health sector, but is still struggling to improve its health status to keep pace with rapid global changes including climate change and extreme events. With a small land area of 50,260 sq. miles, Bangladesh is now ranked as the eighth most densely populated country in the world with about 163 million people with 43.9% of them being women of reproductive age (15-49 years). Presently, Bangladesh faces an MMR of 176 deaths per 100,000 women [1]. After Sub-Saharan Africa, Bangladesh has the highest MMR (Maternal mortality Rate) in the world and continues to face the challenges of pre- and post-natal care, malnutrition, low access of skilled birth attendants (SBAs) [2]. To get access to proper maternal health care is still challenging and is influenced by many factors, including social, political, economic, cultural and religious ones, gender perspective and the country’s health system itself. Poor care during pregnancy, delivery and after birth not only enhance the risk of child death and maternal death, but also the reasons for severe diseases and disabilities among the mothers, reasons which include uterine prolapse, pelvic inflammatory disease, fistula, incontinence, infertility, and pain during sexual intercourse [3]. Most of these events could be prevented by ensuring access to elementary care by an SBA [4,5].
Skilled birth attendants (SBAs)
Skilled birth care during and after the childbirth could help to reduce the risk and help to decrease maternal, something mortality which has been recognized worldwide. According to WHO [6] an SBA is “an accredited health professional – such as a midwife, doctor or nurse – who has been educated and trained to proficiency in the skills needed to manage normal (uncomplicated) pregnancies, childbirth and the immediate postnatal period, and in the identification, management and referral of complications in women and newborns”. The definition given Graham [7] emphasized the processes and environment that are required for an SBA, which includes sufficient supplies, materials and set-up as well as proficient and active systems of communication and referral. Moreover, that report critically analysed the ‘environment’ and found it to largely embrace the social, political and cultural context that an SBA needs to operate and the immediate factors which influence maternal care by the SBA such as training, health system management and financing.
Problem statement
Birth attendance by SBAs is considered as the “single most important determinant in preventing maternal deaths” [8]. Some progress has been seen in the increasing use of antenatal care and in the field of maternal mortality, but still Bangladesh is far away from the target of international development. SBA during delivery is 42.1%, which is still quite low, according to the global standard, which needs to be a minimum of 50% [9]. Home delivery is the tradition of Bangladesh; 62.2% of total births still take place at household level and 48.2% children are born with the help of a traditional birth attendant (TDA). Less than one third of women giving birth were attended by doctors (Figure 1) [9]. So, it is clear that a majority of women could not get access to SBAs and they rely on TBAs. These are threats to maternal health. With the high population, calculations based on this trend have shown that 124,392 women are at still risk for birth related mortality each year in Bangladesh.
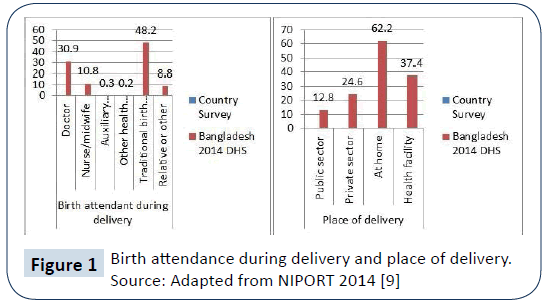
Figure 1: Birth attendance during delivery and place of delivery.
Source: Adapted from NIPORT 2014 [9]
The above scenario clearly indicates that the health system of Bangladesh is dysfunctional in giving access to adequate and effective maternal health care by SBAs. This study will analyse the issues by applying the WHO Health System Six building blocks Framework along with other factors and making strategies (recommendations) for policy, development and practice.
Key Issues Regarding access to SBAs in Bangladesh Health System
Finance
Bangladesh has a very explicit downward trend in health expenditure which decreased by almost half to 28.1% in 2014, down from 43.02% in 1997, and along with this, it has experienced a marked upward trend in out of pocket health expenditure which rose to 66.84%, sixth highest in the world [1]. According to WHO, the annual allocation for health services per head should be BDT 2,652, whereas in Bangladesh it is BDT 390? So, it is clear that, health care seeking behaviour has become more expensive for Bangladeshi. Koenig [10] state that in both urban and rural areas in Bangladesh the main cause for deteriorating maternal health care seeking behaviour is a concern for excessive medical costs.
Moreover, there are some unpredictable and uncountable costs such as hospital fees, corruption (which is the demand known as under-the-table payment), and medical supplies which bring additional financial pressure among the families to get access to the SBAs [10-12]. These all drive the poor away from accessing an SBA and to seeking the TBA whose services seem affordable.
In contrast, the poor and unacceptable SBA’s salary, delayed salary, less opportunity for promotion and lack of inspiration in the system, all led the SBAs to be demotivated and suffer from job unsatisfaction which may affect the outcome of the service [13]. The SBAs may try to take other opportunities in private and international organizations to get better salaries as well as for other facilities that public hospitals do not offer. So, in the public health care sector, there is scarcity of SBAs. On the other hand, in the private health care sector, poor people could not get access to them because of the expensive service.
Governance and Leadership
The stewardship is the most important and compound building block in the health system where the responsibilities, policies and coordination of government with other actors directly impact on health [14]. The success or failure of a country’s health system depends on it. According to World Bank [1] health expenditure as a percentage of GDP from 2011 to 2014 was 3.156%, 3.081%, 2.883% and 2.819% respectively; highest in South-East Asia [15]. This trend clearly shows why there is no sustainable, well defined and strategic policy path in maternal health. Moreover, health care infrastructure varies between urban and rural areas where private sectors are predominantly leading the maternal health care in metropolitan areas which creates explicit inequity in having the opportunity to access maternity services between the urban and rural, and between poor and rich [16]. Because, private sectors offer somewhat better maternal care than public, but those are questions for affordability. So, accessibility of SBAs extremely varies on wealth quantile between both poor and rich (poor vs. rich 5% vs. 51%) and rural and urban areas (rural vs. urban: 13% vs. 37%) in Bangladesh [15-17].
Better access to SBAs was one of the priorities of MDGs and SDGs. To accelerate the progress in achieving MDG 5, Bangladesh adopted a number of strategies such as training a new cadre known as Community Based Skilled Birth Attendants (CSBAs) and also training the Traditional Birth Attendants (TBAs) to get access to SBA [12,13,18,19]. But there is a scarcity of policy and regulation for CSBAs; for which there is no functional mechanism existing in the governance such as no fixed job responsibilities, working hours, leave policy, incentive system, nor are they well equipped and there is a huge lack of supervision and monitoring [13]. So, the inability of the government to provide sincere, focused and well guided leadership regarding CSBAs is about the quality and effectiveness of the service regarding skilled maternity care is questionable.
Human resources
Health Resource for Human (HRH) is an important determinant and factor for measuring health outcome for maternal health and MMR [20,21]. Bangladesh has been found to be one of the 58 crisis countries with the critical shortage of HRH/ health service providers (doctors, nurses and midwives) [22]. Bangladesh has one of the worst nurse-physician ratios, only one nurse per three physicians, a scenario which is the inverse of the World Health Organization’s recommendation in a well-functioning health care system [23]. Additionally, the number of nurses and midwives is falling sharply; the latest data found in 2011 was 0.22 in per 1000 people [1]. Approximately 3 million births take place yearly in Bangladesh and a 20% rise of institutional delivery means that at least an extra 600,000 deliveries need to be conducted at the health facilities [24]. In general, the present health facilities in Bangladesh are not ready to handle these large numbers of deliveries with SBAs. Along with the crisis of SBA, there is the hugely inequitable distribution of the skilled health care providers where the tendency for them to work more in the urban areas rather than rural areas [25]. As a result, the availability to get access to SBA is much more difficult in rural areas.
Medicines and Technologies
Scarcity of medicines and supplies are very common in health services. Most of the time, system does not provide adequate medicines and supplies; for example, oxytocin, antibiotics and expendables such as sutures and gauze. This list is often given to the family to buy from the outside pharmacy which is an extra economic load for the family. The fundamental cause of the scarcity of supplies and equipment is the lack of sustainable funding [13].
SBAs who attending home deliveries have only some basic instruments and medicines because of scarce supplies. If they are missing additional tools and supplies to support a delivery, they need to refer the patient to the health centre. This delay can sometimes be the cause of maternal mortality [18]. So, access to well-equipped quality SBAs’ care is very limited in Bangladesh.
Information
There is a poor linkage in between both Directorate Generals of Health and Family Planning services at the marginal and central levels, although both provide summarized data to the Ministry of Health and Family Welfare regularly [25]. Moreover, there is also little coordination with the national statistics office and the Bangladesh Bureau of Statistics (BBS). Assessment of the general development in improving maternal health in Bangladesh (and elsewhere) has been hampered by the lack of appropriate data as the Demographic and Health Surveys (DHS) provide valuable, but usually inadequate data regarding maternal health behaviour related to antenatal and delivery care [10]. Information distribution through monitoring and evaluation is crucial for policy formulation and regulation and also important for sharing with the people to be aware of their rights, the maternal care available in their locality, the process for accessing SBAs.
Service delivery
According to WHO [14], “In any health system, good health services are those which deliver effective, safe, good quality personal and non-personal care to those that need it, when needed, with minimum waste”. This is the fundamental responsibility of SBAs in the health system. Though service delivery fully depends on the other building blocks in the health system such as financing, workforce and governance and leadership. The priority aims in service delivery are establishing and dealing with inputs and the facility to confirm appropriate access, quality and safety of care in terms of all places, time and classes. Researchers such as Bhuiyan [26] stated that there are not sufficient SBAs available in the rural level, sometimes SBAs could not attend the emergency services.
The quality of maternal service delivery relies on some basic concerns such as scarcity of SBAs, excessive patients pressure, which leads to over workload, training, monitoring, insufficient logistics and laboratory support and not following the protocols [27]. These decrease morality and ability to provide quality care. For example, this study noted from the perceptions of different maternal and child health care providers that they mentioned they did not receive any further training to improve their skills after their graduation and they also mentioned that there is no upper level supervision to monitor their work, something which could improve their quality of service delivery for the patients.
Other challenges
Accessing the maternal health care from SBAs faces also some other several challenges in Bangladesh which need to be tackled. These barriers are different social, cultural, religious, traditional beliefs and perceptions of maternal care to SBAs which mainly result of illiteracy and gender discrimination. For instance, Bangladeshi women are highly depended on their husband and mother-in-law for suggestions and permission regarding their daily activities, finance, food and health care [19]. These also motivated them to rely on traditional medicines and spiritual healers, especially for postpartum care. Dysfunctional communication mainly in remote areas regarding poor road construction and lack of proper transportation also prohibits them from seeking skilled maternal care [28].
Proposed strategy on Governance
This study tries to propose a strategy below (Table 1) of governance and leadership block within the health system. Potential governance is a vital factor in making the whole health system function [29]. This study has used the ‘Health Sector Governance Model’ from Brinkerhoff and Bossert (2008) [30] to divide the strategies into 3 groups of main actors: the state (such as politicians and policymakers), health providers (such as public, private and all levels health sectors) and the citizens (such as service users and the public) in two main columns entitled ‘Strategies to address bottlenecks’ and ‘Proposed activities’. The objective of this framework is to show the pathway to improve accessibility of SBA in Bangladesh through governance bottleneck of health system to improve availability, equity, and affordability, safe and quality maternity care in Bangladesh. Through the lens of governance and leadership this study tried to make strategy to contribute and influence other five building blocks in the health system. This study is recommending the strategies under the state level are to ensure strong policy formulation and regulations, adequate funding, infrastructure, action on corruption regulation and proper advocacy; in providers level proposed strategies are to establish strong management and procurement and at the citizen level suggested approaches are to increase education for knowledge, awareness and behaviour change activity. Monitoring and Evaluation throughout every sector are crucial to follow up the activities, outcomes, strengths and weakness of the system as lesson learning to improve accessibility of SBA in Bangladesh.
M
O
N
I
T
O
R
I
N
G
&
E
V
A
L
U
A
T
I
O
N |
Strategy for governance and leadership (Recommendations) |
| Objective: Improve accessibility of SBA in Bangladesh |
| Desired Outcomes: Availability, Equity, Affordability, Safe and Quality maternity care in Bangladesh |
State level
(Example: Politicians and Policymakers such as Health Ministry, Finance Ministry, Elected officials and Governance) |
| Strategies to address bottlenecks |
Proposed activities (Recommendations) |
| Strong Policy formulation and regulations for access to SBAs for maternity and antenatal health care |
Adequate SBAs recruitment
Regular training and regular refreshment
Clear role and responsibility among the SBA
Appropriate salary, other features: incentives, adequate leaves, working hour in terms of job satisfaction
Appropriate proportion of health workers according to demand and population of an area (rural and urban level)
Free maternal care by SBAs without any disparity
Prioritize universal access to essential health care package targeted on maternal care |
| Adequate funding/ fundraising for health system |
Increase health budget and expenditure on maternal health care
User free maternal care for the poor people |
| Infrastructure |
Proper establishment of health care facilities and distribution of SBAs in rural and urban areas
Improving communication by proper road construction and transportation arranged for the delivery period |
| Corruption regulation |
Strong policy regulation to prohibit corruption in different sector levels (from up to down in the hierarchy of health system).
No payment under the table or extra charge for maternal care |
| Advocacy |
Reliable and adequate information collection on maternal health status and health services for policy formulation, regulation and knowledge sharing with the people. |
Provider levels
(Example: Public, private and all levels health sectors) |
| Strong Management |
Strong management in the provider levels such as in a hospital or health center regarding activity of the health workers, quality control for maternal health care with robust supervision |
| Proper procurement |
Available supplies of medicine and other maternal delivery tools for normal and critical deliveries in the health centres
Adequate medicine and materials need to supply to SBAs regularly
Ensure regular supply chain management for the medicine and other materials to SBAs for the delivery |
Citizen levels
(Examples: Service users, the public, rural and urban, rich and poor) |
| Education for knowledge, awareness and behaviour change activity |
Information sharing as maternal health care promotion, mass media communication and campaigning
Community education for basic understanding of maternal care, utilization, benefits and process of access to SBA
Knowledge on misconception and perceptions such as social, cultural, religious, gender discrimination. For example, women need to be active decision-makers on when they choose to access the SBAs and to be able to reach and afford the care provided, sometimes rapidly during an emergency |
Table 1 Strategy for improving Governance and Leadership to the accessibility of SBA in Bangladesh.
The limitation of this study is, this only focused on some specific critical issues and tried to develop a strategy based on those to increase easy accessibility to SBAs in Bangladesh. This study is just one of many critical reasons and essential initiatives towards the overall development and accessibility of maternal care by SBAs in Bangladesh.
Conclusion
The table outlines a strategy to strengthen the fundamental blocks governance and leadership in the health system. As a final point, to access SBAs regarding maternal health, the health systems cannot perform without having strategic governance and leadership. To summarize the given strategy, the Bangladesh government need to take strong initiatives to revise their policies, regulations and strategies to make efficient and effective health system. In addition, proper funding, effective management at every level, anticorruption and strong dedication of the government are crucial factors. Moreover, proper infrastructure, adequate and quality skilled workers production by having regular training, supervision, adequate equipment and job satisfaction could prepare the health workers to be more confident and efficient in delivering skilled services to the mothers. Furthermore, proper advocacy from the policy level to ground level with proper monitoring and evaluation and by sharing information and knowledge will escalate the behaviour change along with communication to make people improve their perceptions, to be aware about their rights and the process to get access to SBAs. Finally, universal health coverage for maternal care which the Bangladesh government aims to reach the SDG by 2030, will be helped by the above initiatives, and access to an SBA for every mother could be ensured for all classes, ethnicities, with equity and quality for safe childbirth and maternal health care.
Competing Interest
We declare no competing interests
21079
References
- WHO (2010) Improving maternal, newborn and child health in the South-East Asia Region: Focus on Bangladesh.
- WHO (2016) Trends in maternal mortality: 1990 to 2015 [online]. World Health Organization.
- Kwast BE (1996) Reduction of maternal and perinatal mortality in rural and peri-urban settings: What works? European Obstetrics & Gynecology and Reproductive Biology J 69: 47–53.
- Bashar SAM, Dahlblom K, Stenlund H (2012) Determinants of the use of skilled birth attendants at delivery by pregnant women in Bangladesh.
- Graham WJ, Bell JS, Bullough CH (2000) Can skilled attendance at delivery reduces maternal mortality in developing countries? SHSOP pp. 97-130.
- WHO/UNFPA/UNICEF/World Bank (1999) Reducing maternal mortality. A joint statement by WHO/UNFPA/UNICEF/World Bank. Geneva: World Health Organization.
- NIPORT (2016) Bangladesh Demographic and Health Survey 2014. Dhaka, Bangladesh, and Rockville, Maryland, USA: NIPORT, Mitra and Associates, and ICF International.
- Koenig MA, Saha T, Al-Sabir A, El Arifeen S, Hill K, et al. (2007) Maternal health and care-seeking behavior in Bangladesh: Findings from a national survey. International Family Planning Perspectives 33: 75–82.
- Afsana K (2005) The tremendous cost of seeking hospital obstetric care in Bangladesh. Reproductive health matters 12: 171–80.
- Bergeson-Lockwood J, Madsen EL, Bernstein J (2010a) Maternal health supplies in Bangladesh.
- Turkmani S, Gohar F (2014) Community based skilled birth attendants. Journal of Asian Midwives 1: 17–29.
- Majumder MAA (2013) World health statistics 2011: How does Bangladesh compare with other south-east Asian countries? South East Asia Journal of Public Health 1: 1.
- Kamal N, Curtis S, Hasan MS, Jamil K (2016) Trends in equity in use of maternal health services in urban and rural Bangladesh. Int J for Equity in Health Vol. 15.
- Tasnim S, Rahman A, Shahabuddin AKM (2009) Access to skilled care at home during pregnancy and childbirth: Dhaka Bangladesh. International Quarterly of Community Health Education 30: 81–87.
- Blum LS, Sharmin T, Ronsmans C (2006) Attending home vs. Clinic-based deliveries: Perspectives of skilled birth attendants in Matlab, Bangladesh. Reproductive Health Matters 14: 51–60.
- Walton LM, Schbley B (2013) Cultural barriers to maternal health care in rural Bangladesh. Online Journal of Health Ethics Vol. 9.
- Joint Learning Initiative (2004) Human resources for health: Overcoming the crisis.
- Ahmed SM, Hossain MA, Rajachowdhury AM, Bhuiya AU (2011) The health workforce crisis in Bangladesh: Shortage, inappropriate skill-mix and inequitable distribution. Human Resources for Health Vol. 9.
- WHO (2006) The World Health Report 2006 - Working together for health. Geneva: World Health Organization.
- Ahmed S, Mahmood I (2012) Health systems in Bangladesh. Health Systems and Policy Research Vol. 1.
- Islam N, Islam MT, Yoshimura Y (2014) Practices and determinants of delivery by skilled birth attendants in Bangladesh. Reproductive Health Vol. 11.
- Ahmed SM, Alam BB, Anwar I, Begum T, Huque R, et al. (2015) Bangladesh health system review. Vol 5
- Bhuiyan AB, Mukherjee S, Acharya S, Haider SJ, Begum F (2005) Evaluation of a skilled birth attendant pilot training program in Bangladesh. Int J of Gynecology & Obstetrics 90: 56–60.
- Islam F, Rahman A, Halim A, Eriksson C, Rahman F, et al. (2015) Perceptions of health care providers and patients on quality of care in maternal and neonatal health in fourteen Bangladesh government healthcare facilities: A mixed-method study. BMC Health Services Research Vol. 15.
- Sibley L, Sipe T, Brown C, Diallo M, McNatt K, et al. (2007) Traditional birth attendant training for improving health behaviours and pregnancy outcomes. Cochrane Database Syst Rev
- Lewis M (2006) Governance and corruption in public health care systems. SSRN Electronic Journal.
- Brinkerhoff D, Bossert T (2008) Health Governance: Concepts, Experience, and Programming Options. USAID.

