A.Dukat1*, P.Sabaka1, J.Gajdosík2, F.Simko3, M.Vrbnjak1 and O.Tlcimuka1
2nd. Department of Internal Medicine Comenius University, Bratislava, Slovakia
Prim Med Care Ctr, Nove Zamky, Slovakia
Department of Pathophysiology Comenius University, Bratislava, Slovakia
Corresponding Author:
Andrej Dukat, MD, PhD
2nd. Department of Internal Medicine Comenius University
13 Mickiewiczova, SK 81369 Bratislava, Slovakia
Tel: 533337301
E-mail: andrej.dukat@sm.unb.sk
Title: Acid uric and other cardiovascular risk factors control in the primary care settings in the community.
Background: Hyperuricaemia represents nowaday the newer risk factor for cardiovascular di-seases. Epidemiologic data shows, that its prevalence differs in various populations signifi-cantly from 4% up to 40% with race and geographical variables. Prevalence data and its con-trol in our patient´s population are missing yet. From The Framingham data relative risk was estimated of 25% for cardiovascular diseases, coronary heart disease and all-course mortality. The purpose of the survey was to bring the registry data as the source for the further evalua-tion and secondary prevention measures.
Methods: 330 primary care physicians in the country were asked to participate for the survey Mirror Slovakia. Hyperuricaemia and other main cardiovascular risk factors were evaluated from the sample of 20 000 patients from the primary care physician´s registries. Final data were obtained from 19,644 patients having all three controls: baseline, at 6th and 12th months. Risk factor control and medical therapy was evaluated from the medical records and pa-tient´s diaries in order to see the primary care in the community settings.
Findings: High prevalence of the main risk factors was seen to contributing to very high glo-bal cardiovascular risk of our patients in the community. This corresponds with the current one of the highest cardiovascular mortality in Europe. Significant higher acid uric concentra-tions among treated patients was seen in men, but not in women. The most often used diure-tic hydrochlorothiazide was in clinical practice of hypertension. Hyperuricemia was more prevalent among patients treated with hydrochlorothiazide both in men and in women. Selec-tion of types of antihypertensives with uricosuric effects may contribute to the improvement of the metabolic changes among treated high risk patients.
Conclusions: Obtained data for the national registry are the source for the improvement in risk factor control and secondary prevention in daily clinical practice in the country.
Keywords
Hyperuricaemia, Cardiovascular risk, Hypertension
Introduction
About possible assotiations of uric acid to the cardiovascular risk it is known from the lite-rature already from the end of 19th century [1]. Epidemiologists as well as clinicians are repeatedly showing to assotiations of hyperuricaemia to cardiovascular, renal, and metabolic risks [2,3]. Hyperuricaemia among patients with present cardiovascular disease represents the predictor of poor prognosis, and in hospitalized populations also the predictor of an increased hospital mortality, especially among heart failure patients [4,5]. Slovakia nowadays present one of the highest cardiovascular morbidity and mortality in Europe [6]. There is the need for the improvement of the global cardiovascular risk in the country. First step has to be the registry of high risk patients, knowledges of treatment measures and patient´s compliance to therapy [7,8].
Methods
In 2014 there have been the epidemiologic study called Mirror Slovakia performed in the community with the followed sample of 20 000 primary care patients followed and treated for the period of 12 months. Patients were followed-up after 6 and 12 months, and wrote their standard questionnaire. From the followed sample results were obtained from 19 644 patients (46,06% men and 53,94% women). After already severe cardiovascular event were 13,79% patients (after myocardial infarction 7,63% and after stroke 6,16%). Comorbidities presented were hypertension in 7400, dyslipidemia in 3080, 9102 had both comorbidities present (hy-pertension and dyslipoproteinaemia). 3709 were up to 60 years of age, 3755 over 60 years. Current smokers were in 4554, 213 had type I, and 3793 diabetes mellitus type II.
The aim of the study was to see the prevalence of coronary risk factors, including acid uric and their control in the contitions of daily clinical practice in the country. This survey was supported with the educational grant Mirror Slovakia sponsored by Krka Slovakia. This epidemiological project was approved by the local ethical committee as well as the main ethical committee in the capital of the country. It was approved by the Association of Primary Care Physicians and all of the participants signed the informed consent participating in this study.
Statistical methods: Descriptive data are given as the mean ± standard errors. Normal dis-tribution of variables was controlled by Kolmogorov-Smirnov‘s test. Mean acid uric levels between the samples were compared using Mann-Whitney‘s test, as its values had not normal distribution. Cathegorical variables (number of patients in the groups) were compared using χ-2 test. To assess correlations of single variables (age, BMI, BP, TAG, LDL-C, HDL-C, creati-nine) to acid uric concentration, Spearmann corelation test was used.
Results
19 644 treated patients from the survey Mirror Slovakia were followed for the period of 12 months to evaluate hyperuricemia and other main risk factors. Concentrations of acid uric were compared to the hypertension control after the guidelines. There have been differences between the sexes: significant correlation were seen in men, but not in women (Figures 1,2).
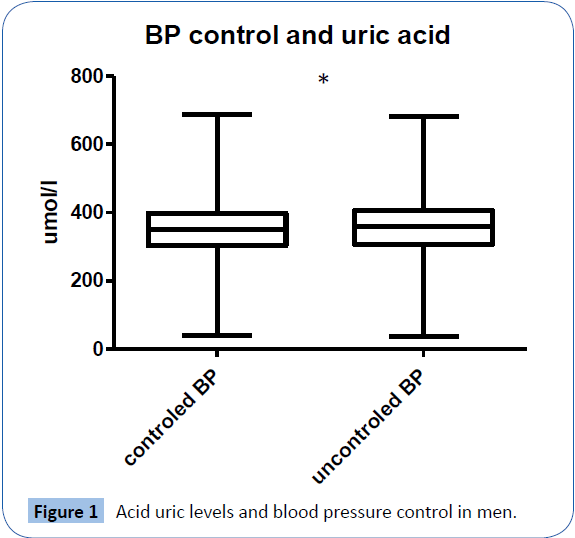
Figure 1: Acid uric levels and blood pressure control in men.
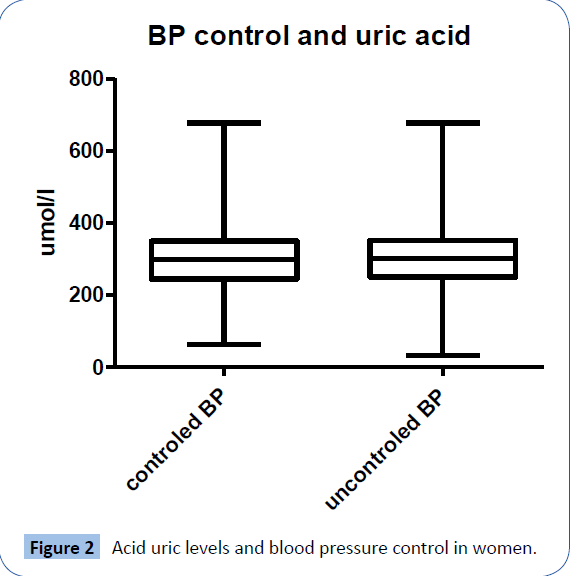
Figure 2: Acid uric levels and blood pressure control in women.
Among treated males with uncontrolled hypertension according the guidelines significant higher acid uric levels were present (p<0.0001). This correlation was not seen among treated women (p=0.188).
The most common therapy for hypertension in our daily clinical practice are thiazide diuretics (hydrochlorothiazide). This therapy may influence the acid uric levels among the patients (p<0.05). Therapy with hydrochlorothiazide significantly increased the acid uric levels, both in men and in women (Figures 3,4).
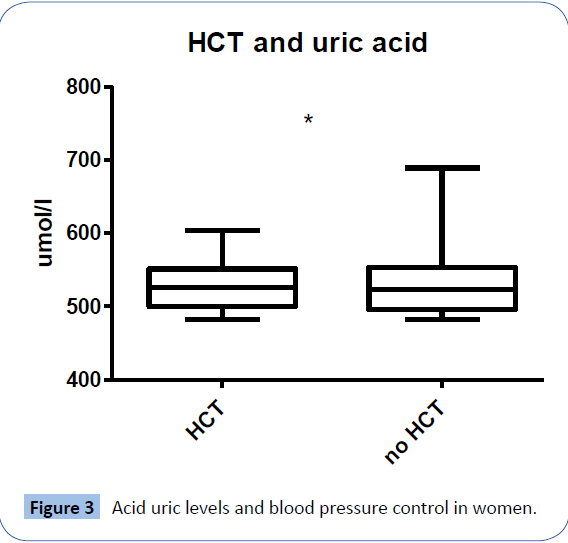
Figure 3: Acid uric levels and blood pressure control in women.
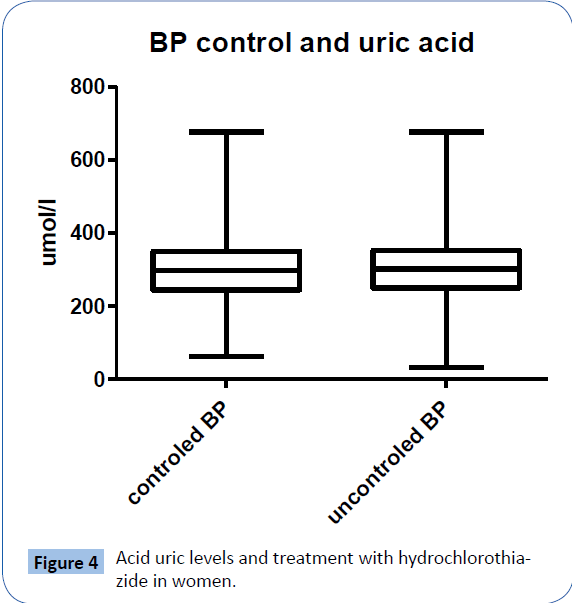
Figure 4: Acid uric levels and treatment with hydrochlorothiazide in women.
| parameter |
P value |
Spearman r |
95% confidence interval |
| BMI (kg/m2) |
< 0,0001 |
0,1705 |
0,1457 - 0,1950 |
| Waist (cm) |
< 0,0001 |
0,2028 |
0,1675 - 0,2376 |
| TAG (mmol/l) |
< 0,0001 |
0,1899 |
0,1653 - 0,2142 |
| Kreat (umol/l) |
< 0,0001 |
0,2561 |
0,2323 - 0,2797 |
| BPs (mmHg) |
< 0,01 |
0,04094 |
0,01565 - 0,06617 |
| BPd (mmHg) |
< 0,001 |
0,04718 |
0,02190 - 0,07240 |
| HR (min-1) |
< 0,0001 |
0,04863 |
0,02335 - 0,07386 |
| Age (years) |
0,0589 |
0,02368 |
-0,001624 - -0,04896 |
Table 1: Correlations of acid uric levels to selected parameters in men.
| parameter |
P value |
Spearman r |
95% confidence interval |
| BMI (kg/m2) |
< 0,0001 |
0,1705 |
0,1457 - 0,1950 |
| Waist (cm) |
< 0,0001 |
0,2028 |
0,1675 - 0,2376 |
| TAG (mmol/l) |
< 0,0001 |
0,1899 |
0,1653 - 0,2142 |
| BPs (mmHg) |
< 0,01 |
0,04094 |
0,01565 - 0,06617 |
| BPd (mmHg) |
< 0,001 |
0,04718 |
0,02190 - 0,07240 |
| HR (min-1) |
< 0,0001 |
0,04863 |
0,02335 - 0,07386 |
| Age (years) |
0,059 |
0,02368 |
-0,001624 - 0,04896 |
| LDL-C (mmol/l) |
< 0,0001 |
0,09511 |
0,06991 - 0,1202 |
| HDL-C (mmol/l) |
< 0,0001 |
-0,04839 |
-0,07371 - -0,02300 |
BMI = body mass index
TAG = triglycerides
BPs = systolic blood pressure
BPd = diastolic blood pressure
HR = heart rate
LDL-C = low density cholesterol
HDL-C = high density cholesterol |
Table 2: Correlations of acid uric levels to selected parameters in women.
Patients were followed after 6 and 12 months. Mean acid uric levels in baseline were 353,8 ± 75,98 μmol/l, after 6 months 343,9 ± 73,88 and after 12 months 338,7 ± 71,53 μmol/l. The trend towards the decrease of acid uric levels during the follow-up period could be seen.. Percenta-ge of patients with hyperuricemia decreased from 1101 (17,3%) through 826 (13%) up to 695 (11%) (baseline, 6 month, 12 month) respectively.
Discussion
Patophysiological causes of hyperuricemia are complex and associations with cardiovascular diseases were described [9,10]. Especially associations such as arterial hypertension, systemic inflammation, decreased vascular response, proaggregation, endothelial dysfunction and oxidative stress are present [11]. Acid uric concentrations revealed the broad reference interval up to the high age with some chronobiological fluctuations. From The INTERHEART study we know, that the uric acid concentration correlate with the body weight, is present in 80% patients with metabolic syn-drome, type 2 diabetes mellitus and in 70% of patients occured together with diabetes mellitus and hypertension.
During the last decade nearly 9 studies were published, showing the association between acid uric concentrations and cardiovascular diseases, but still hyperuricemia is not recognized as the important risk factor [12,13]. For the clinical practice is is useful to recognize the relation-ship of hyperuricemia and endothelial dysfunction and that normalization of its levels together with control of other risk factors may contribute to improvement of endothelial function [14,15]. From this aspect rationale is to follow-up the acid uric levels and for the cardiological phar-macotherapy to choose drugs having except their main therapeutic effects also possible acid uric lowering effect (i.e.ACE-inhibitors, AT-1 blockers, calcium channel blockers, sta-tins, fibrates) [16,17].
Follow-up of antihypertensive and goiter treatment among 24 768 patients with hypertension 20-79 yrs old compared to randomized controls from Britain´s registry (BMJ 2012:344:d8190) showed the benefit of calcium channel blockers with losartan and disadvantage of diuretic tre-atment from the side of acid uric levels.Uricozuric effect was achieved with losartan RR:0,8l (0,70- 0,94) and calcium channel blockers RR:0,87 (0,82-0,93). Treatment with betablockers, ACE-inhibitors ans AT-1 blockers was neutral: betablockers RR:1,48 (1,40-1,57), ACE-inhi-bitors RR:1,24 (1,17- 1,32) ans AT-1 blockers (without losartan) RR:1,29(1,16-1,43). Therapy with diuretics lead to the increase of acid uric levels RR:2,36 (2,21-2,52).
In The ACTION study among 7665 patients therapy with amlodipine lowered acid uric levels of 21%, and nifedipine GITS of 13%. Therapy with losartan significantly lowered the acid uric levels of 20-25%. Therapy with other AT-1 blockers: candesartan, valsartan, telmisartan a eprosartan did not changed the acid uric levels. To the contrary increased acid uric levels was present with the therapy of older betablockers: propranolol, timolol, alprenolol, atenolol, but also metoprolol.
Hyperuricemia has its influence also in the process of vascular inflammation leading to pre-glomerular arteriolopathy. As a result of hyperuricemia there is also the tubulointerstitial in-flammation and fibrosis. zápal a fibróza. Hyperactivity of the renin-angiotensinaldosterone system, leads to the decrease of glomerular filtration rate and the decrease of the fractional natrium excretion. This process is accompanied by an increase of renin release and the dec-rease of NO-synthase [18]. For the detrimental effects of hyperuricemia however several me-chanisms are involved. End results are the effects: proinflammatory, proaggregative, prooxydative and proproliferative, all having vasculotoxic effects with further enhancing the endo-thelial dysfunction [19]. Endothelial dysfunction seen at the beginning of the pathophysio-logical mechanisms leads to atherotrombosis and further cardiovascular events [20]. There is also the connection to dyslipidaemia through the systemic inflammation. Hyper-uricaemia is associated with the increased ratio triglyceride to HDL-cholesterol and presence of liver steatosis (independently of presence of metabolic syndrome and obesity) with the increase of hsCRP [21].
Conclusions
There is the increase of data showing the associations of hyperuricemia to cardiovascular di-seases. Thus hyperuricemia may represent an useful marker for the complex evaluation of the global cardiovascular risk, as well as the possible therapeutic target for the secondary preven-tion. Several prospective studies are ongoing to estimate the value of this relatively newer biomarker.
Funding
this survey was supported by the educational grant of KRKA Slovakia. Funding source was used for the technical support: printing the protocols, patients diaries, informed consent and for statistical evaluation of results.
7039
References
- Alderman MH (2007) Podagra, uric acid, and cardiovascular disease. Circulation 116: 880-883.
- Culleton BF, Larson MG, Kannel WB, Levy D (1999) Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study. Ann Intern Med 131: 7-13.
- Saag KG, Choi H (2006) Epidemiology, risk factors, and lifestyle modifications for gout. Arthritis Res Ther 8 Suppl 1: S2.
- Ghei M, Mihailescu M, Levinson D (2002) Pathogenesis of hyperuricemia: recent advances. Curr Rheumatol Rep 4: 270-274.
- Leyva F, Anker SD, Godsland IF, Teixeira M, Hellewell PG, et al. (1998) Uric acid in chronic heart failure: a marker of chronic inflammation. Eur Heart J 19: 1814-1822.
- Nichols M, Townsend N, Scarborough P, Rayner M (2013) Trends in age-specific coronary heart disease mortality in the European Union over three decades: 1980-2009. Eur Heart J 34: 3017-3027.
- Choi HK, Curhan G (2007) Independent impact of gout on mortality and risk for coronary heart disease. Circulation 116: 894-900.
- Feig DI, Kang DH, Johnson RJ (2008) Uric acid and cardiovascular risk. N Engl J Med 359: 1811-1821.
- Zhu Y, Pandya BJ, Choi HK (2011) Prevalence of gout and hyperuricemia in the US general population: the National Health and Nutrition Examination Survey 2007-2008. Arthritis Rheum 63: 3136-3141.
- Whelton A (2012) Hyperuricemia and hypertension: a confluence of concepts. Hypertension 60: 1112-1113.
- Loeffler LF, Navas-Acien A, Brady TM, Miller ER 3rd, Fadrowski JJ (2012) Uric acid level and elevated blood pressure in US adolescents: National Health and Nutrition Examination Survey, 1999-2006. Hypertension 59: 811-817.
- Tangri N, Weiner DE (2010) Uric acid, CKD, and cardiovascular disease: confounders, culprits, and circles. Am J Kidney Dis 56: 247-250.
- Ndrepepa G, Braun S, Haase HU, Schulz S, Ranftl S, et al. (2012) Prognostic value of uric acid in patients with acute coronary syndromes. Am J Cardiol 109: 1260-1265.
- Kivity S, Kopel E, Maor E, Abu-Bachar F, Segev S, et al. (2013) Association of serum uric acid and cardiovascular disease in healthy adults. Am J Cardiol 111: 1146-1151.
- Linke AHP, Oberbach A, Jehmlich N (2013) Hyperuricemia induces endothelial dys-function by increasing reactive oxygen species. Eur Heart J 34: S1.
- Filippatos GS, Ahmed MI, Gladden JD, Mujib M, Aban IB, et al. (2011) Hyperuricaemia, chronic kidney disease, and outcomes in heart failure: potential mechanistic insights from epidemiological data. Eur Heart J 32: 712-720.
- Rich MW (2000) Uric acid: is it a risk factor for cardiovascular disease? Am J Cardiol 85: 1018-1021.
- Mos L, Saladini F, Fania C (2014) Epidemiology and Prevention of CV Disease: Physiology, Pharmacology and Lifestyle. Circulation 130: A12539.
- Aguilar FG, Selvaraj S, Martinez EE (2012) Serum Uric Acid is an Independent Risk Fac-tor for Subclinical Cardiac Dysfunction: A Speckle-Tracking Analysis of the HyperGEN Study. Circulation 126: A14448.
- Wong CKA, Chen Y, Zhen Z (2013) Gender-specific differences in the association of hyperuricaemia with subclinical atherosclerosis. Eur Heart J 34:S-1.
- Keenan T, Blaha MJ, Nasir K, Silverman MG, Tota-Maharaj R, et al. (2012) Relation of uric acid to serum levels of high-sensitivity C-reactive protein, triglycerides, and high-density lipoprotein cholesterol and to hepatic steatosis. Am J Cardiol 110: 1787-1792.


