Engin O*, Kilinc G and Tuncer K
Department of General Surgery, Izmir Tepecik Education and Research Hospital, Turkey
- *Corresponding Author:
- Engin O
Department of General Surgery
Izmir Tepecik Education and Research Hospital
Turkey
Tel: +902324525252
E-mail: omerengin@hotmail.com
Received date: December 14, 2018; Accepted date: April 10, 2019; Published date: April 17, 2019
Citation: Engin O, Kilinc G, Tuncer K (2019) Acute Intestinal Obstruction in an Adult Patient Due to Ladd’s Band: A Case Report. J Univer Surg Vol.7 No.1:1. DOI: 10.36648/2254-6758.7.1.106
Introduction: In adult patients some adhesions between intestinal segments and malignities are common in the ethiology of mechanic intestinal obstruction whereas congenital anomalies are seen rare. In this case report we present a 60-year-old patient presents with mechanical bowel obstruction symptoms and diagnosed as Ladd's bands.
Case presentation: A 60-year-old male applies emergency servise with vomiting and nausea. According to the laboratory and radiological tests the paient was diagnosed as mechanical bowel obstruction and underwent exploratory laparatomy. In exploration Ladd's band was seen and cut for releasing the herniated intestinal segments.
Discussion: Congenital anomalies of intestinal rotation are often seen in infants and children therefore this pathology can be missed in adult patients. We must be aware of these pathologies on the way of diagnosis of the patients with mechanical bowel obstruction.
Keywords
Congenital anomalies; Ladd's bands; Herniated intestinal segments; Bowel obstruction; Hernias
Introduction
In adult patients, mechanical bowel obstructions (MBO) caused by adhesions, malignancies and hernias can be seen. Congenital anomalies which cause intestinal obstructions are one of the most important parts of childhood MBO reasons therefore these pathologies can be missed in diagnosis of intestinal obstruction in adults. Intestinal malrotation is a rare pathology which occurs with the rate of 0.2%-0.5% and most cases diagnosed in neonatal period whereas only 0.2% of them found in adulthood [1,2]. Ladd's band is one of the congenital bands that can cause internal herniation and intestinal volvulus which can disrupt bowel circulation and make intestinal necrosis. Patients usually apply in childhood with obstructive symptoms such as vomiting and nausea. Here we present an adult patient who was hospitalized with the diagnosis of mechanical bowel obstruction and operated for Ladd's band. The disease we mentioned in our case report is not a very rare situation. It is among rare diseases. There is not a lot of case series about this pathology therefore for making contribution to the case series in literature we are presenting our case to your evaluation.
Case Presentation
A 60-year-old male applied to emergency service with symptoms vomiting and nausea. The patient had no comorbid diseases and prior history of abdominal surgery. In physical examination abdominal distension and tenderness in all abdominal quadrants were found. First standed abdominal X-ray graphy and laboratory tests including complete blood count, renal and liver function tests and electrolytes were analyzed. In laboratory tests creatinine levels were finding minimally increased due to vomiting and other parameters were normal. In abdominal X-ray air-fluid levels were seen as a sign of intestinal obstruction therefore abdominal computered tomography (CT) was taken to show the pathology which caused ileus (Figure 1). On abdominal CT scan, free fluid in abdominal cavity and thickened intestinal walls with air-fluid levels in was seen (Figure 2).
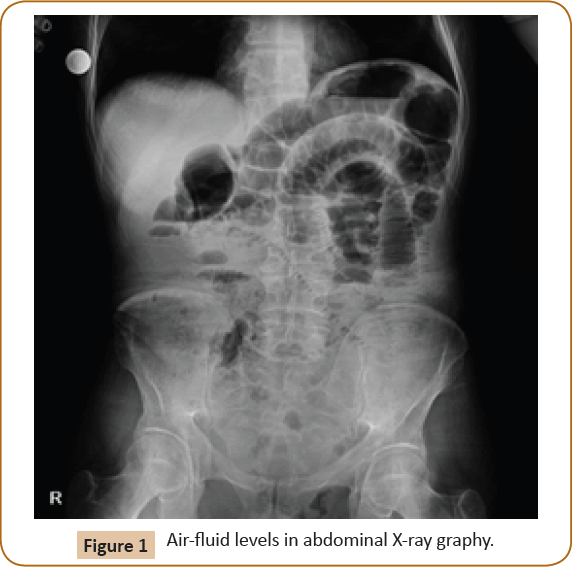
Figure 1: Air-fluid levels in abdominal X-ray graphy.
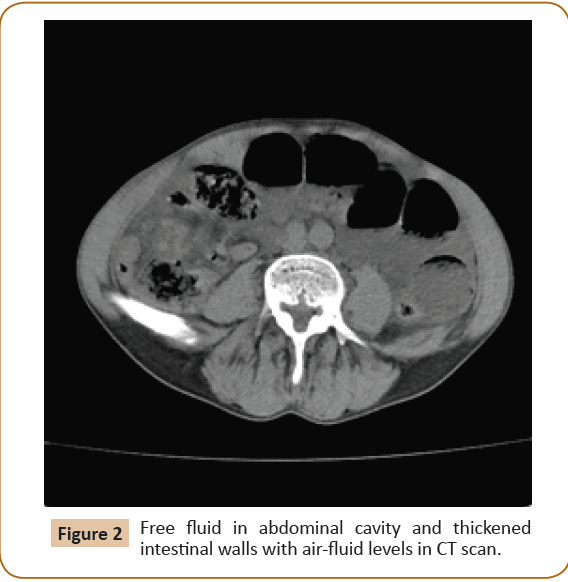
Figure 2: Free fluid in abdominal cavity and thickened intestinal walls with air-fluid levels in CT scan.
The patient was hospitalized, nazogastric tube was placed, iv hidration therapy and enema were given. According to occured acute abdomen symptoms and up to 90 degree angle air fluid levels in control abdominal X-ray the patient underwent exploratory laparatomy. In exploratory laparatomy Ladd's band between cecum and right lateral abdominal wall was seen and all intestinal segments starting after 150 cm of the treitz ligament underwent internal herniation and ischemia below this band (Figure 3).
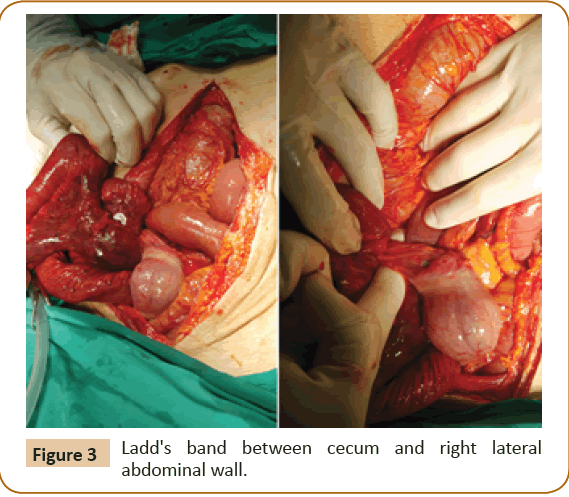
Figure 3: Ladd's band between cecum and right lateral abdominal wall.
Ladd's band was cauterized and cut for releasing the intestinal segments. After performing hot compresses to the intestines ischemia was regressed and the patient left to the second look. In second look all intestinal circulation and motility found to be normal except the 150th cm from the treitz ligament where the herniation beginned in the first operation. This segment was found to be necrosed therefore ileostomy was performed due to the edema and calibration differences between the intestines. On postoperative day 2 the patient was started oral intake. On postoperative day 5 the patient discharged with antimotility agents and the diet list prepared by the nutritionist. At present the patient is following up in outpatient clinics and preparing for the stoma closure [3-5].
Discussion and Conclusion
Congenital anomalies of intestinal rotation are often seen in infants and children; however, they are uncommon in adults. Approximately 85% of malrotations present in neonatal period therefore it is difficult to diagnose this pathology in adult patients. Patients with malrotation can be asymptomatic throughout their lives whereas some of them can be symptomatic in adulthood. Patients usually apply with obstructive symptoms such as vomiting, nausea, general abdominal pain and distension. On the way of diagnose; abdominal X-ray graphies, CT scans, barium studies and angiography can be performed. In treatment according to the quality of bowel circulation and motility Ladd's procedure or bowel resection with anastomosis or ostomy can be done.
24330
References
- Kotze PC, Martins JF, Rocha JG (2011) Procedimento de Ladd para má rotação intestinal no adulto: relato de caso. Arq Bras Cir Dig 24: 89-91.
- Dilley AV, Pereira J, Shi EC (2000) The radiologist says malrotation: Does the surgeon operate? Pediatr Surg Int 16: 45-49.
- Wang C, Welch CE (1963) Anomalies of intestinal rotation in adolescents and adults. Surgery 54: 839-855.
- McIntosh R, Donovan EJ (1939) Disturbances of rotation of the intestinal tract. Am J Dis Child 57: 116-166.
- Gamblin TC, Stephens RE, Johnson RK, Rothwell M (2003) Adult malrotation: A case report and review of the literature. Curr Surg 60: 517-520.

