Keywords
Winkler’s disease, Chondrodermatitis Nodularis helicis, carcinoma.
List of Abbreviations
Chondrodermatitis nodularis chronica helicis (CNCH)
Background
Winkler’s disease usually presents as 3 to 10 mm nodules in the helix or anti helix. We are reporting an unusual presentation of Winkler’s disease as a large nodular mass arising from the tragus, nearly occluding the external auditory canal (size about 1.5 x 2.0 cms).
Case presentation
A 19 year old female patient presented to us with a painful swelling in the right ear of 1 week duration. Initially it was pin head sized and gradually increased to present size after being traumatized by patient herself.
Clinically right pinna showed a dome shaped firm, reddish grey mass about 1.5x2.0 cms. (Figure 1). Surface was scaly in appearance, tender and does not bleed on palpation. Tympanic membrane not visualised as the mass had occluded the External Auditory meatus completely. There was no regional lymphadenopathy.
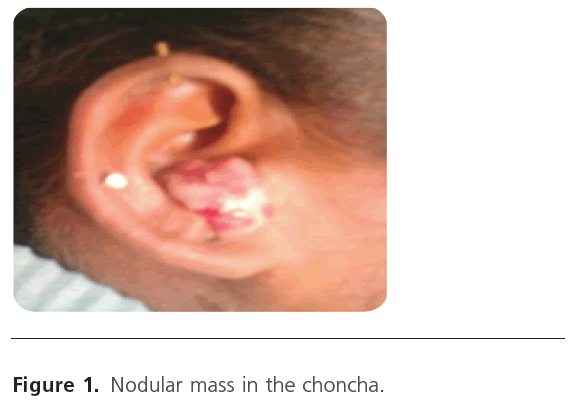
Figure 1: Nodular mass in the choncha.
The lesion was excised in–toto under local anaesthesia; underlying tragal cartilage was exposed but intact. There was minimal bleeding during the procedure and raw area was cauterized chemically. Specimen was sent for Histopathologic examination. (Figure 2).

Figure 2: Excised mass.
Diagnosis
Histopathologic examination (Figure 3 & 4), shows bits of granulation tissue with prominent vascular proliferation and dense mononuclear cell infiltrate admixed with eosinophils. Overlying stratified squamous epithelium shows hperplastic changes with acanthosis, papillomatosis and hyperkeratosis with foci of ulcerations and reported as features of exuberant granulation tissue and diagnosed as Chondrodermatitis nodularis chronica helicis.
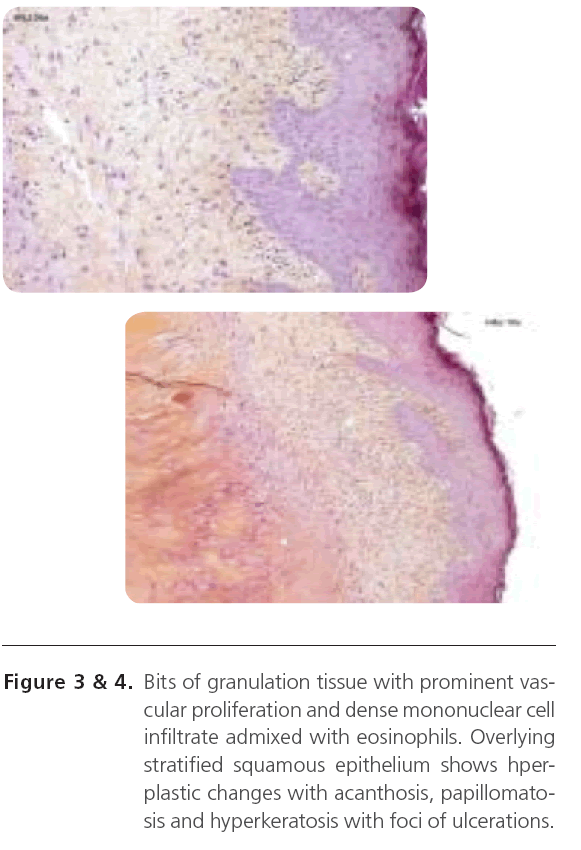
Figure 3&4: Bits of granulation tissue with prominent vascular proliferation and dense mononuclear cell infiltrate admixed with eosinophils. Overlying stratified squamous epithelium shows hperplastic changes with acanthosis, papillomatosis and hyperkeratosis with foci of ulcerations.
Treatment
The lesion was excised in–toto under local anaesthesia; underlying tragal cartilage was exposed but intact. There was minimal bleeding during the procedure and raw area was cauterized chemically.
Discussion
Chondrodermatitis nodularis chronica helicis (CNCH) describes an uncommon, painful, inflammatory nodule of the external ear.1-7 Most cases involve middle-aged or elderly white men who have these nodules on the outer rim of the helix.1-4,7 Women and nonwhites have been noted occa-sionally to have lesions in areas other than the helix, such as the antihelix or antitragus. The lesions are believed by several researchers[1-3,8] to relate to trauma or sun damage. The nodules are more commonly reported on the right ear, which is believed to be the preferred resting side during sleep.[8] The lack of a thick, cushioning, subcutaneous layer in the auricle may predispose the underlying cartilage to pressure-induced ischemia and damage.[7] Despite numerous theories, the exact cause and pathogenesis of CNCH remain uncertain.[2,4-5] There are no reliable figures for its incidence or prevalence but it is probably common condition. It is probably caused mainly by pressure, combined with the anatomy of the pinna and its blood supply:
The initial damage may be triggered by inflammation, oedema, and necrosis from trauma, cold, actinic damage or pressure. The pinna has relatively little subcutaneous tissue for insulation and padding. Only small dermal blood vessels supply the epidermis, dermis, perichondrium and cartilage. These features may prevent adequate healing and lead to secondary perichondritis. Possibly, perichondrial arteriolar changes may also be involved.
Clinical appearance.
The nodules of CNCH usually appear dome shaped, firm, reddish gray, with an erythematous rim, and vary from 3 to 10 mm. The surface of the lesion often is covered with a scale or crust over an underlying central depression.[1-2] Ulceration can be present, and the lesion usually is tender to even the slightest pressure. The lesions usually persist, with spontaneous remission rare.[1] The lesions do not develop malignancy.
Lesions often appear to arise spontaneously, and patients may not relate a definite history of trauma. The nodules often cause notable distress, and patients often seek medical advice when the pain interferes with sleep.[8-10] The characteristic location, appearance, and pain usually allow for proper diagnosis.[1,8] Histological examination may support the diagnosis, but is performed mainly to exclude cancer.[8]
Histologically, the lesions often demonstrate dermal inflammation and fibrosis associated with either a central hyperkeratotic plug or ulceration and crust.[1,3] Ulcer margins often demonstrate hyperplasia, but Hurwitz[3] noted that one third of 84 lesions had no ulceration. Cartilage beneath the granulomatous and fibrotic dermis often is disrupted, hemorrhagic, and even necrotic, although occasionally it can appear undamaged. [3] Chondrodermatitis nodularis chronica helicis lesions could begin as a perichondritis, extending outward to involve the skin.[6] It is possible that inflamed hair follicles in the skin may be central to the pathologic process.[3]
Management options.
The unusual nature of CNCH and the high recurrence rate for this benign condition has produced a wide variety of surgical and nonsurgical treatment options.2, 6 Nonsurgical options include cryotherapy, topical corticosteroids, topical antibiotic ointments, intralesional collagen injection, and intralesional corticosteroid injection.[1-5,7,10] Surgical options are generally considered the treatment of choice, and include wedge resection of the skin and cartilage with suture closure; curettage and electrocautery; carbon dioxide laser ablation therapy; and excision of the skin lesion followed by scalpel resection, curettage, or electrosurgical treatment of the underlying cartilage.[1-9,11-13]
Dermatologist and ENT surgeons may need to perform a biopsy of lesions of CNCH to exclude the presence of other conditions such as cancer. Shave biopsy followed by treatment to the wound base is often advocated as an initial diagnostic and therapeutic intervention.[2,8] Soft, necrotic, underlying cartilage can be removed by vigorous curettage.[2] Reports from before 1960 suggested recurrences from this technique at more than 20%.[6,8] More aggressive treatment to the underlying cartilage also has been performed. Kromann et al[8] reported a recurrence rate of 31% among 142 patients treated with curettage followed by electrodesiccation (electrosurgical ablation) of the underlying cartilage. We have successfully treated this patient with a modification of the shave technique on the skin, followed by cauterization of the base with Silver nitrate.
Surgical excision remains the hallmark of therapy for CNCH.[1] Unfortunately, recurrences are common if all sites of inflammation are not removed.[2,6,9] Even when wide excision of the underlying cartilage is performed, recurrences have developed in up to 10% of patients at the edges of the excised cartilage.[6,12] The cartilage damage beneath a nodule usually involves only 1 cartilage surface, and some physicians advocate a partial excision procedure involving the cartilage, rather than a through-and-through pie-shaped or wedge excision of the auricle. Lawrence[13] has advocated that only the damaged cartilage should be removed, with skin flap closure performed over the excised cartilage. Lawrence has reported excellent cosmetic results and cures in 34 (74%) of 46 patients.
Learning points/take home
• Chondrodermatitis nodularis chronica helicis is an uncommon dermatologic condition that can present to the dermatologist or ENT surgeon as a painful nodule on the ear.
• Proper identification of the lesion, and exclusion of a skin cancer of the auricle, will allow for proper treatment.
• Dermatologist may initially try topical or injection therapy, but surgical therapy usually is required.
• Several fairly simple excisional procedures can be performed to remove the painful nodule, but additional treatment of the underlying diseased cartilage will provide the highest cure rates.
Acknowledgments
MVJ Medical College and research Hospital, Bangalore.
2502
References
- Wade TR (1979) Chondrodermatitis nodularis chronica helicis: a review with emphasis on steroid therapy. Cutis 24:406-409.
- Habif TP (1996) Clinical Dermatology: A Colour Guide to Diagnosis and Therapy. 3rd ed. St Louis, Mosby: 643.
- Hurwitz RM (1987) Painful papule of the ear: a follicular disorder. J Dermatol Surg Oncol; 13:270-274.
- Greenbaum SS (1991) The treatment of chondrodermatitis nodularis chronica helicis with injectable collagen. Int J Dermatol; 30:291-294.
- Coldiron BM (1991) The surgical management of chondrodermatitis nodularis chronica helicis. J Dermatol Surg Oncol; 17:902-904.
- Munnoch DA, Herbert KJ, Morris AM. (1996) Chondrodermatitis nodularis chronica helicis et antihelicis. Br J Plast Surg.; 49:473-476.
- Long D, Maloney ME (1996) Surgical pearl: surgical planing in the treatment of chondrodermatitis nodularis chronica helicis of the antihelix. J Am Acad Dermatol; 18:761-762.
- Kromann N, Hoyer H, Reymann F (1983) Chondrodermatitis nodularis chronica helicis treated with curettage and electrocauterization: follow-up of a 15-year material. Acta Derm (Stockh); 63:85-87.
- Sinclair P (1996) Excision technique for chondrodermatitis nodularis helicis. Australas J Dermatol; 37:61.
- Beck MH. (1985) Treatment of chondrodermatitis nodularis helicis and conventional wisdom? Br J Dermatol; 113:504-505.
- Karam F, Bauman T (1988) Carbon dioxide laser treatment for chondrodermatitis nodularis chronica helicis. Ear Nose Throat J; 67:757-763.
- Kitchens GG (1989) Auricular wedge resection and reconstruction. Ear Nose Throat J; 68:673-683.
- Lawrence CM (1991) The treatment of Chondrodermatitis nodularis with cartilage removal alone. Arch Dermatol; 127:530-535.

