Munish Kumar1, Durgesh Kumar2 and Kamlesh Tewary3
1Department of Neurology, Sri Krishna Medical College, Muzaffarpur, Bihar, India
2Residentship, Sri Krishna Medical College, Muzaffarpur, Bihar, India
3Department of Medicine, Sri Krishna Medical College, Muzaffarpur, Bihar, India
- *Corresponding Author:
- Munish Kumar
Department of Neurology, Sri Krishna Medical College
Muzaffarpur, Bihar, India
Tel: 9102556521
Email: munishpmch@gmail.com
Received Date: October 11, 2016; Accepted Date: November 02, 2016; Published Date: November 04, 2016
Citation: Kumar M, Kumar D, Tewary K. Assessment of Essential Tremors on Clinical and Functional Performance Tests. 2016, 7:6 doi: 10.21767/2171-6625.1000157
Keywords: Essential tremor; 9-Hole Peg test (9-HPT); Box and block test
Introduction
Tremor is the most common movement disorder, defined as “a rhythmic, involuntary oscillatory movement of a body part.” It is repetitive and stereotyped that distinguishes it from other involuntary movements like chorea, athetosis, ballism, tics, and myoclonus [1]. Functionally, tremor impacts the performance of fine motor skills such as feeding, drinking, writing, body care, and fine object manipulation [2]. The severity of tremor can be measured with a variety of clinical and electrophysiological techniques, including clinical rating scales, quality-of-life questionnaires, spirography (Archimedes’ spirals), functional performance tests, for example, the nine- Hole Peg test, box and block test, and, by accelerometery and surface electromyography. Various rating scales were designed specifically for the assessment of tremor amplitude or the impact of tremor on activities of daily living (ADL) and quality of life [3]. Effect of tremor on daily living activities (ADL) can be evaluated using specific questionnaires such as the ADL-T24, which has a good inter-session reproducibility [4]. The nine- Hole Peg test and box and block test are simple, low-cost, and efficient test of gross manual dexterity. The nine-Hole Peg test had high Inter-rater reliability (r=0.96) as well as good testretest reliability (r=0.69) [5]. The box and block test had high inter-rater reliability (r=0.99) and Test-retest reliability (r=0.94) [6]. The purpose of the study is to quantify the disability due to tremor with the functional performance test scores.
Design/Methods
A total of 60 patients, more than 12 years of age, having essential tremor that presented to Sri Krishna Medical College and Hospital, Muzaffarpur, Bihar, India between June 2015 to May 2016 were prospectively analyzed on clinical and functional performance tests. This study was carried after ethical clearance and permission of the institute. A written informed consent was taken from subjects or parents, after adequate explanation. All patients were subjected to general physical and detailed neurological examination. Assessment of disability done using Activities of Daily Living scales / ADLT24.4 Tremor severity was assessed on the basis of difficulties encountered while doing activities of daily living [7]. Tremor severity was divided into mild, moderate, severe, and incapacitating. Mild (1) - able to do the activity without difficulty, moderate (2) - Able to do the activity with a little effort, severe (3) - Able to do the activity with a lot of effort, and incapacitating (4) - Cannot do the activity by himself.
The functional performance tests used are 9-Hole Peg test 5- A square board with nine holes (each hole 1.3 cm deep and are spaced 3.2 cm apart) and nine wooden pegs (0.64 cm in diameter and 3.2 cm long) was used. Patients were allowed to pick one peg (from a container beside the holes) at a time and then quickly put into the hole in any order until holes were filled and in continuation instructed to remove the pegs one at a time and return them to the container. Using a stop watch time calculated in seconds when patient touched the first peg till the last peg returned to the container. Each hand was separately tested.
Box and block Test 6 - A rectangular box that is divided into two square compartments of equal dimension by means of a partition with 100 blocks (2.5 cm × 2.5 cm × 2.5 cm) was placed lengthwise in front of the patient at a comfortable height. The blocks were in the compartment of the test box on the side of the patient’s corresponding hand i.e., right or left. The patients were instructed to grasp one block at a time with the tested hand, transport the block over the partition, and release it into the opposite compartment. This was done for one minute and at the end number of blocks counted. If a patient transported two or more blocks at a time, this number was subtracted from the total. The score was the number of blocks carried from one compartment to the other in one minute. Each hand was separately scored.
Data Analysis
Demographic data and the functional performance tests score were recorded and analyzed using SPSS v20.0 software. Values were expressed as mean ± Standard deviation (SD) or mean ± Standard error (SE). The Spearman rank correlation coefficient (r) was used to analyze the relationship between tremor severity and the functional performance tests score. The correlation coefficient (r) considered as poor if r<0.3 and moderate if 0.3 < r < 0.5 and strong if r>0.5.
Results
Sixty patients with essential tremor had the mean ± SD age of 48.32 ± 19.04 years (range 16 to 92 years) with male: female ratio as 9:1 i.e., males more common than females and out of which 8 (13.34%) had positive family history. Their mean disease duration was 3.82 years. Phenomenologically tremor was mainly action/postural in 90.2% but was also present at rest in 9.09% and as intention type in 9%.
Fifty-six percent patients had mild tremor severity, 32% moderate, 11% severe and 1% incapacitating type. The mean ADL-T24 Score was 3.21 in mild, 8.54 in moderate, 14.63 in severe and 23.12 in incapacitating type of tremor (Figure 1).
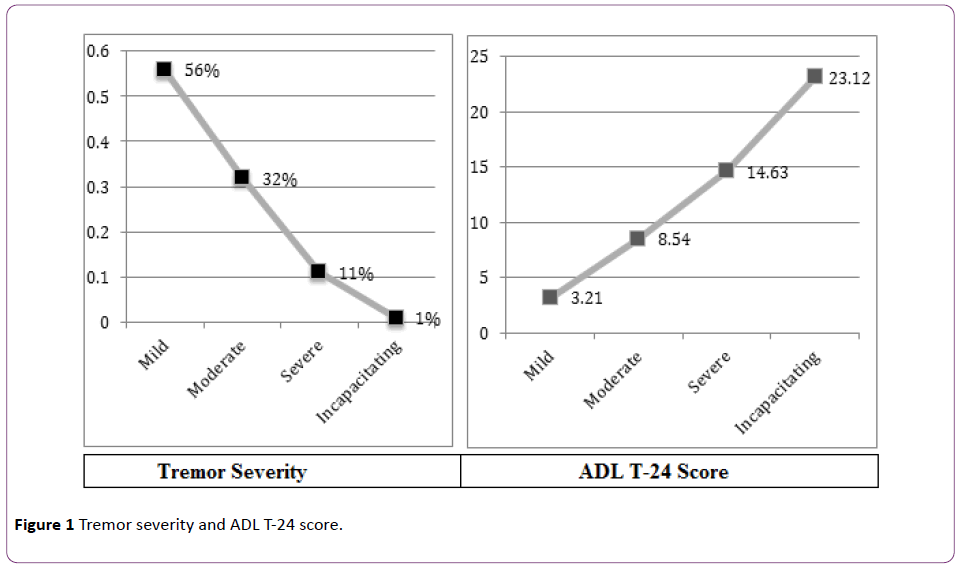
Figure 1: Tremor severity and ADL T-24 score.
The mean disease duration had positive correlation with the ADL-T24 score. This means that as the disease progresses the difficulty in doing daily living activities increases.
The mean (± SD) number of seconds taken during 9-Hole Peg Test was 17.26 (± 4.32) seconds. The mean (± SD) number of blocks transferred within one minute with box and block test was 46.21 (± 8.64). There was a positive correlation between ADL-T24 score and 9-Hole Peg score (R2=+0.56) but a negative correlation between ADL-T24 and box and block score (R2=-0.68) (Figures 2 and 3).
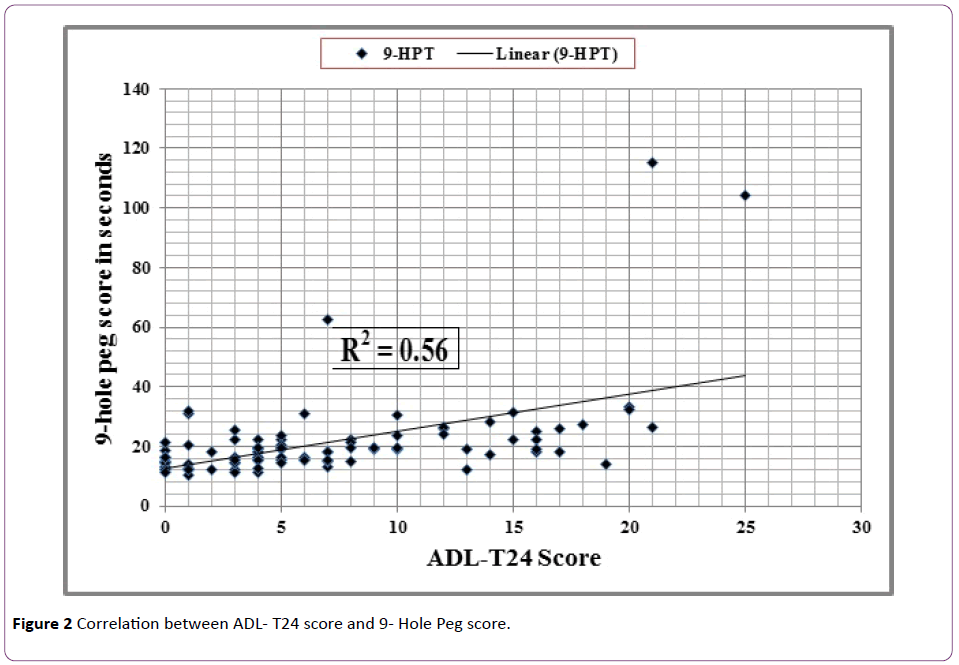
Figure 2: Correlation between ADL- T24 score and 9- Hole Peg score.
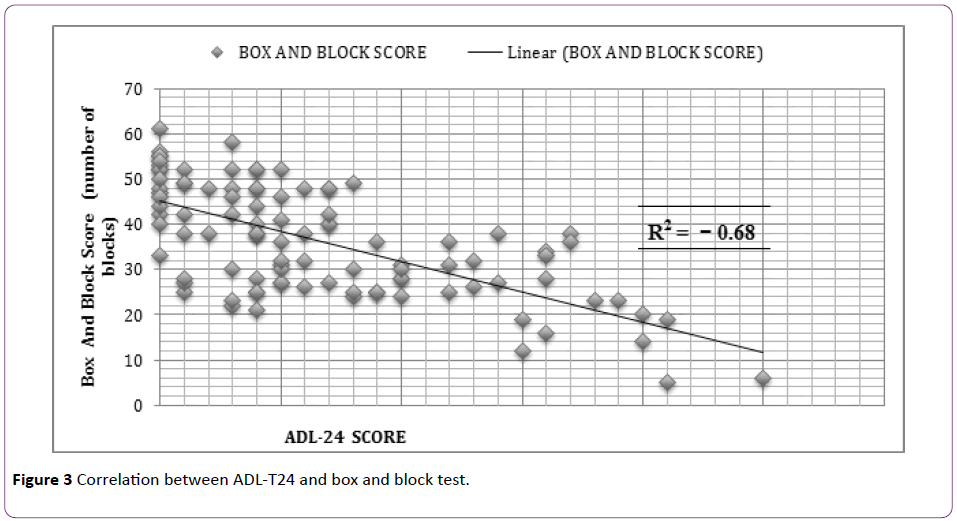
Figure 3: Correlation between ADL-T24 and box and block test.
Reciprocal pattern was seen between 9-Hole Peg score and box and block test score. The correlation coefficient between them is -0.57.
Discussion
A particular tremor rating scale ADL – T24 was used for clinical scoring of the Essential tremor. The functional performance tests like 9-Hole Peg Test and box and block test were used because they had good test-retest and inter-rater reliability. The mild to moderate tremor was more common than severe and incapacitating type. The ADL-T24 score was proportionate to tremor severity. There was a positive correlation between disease duration and mean ADL-T24 score. This shows that as the disease progress, the daily living activities becomes more difficult.
There was a moderate positive correlation between ADLT24 score and 9-Hole Peg score (R2=+ 0.56) whereas a strong negative correlation between ADL-T24 and box and block score (R2=-0.68). This signifies that those having higher ADLT24 score will take longer time to complete 9-Hole Peg test and lesser number of blocks be transferred in one minute". To best of our knowledge only one study of this type by Girimaldi found a positive correlation between ADL-T24 score and 9-Hole Peg score (R2=0.89) and a negative correlation between ADL-T24 and box and block score (R2=-0.66) [8]. Reciprocal pattern was seen between 9-Hole Peg score and box and block score with a moderate negative correlation (R2=-0.57), similar to study by Girimaldi G (R2=-0.75) [8]. Thus, the tremor severity correlates well with the functional performance tests. The comparative study of ADL–T24, 9-Hole Peg score and box and block score with Essential tremor had not been reported previously from India.
Conclusion
The severity of tremor was correlated with the help of quality-of-life questionnaires as well as with functional performance tests, for example, the nine-Hole Peg test, box and block test. The functional performance tests are potential to measure the tremor severity.
17527
References
- Bhidayasiri R (2005) Differential diagnosis of common tremor syndromes. Postgrad Med J 81: 756-762.
- Héroux ME,Parisi SL,Larocerie-Salgado J, NormanKE (2006) Upper-extremitydisability in essentialtremor. Arch PhysMedRehabil87:661-670.
- Elble R, Bain P, Forjaz MJ, Haubenberger D, Testa C, et al. (2013) Task force report: Scales for screening and evaluating tremor: Critique and recommendations. MovDisord 28: 1793-1800.
- Grimaldi G, Manto M (2010) Neurological tremor: Sensors, signal processing and emerging applications. Sensors 10:1399-1422.
- Mathiowetz V, Weber K, Kashman N, Volland G (1985) Nine Hole Peg test: Normative data for adults. OccupTherJ Res 5:24-38.
- Mathiowetz V, Volland G, Kashman N, Weber K (1985) Adult norms for the box and block test of manual dexterity. Am J OccupTher 39:386-391.
- Bain PG, Findley FJ, Atchison P, Behari M, Vidailhet M, et al. (1993) Assessing tremor severity. JNNP 56:868-873.
- Grimaldi G, Manto M (2013) Mechanisms and emerging therapies in tremor disorders. Contemporary Clinical Neuroscience 26:325-340.

