Petchiappan V1, Selvam S2, Dhanush M1 and Prabu N3**
1PSG Institute of Medical Sciences and Research, Coimbatore, Tamil Nadu, India
2St Johns Research Institute, Bengaluru, Karnataka
3Sakthi Rheumatology Centre Private Ltd, Coimbatore, Tamil Nadu, India
Corresponding Author:
Naga Prabu
Sakthi Rheumatology Centre Private Ltd
Coimbatore, Tamil Nadu, India
Tel: +919787055266
E-mail: nagaprabu1@gmail.com
Received date: June 18, 2018; Accepted date: July 04, 2018; Published date: July 11, 2018
Citation: Petchiappan V, Selvam S, Dhanush M, Prabu N (2018) Assessment of Handgrip Strength in Patients with Rheumatoid Arthritis and Fibromyalgia-Do They Differ? -An Observational Study. Arch Med Vol No:10 Iss No:4:3 doi: 10.21767/1989-5216.1000279
Copyright: © 2018 Petchiappan V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Hand grip strength; Grip strength in rheumatoid arthritis; Hand grip strength in fibromyalgia; Dynamometer; Rheumatoid arthritis; Fibromyalgia
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory systemic disorder of autoimmune etiology which causes progressive joint inflammation, destruction and limitation of joint function if left untreated. Hand and wrist joint involvement is noticed in 80 to 90% of RA patients [1] leading to hand deformities and limitation of the hand function. The most commonly affected hand joints are the metacarpophalangeal (MCP), proximal interphalangeal (ICP) and wrist joints. Reduced flexion or extension of PCP and MCP joints affect the fine movements of the hand and grasp function [2] causing functional disability which in turn affects the activities of daily living (ADL).
Impairment of hand function in RA is due to multiple factors. Apart from hand pain, deformities and loss of range of joint movements, the decreased muscle strength or fatigue also plays an important role in the limitation of joint function. Most of the patients with RA have reduced handgrip strength and impaired hand function [3-7] which has implications on the overall morbidity and mortality.
The effect of handgrip strength on total locomotion [8] was studied by Jonsson et al. and found it to be highly significant. Also one of the predictors of mortality in RA was reduced handgrip [9] as noted by Pincus et al. All these indicate that it is all the more important to assess the hand function in RA patients and initiate appropriate early treatment strategies to preserve the hand function.
Another rheumatological disease which causes chronic widespread pain, fatigue, limitation of physical activities, functional and emotional impairment is Fibromyalgia syndrome [10-14]. Chronic pain seen in fibromyalgia is non-inflammatory.
Alteration in the central processing of pain input and defect in endogenous inhibition of pain is responsible for the chronic widespread pain and increased pain sensitivity [15]. Difficulty in performing the daily routine tasks such as walking, reaching for high shelves, lifting objects and washing own hair is due to decrease in the muscle strength and flexibility. Numerous studies have shown reduced handgrip in patients with FM [ 16-20].
In fact RA and FM are two commonly encountered rheumatological diseases which can cause limitation of hand function. Both can co-exist in the same patient and can have masking clinical features. In view of increased pain sensitivity seen in FM patients, they might exhibit tenderness on palpation which can be mistaken for hand involvement in RA. This necessitates the objective measurement of hand function by using a valid tool to assess the hand function.
Assessment of handgrip by dynamometer is a well-established measure to assess the hand function in both the diseases [ 16,21]. With this background, we intended to assess the handgrip strength in RA and FM patients and to compare it with the healthy subjects to find out the degree of impairment of hand strength in both the study groups.
Aim
The aim of the study is to assess the handgrip strength in RA and FM patients and to compare it with the age and sex matched controls.
Patients and Methods
The study included a total of 30 study subjects, out of which 16 had Rheumatoid arthritis diagnosed as per 2010 ACR classification criteria; 14 had Fibromyalgia diagnosed according to ACR revised diagnostic criteria 2016.
A group of 30 age and sex matched controls were chosen in the study. Subjects more than 17 years were included in the study. Patients with hand deformities or anomalies, blindness, neurological or muscular diseases which affect the performance of the test were excluded from the study.
Methodology
This is a cross sectional observational study conducted in patients attending Rheumatology OP during June 2013-March 2014 in a tertiary care center in Coimbatore, South India. The study design was approved by the Ethics committee and informed consent obtained from all the participants. The handgrip strength of the dominant and non–dominant hand was assessed in both the study and control groups by the same examiner to avoid the inter-observer error.
The hand grip power assessment was done by using a country made handheld plastic dynamometer with the readings from 0 to 110 kilograms. This hand held dynamometer has the advantage of easy availability and reduced cost. The assessment was done with the subjects seated in a chair, shoulders adducted and neutrally rotated, elbows flexed at 90 degrees, forearm in neutral position; wrist between 0 to 30 degrees dorsiflexion and 0 to 15 degrees ulnar deviation. After an initial demonstration of the test, the subjects were asked to squeeze the instrument gradually and continuously for a period of at least two seconds; two recordings were taken in each hand and the mean score was calculated.
Statistical Analysis
Descriptive statistics were reported using mean and SD, median with 25th, 75th percentiles. Handgrip strength of right and left sides were compared between FM and RA group using independent t test. Handgrip strength between FM, RA and control group was compared using ANOVA. Bonferroni correction test was done for multiple comparisons. Paired t test was used to compare the right and left side handgrip strength in each group separately. p value less than 5% was considered as statistically significant.
Results
Among 30 patients, 16 had RA with a mean age of 53.19 ± 6.12 years; 14 had FM with a mean age of 45.36 ± 13.48 years.
The mean age of the control group was 48.03 ± 11.07 years. There were 13 females each in the RA and FM groups; while there were 3 males in RA and 1 male in FM group. There were 4 male and 26 females in the control group.
The results of mean, median with 25th and 75th percentiles of hand grip in RA, FM and control groups were listed in Table 1. The mean hand grip in dominant hand was 87.8 ± 22.7 kilograms in fibromyalgia while in RA it was 60.3 ± 21.0 kilograms. Nondominant hand grip was 72.5 ± 25.7 kilograms in fibromyalgia while in RA it was 52.2 ± 29.3 kilograms. In healthy controls the grip strength was 89.4 ± 11.7 in dominant hand and 81.2 ± 14.1 kilograms in non-dominant hand.
| Variables |
FM |
RA |
P-value |
| Dominant Hand |
Mean |
87.8 ± 22.7 |
60.3 ± 21.0 |
0.002* |
| Median with 25th and 75th percentiles |
90 (70, 110) |
70 (40, 77) |
| Non-dominant Hand |
Mean |
72.5 ± 25.7 |
52.2 ± 29.2 |
0.055* |
| Median with 25th and 75th percentiles |
70 (53.7, 92.5) |
45 (31, 70) |
Table 1: Comparison of hand grip in rheumatoid arthritis (RA) and fibromyalgia (FM) patients.
On comparison of the hand grip strength between RA and FM patients (Table 1), we found that RA patients had a significantly lower hand grip in both dominant and non-dominant hands than FM patients (p=0.002 and p=0.055 respectively).
When compared with healthy age and gender matched controls (Figure 1), results showed that RA group had significantly lower dominant hand grip than FM and healthy controls (p<0.001). While comparing the non-dominant handgrip strength, it was observed that both FM and RA groups had significantly lower strength as compared to health control groups (Table 2).
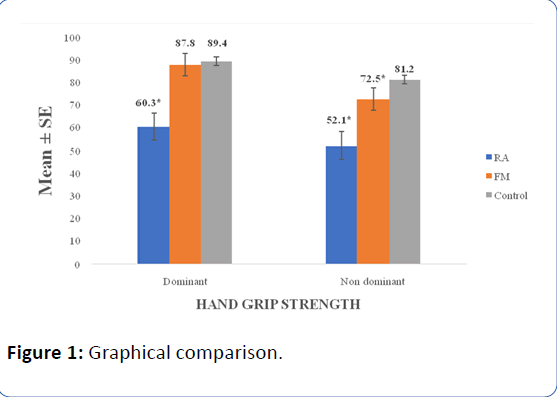
Figure 1: Graphical comparison.
| Variables |
FM |
RA |
Control |
P-value |
| Dominant Hand |
Mean |
87.8 ± 22.6 |
60.3 ± 21.0* |
89.4 ± 11.7 |
<0.001 |
| Median with 25th and 75th percentiles |
90 (70, 110) |
70 (40, 78) |
85 (80, 100) |
| Non-dominant Hand |
Mean |
72.50 ± 25.70* |
52.1 ± 29.2* |
81.2 ± 14.1 |
<0.001 |
| Median with 25th and 75th percentiles |
70 (54, 93) |
45 (31, 70) |
80 (70, 90) |
|
| *Significantly lower than control group. |
Table 2: Comparison of hand grip in rheumatoid arthritis (RA), fibromyalgia (FM) and healthy controls.
Within group comparison of dominant and non-dominant hand grip, results showed that in FM group, hand grip strength was significantly higher in dominant hand (p=0.003) but there was no significant difference in RA group (Table 3).
| Variables |
Dominant Hand |
Non-dominant Hand |
P-value |
| FM |
87.8 ± 22.6 |
72.5 ± 25.7 |
0.003* |
| RA |
60. 3 ± 21.0 |
52.1 ± 29.2 |
0.403 |
Table 3: Comparison of dominant and non-dominant handgrip in rheumatoid arthritis (RA) and fibromyalgia (FM) patients.
Discussion
While there are various studies on RA and FM separately which had compared the hand grip strength with that of healthy controls, the literature is sparse regarding head-on comparison of handgrip in FM and RA patients. Our study is one of its kinds which assessed the handgrip force in RA and FM patients and compared it with the healthy controls. The present study showed that both the dominant and non-dominant hand grip was less in RA group when compared with the FM and healthy controls. Our observation of reduced hand grip in RA patients when compared with the healthy controls was similar to that observed in other studies [17,22,23].
Our results concur with the other studies which had reported lower hand grip in FM patients when compared with the healthy women [17,18]. Nordenskiold et al. [17] reported 40% reduction in the handgrip in FM patients than healthy adults. Sahin et al. [ 18] compared the handgrip of 41 fibromyalgia patients with 40 years of age and BMI matched healthy women and noted lower grip force in FM patients. Similar observation of reduced grip force in FM patients than healthy controls was noted in other studies as well [19,20]. Also patients with severe FM had lower grip force than those with moderate FM [16,24] which we have not analyzed in our study.
In the present study we noted that the dominant hand grip is significantly higher than the non-dominant hand in FM group while we did not observe any significant difference in RA group. This might possibly be due to symmetrical hand involvement limiting the hand grip function equally in Rheumatoid arthritis. The data from the literature is conflicting regarding the influence of dominance on hand grip in RA patients. Iop et al. [25] did not observe a significant difference in hand grip between the right and left hand in the Rheumatoid arthritis group which was similar to our observation. Fraser et al. [26] observed that dominant hand in RA patients was on average 20% weaker than the non-dominant hand while another study [27] reported greater hand grip in the dominant hands of RA patients.
To the best of our knowledge, we found only one study which had assessed the hand grip strength in RA and FM patients and compared it with the healthy controls. Our observation of reduced grip force in both the study groups was similar to that observed by Nordenskjold [17] who had studied 19 RA, 14 FM and 18 healthy subjects. The hand grip was assessed by Grippit instrument and compared with the normative data from 169 healthy subjects.
We used a simple, easily available, non-expensive hand held dynamometer to assess the hand grip while most of the reported studies worldwide had used Jamar dynamometer, a standard instrument to measure the hand grip. The need for assessment of chronic diseases through simple means is more important in the follow up of patients; having expensive and complicated assessment tools may not be always feasible in routine clinical practice. One such kind of instrument is the simple country made hand held dynamometer which is widely available but lacks the reliability. Also the normative data of hand grip as measured by Jamar dynamometer is available across a wide range of population [28]. There is one Indian study with normative data for hand grip in young adults [29] while the data across various age groups is lacking. Hence we compared our study results with the age and sex matched controls.
We have not taken into account the physique and the work pattern of the study population which might have an influence in the assessment of hand grip strength. Manual workers and labors which require lot of muscular action may have a greater hand grip strength than people who are not used to do such activities. The disease activity assessment was not done in our study patients which can have an influence of the hand function. Ours is a small observational study but worth mentioning which can stimulate further research in this field.
Conclusion
RA patients have poor hand grip than fibromyalgia and both RA and FM have low hand grip when compared to controls.
Acknowledgement
We would like to thank the patients and the normal healthy controls for participating in this study.
Competing and Conflicting Interests
The authors declare no competing and conflicting interest.
22944
References
- Durmus D, Uzuner B, Durmaz Y, Bilgici A, Kuru O (2013) Michigan hand outcomes questionnaire in rheumatoid arthritis patients: Relationship with disease activity, quality of life, and hand grip strength. J Back Musculoskelet Rehabil 26: 467-473.
- Melvin JL (1982) Rheumatoid disease, occupational therapy and rehabilitation (2nd ed.), Philadelphia, FA Davis: 32.
- Myers DB, Grennan DM, Palmer DG (1980) Hand grip function in patients with rheumatoid arthritis. Arch Phys Med Rehabil 61: 369-373.
- MacBain KP (1970) Assessment of function in the rheumatoid hand. Can J Occup Ther 37: 95-103.
- An KN, Chao EYS, Askew LJ (1980) Hand strength measurement instruments. Arch Phys Med Rehabil 61: 366-368.
- Spiegel JS, Paulus HE, Ward NB, Spiegel TM, Leake B, et al. (1987) What are we measuring? An examination of walk time and grip strength. J Rheumatol 14: 80-86.
- Jones E, Hanly JG, Mooney R, Rand LL, Spurway PM, et al. (1991) Strength and function in the normal and rheumatoid hand. J Rheumatol 18: 1313-1318.
- Jonsson B, Larsson SE (1990) Hand function and total locomotion status in rheumatoid arthritis-an epidemiologic study. Acta Orthop Scand 61: 339-343.
- Pincus T, Callahan LF, Vaughn WK (1987) Questionnaire, walking time and button test measures of functional capacity as predictive markers for mortality in rheumatoid arthritis. J Rheumatol 14: 240-251.
- Wilson HD, Robinson JP, Turk DC (2009) Toward the identification of symptom patterns in people with fibromyalgia. Arthritis Rheum 61: 527-534.
- Belt NK, Kronholm E, Kauppi MJ (2009) Sleep problems in fibromyalgia and rheumatoid arthritis compared with the general population. Clin Exp Rheumatol 27: 35-41.
- Gormsen L, Rosenberg R, Bach FW, Jensen TS (2010) Depression, anxiety, health-related quality of life and pain in patients with chronic fibromyalgia and neuropathic pain. Eur J Pain 14: 127.
- Salaffi F, Sarzi-puttini P, Girolometti R, Atzeni F, Gasparini S, et al. (2009) Health-related quality of life in fibromyalgia patients: A comparison with rheumatoid arthritis patients and the general population using the SF-36 health survey. Clin Exp Rheumatol 27: S67-S74.
- Mas AJ, Carmona L, Valverde M, Ribas B, EPISER Study group (2008) Prevalence and impact of fibromyalgia on function and quality of life in individuals from the general population: Results from a nationwide study in Spain. Clin Exp Rheumatol 26: 519-526.
- Bradley LA (2009) Pathophysiology of fibromyalgia. Am J Med 122: S22-30.
- Aparicio VA, Ortega FB, Heredia JM, Carbonell-Baeza A, Sjostrom M, et al. (2011) Handgrip strength test as a complementary tool in the assessment of fibromyalgia severity in women. Arch Phys Med Rehabil 92: 83-88.
- Nordenskiold UM, Grimby G (1993) Grip force in patients with rheumatoid arthritis and fibromyalgia and in healthy subjects: A study with the Grippit instrument. Scand J Rheumatol 22: 14-19.
- Sahin G, Ulubas B, Calikoglu M, Erdogan C (2004) Handgrip strength, pulmonary function tests, and pulmonary muscle strength in fibromyalgia syndrome: Is there any relationship? South Med J 97: 25-29.
- Maquet D, Croisier JL, Renard C, Crielaard JM (2002) Muscle performance in patients with fibromyalgia. Joint Bone Spine 69: 293-299.
- Mengshoel AM, Forre O, Komnaes HB (1990) Muscle strength and aerobic capacity in primary fibromyalgia. Clin Exp Rheumatol 8: 475-479.
- Bjork MA, Thyberg ISM, Skogh T, Gerdle BUC (2007) Hand function and activity limitation according to health assessment questionnaire in patients with rheumatoid arthritis and healthy referents: 5-year follow up of predictors of activity limitation (the Swedish TIRA project). J Rheumatol 34: 296-302.
- Brorsson S, Nilsdotter A, Pedersen E, Bremander A, Thorstensson C (2012) Relationship between finger flexion and extension force in healthy women and women with rheumatoid arthritis. J Rehabil Med 44: 605-608.
- Aparicio VA, Carbonell A, Ortega FB, Ruiz-Ruiz J, Heredia JM, et al. (2010) Handgrip strength in men with fibromyalgia. Clin Experiment Rheumatol 28: S78-S81.
- Iop RR, Shiratori AP, Ferreira L, Junior NGB, Domenech SC, et al. (2015) Production capacity of maximal isometric grip strength in women with rheumatoid arthritis: A pilot study. Fisioter Pesq 22: 11-16.
- Fraser A, Vallow J, Preston A, Cooper RG (1999) Predicting ‘normalâ€Âââ€Ã
¾¢ grip strength for rheumatoid arthritis patients. Rheumatol 38: 521-528.
- Nordenskiold U, Grimby G (1997) Assessments of disability in women with rheumatoid arthritis in relation to grip force and pain. Disabil Rehabil 19: 13-19.
- Leong DP, Teo KK, Rangarajan S, Kutty VR, Lanas F, et al. (2016) Reference ranges of handgrip strength from 125,462 healthy adults in 21 countries: A prospective urban rural epidemiologic (PURE) study. J Cachexia Sarcopenia Muscle 7: 535-546.
- Bansal N (2008) Hand grip strength: Normative data for young adults. Indian J Physiother Occup Ther 2: 29-33.


