Research Article - (2016) Volume 8, Issue 5
Breast Cancer in Previously Lactating Women
Amer Hashim Al Ani*, Hussein Shammout, Awad Al Domour and Monther Abu Reden
Department of General Surgery, Sheikh Khalifa Hospital, Ajman, United Arab Emirates
Corresponding Author:
Amer Hashim Al Ani
Department of General Surgery, Sheikh Khalifa Hospital
Ajman, United Arab Emirates
Tel: 00971562623722
E-mail: ameralqadi2002@yahoo.com
Received date: October 13, 2016; Accepted date: October 24, 2016; Published date: October 31, 2016
Citation: Ani AHA, Shammout H, Domour AA, et al. Breast Cancer in Previously Lactating Women. Arch Med. 2016, 8:5 doi: 10.21767/1989-5216.1000168
Copyright: © 2016 Ani AHA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Abstract
Introduction: Many studies suggest that women who breast-fed, had a decreased risk of developing breast cancer (ranging from 10%-64%) compared to women who never breast-fed. Some studies revealed that breastfeeding had no influence on the risk of developing breast cancer. Breastfeeding may be more protective against the development of premenopausal compared to postmenopausal breast cancer. Although there are a few studies that report a decrease in the risk of breast cancer after only three or more months of breastfeeding, the evidence for risk reduction becomes more consistent with the longer women breastfeed. Breast cancer in previously lactating women is rarely dealt with in the medical literature.
Patients and Methods: From January 2009 to May 2012, fifty previously lactating women with breast cancer were studied in Al Bashir Teaching Hospital, Amman, Jordan. Their age ranged from 27-70 yrs, the number of their children were ranging from 3-8 with a history of breastfeeding for 3 months to 3 yrs. The clinical presentation, and ultrasound characteristics, mammogram findings and histopathological criteria were examined.
Result: Breast cancer in lactating women was present in right breast in 23 patients (46%), in the left breast in 27 patients (54%). It was present in the upper outer quadrant in 27 patients (54%), upper inner quadrant in 8 patients (16%), lower outer quadrant in 10 patients (20%), and in the lower inner quadrant in 2 patients (4%). Presenting symptoms were: mass in 25 patients (50%), nipple retraction in 10 patients (20%), ulcers in 5 patients (10%), nipple discharge, or skin tethering in 4 patients each (8%), and pain in 2 patients (4%). By ultrasound 21 lesions (42%) were hypo-echoic, 19 lesions (38%) were of mixed echogenicity, 5 lesions (10%) were isoechoic and 5 lesions (10%) were hyper-echoic. By mammogram 15 lesions (30%) were radio opaque, 12 lesions (24%) were of low opacity, and 2 lesions (4%) were radiolucent. In 4 lesions (8%) micro calcifications were present, in 3 lesions (6%) macro calcifications were present, the mass was speculated in 9 lesions (18%) and skin thickening was present in 5 patients (10%) of the lesions. Forty seven lesions (94%) were a ductal carcinoma, 2 lesions (4%) were a lobular carcinoma, and only 1 case (2%) was a malignant phylloid tumor. Thirty one lesions (62%) were poorly differentiated, 19 lesions (38%) were moderately differentiated, and no well differentiated lesions were detected.
Conclusion: Breast cancer in lactating women is mostly ductal carcinoma that is present as a mass in upper outer quadrant of the left breast, which is hypo-echoic by ultrasound, radio opaque by mammogram and of poor differentiation. These findings need to be reviewed with a larger number of patients.
Keywords
Breast cancer; Previously lactating women; Mammogram
Introduction
Breast cancer is by far the most frequently diagnosed cancer and cause of death among women worldwide. There were an estimated 1.7 million new cases (25% of all cancers in women) and 0.5 million cancer deaths (15% of all cancer deaths) in 2012. Breast cancer is the most common cancer diagnosis in women in 140 countries and the most frequent cause of cancer mortality in 101 countries [1]. The lifetime probability of developing breast cancer is one in six overall (one in eight for invasive disease) [2]. In Jordan in 2010 breast cancer ranked first among cancer in females, accounting for (37.4%), of all female cancers [3]. It is the leading cause of cancer deaths among Jordanian women [3]. Breast cancer accounts for (22.4%) of total new cancer cases in 2010 in Jordan [3]. Even though the incidence of breast cancer in Jordan is lower than the incidence in Western countries, the mortality rate is very high due to late presentation of the disease [3]. Jordanian women are afflicted with breast cancer at a much younger age (median age is 50) than women in Western countries (median age is 65) [3]. Incidence rates of breast cancer are increasing at 4% per year in Jordan [4]. In a society in which 50% of the population is under the age of 18 yrs old, this must be addressed [4]. 89% of mothers breastfed their infants in Jordan [5]. Breast Cancer in Previously Lactating women is the most common breast cancer in Jordanian women, as most of them are affected at a median age of 50 yrs. While pregnancy-associated breast cancer, defined as breast cancer occurring during pregnancy or during the first 12 postpartum months, one can define Breast cancer in previously lactating women as breast cancer occurring after the first 12 postpartum months of last pregnancy [6]. Breast cancer in previously lactating women is rarely dealt with in the medical literature. The aim of this study is to find the differences and similarities between breast cancer in previously lactating women and breast cancer in non-lactating women.
Patients and Methods
From January 2009 to May 2012, fifty cases of previously lactating women with breast cancer were studied in Al Bashir Teaching Hospital, Amman, Jordan. A detailed history was taken and patients were examined thoroughly. Breast ultrasound, mammogram were done for all the patients. Breast preserving procedures, simple or radical mastectomy was the done for all patients. Histopathology reports for surgery specimens were studied. The age of them was ranging from 27 to 70 yrs, with a mean age of 50.7 yrs (Figure 1). All selected women have children. The number of children was ranging from 1-8 (the mean was 5.14) (Figure 2). All of them breast fed (lactated) their children. The minimum lactation duration was ranging from 2-24 months (with a mean of 11.58) (Figure 3). The maximum lactation duration was ranging from 2-36 months (with a mean of 16.85) (Figure 4).
Figure 1: Age range and the mean age of breast cancer patients.
Figure 2: The number of children of patients.
Figure 3: Minimum duration of lactation.
Figure 4: The maximum duration of lactation.
Result
The collected data showed that cancer involved right breast in 23 patient (46%). While left breast was involved in 27 (54%) patients. Upper outer breast quadrant was involved in 27 women (54%). Upper inner quadrant was involved in 8 patients (16%). Lower outer quadrant was involved in 10 patients (20%). Lower inner quadrant was involved in 2% patients (4%). More than one quadrant was involved 3 patients (6%) (Figure 5). Women were presented with one of the following signs and symptoms; breast pain in 2 patients ( 4%), breast mass in 25% (50%) , nipple discharge in 4 women (8%) , nipple retraction in 10 patients (20%) , breast skin ulceration in 5 patients (10%) and skin tethering in 4 patients (8%). The breast masses in these patients by ultrasound examination were hyperechoic in 5 patients (10%). Hypoechoic in 21 patients (42%). Isoechoic in 5 patients (10%). and of mixed echo in 19 patients (38%) (Figure 6). Mammogram findings in these patients include: radioopaque lesions in 15 patients (30%). Low opacity lesions in [6] patients (24%). Radiolucent lesions in 2 patients (4%). There were micro-calcifications in 4 patients (8%). There were macrocalcifications in 3 patients (6%). Speculated masses in 9 patients (18%). Skin thickening was discovered in 5 patients (10%) (Figure 7). Types of malignant tumors discovered during this study were: invasive ductal carcinoma in 47 patients (94%), Invasive lobular carcinoma in patients 2 (4%) and malignant phylloid tumor of the breast in 1 patients (2%). The grading of the tumors in this study was; poorly differentiated tumors in 31 patients (62%). Moderately differentiated tumors in 19 patients (38%). No well, differentiated tumors were observed in this study.
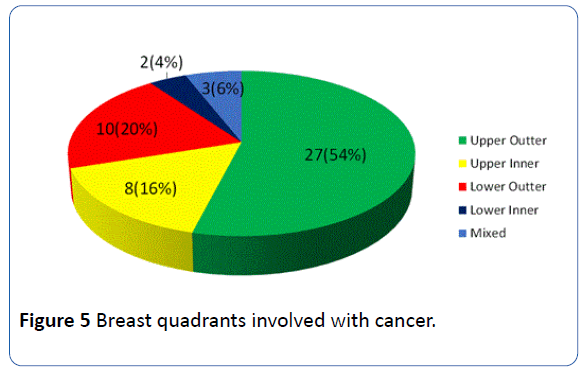
Figure 5: Breast quadrants involved with cancer.
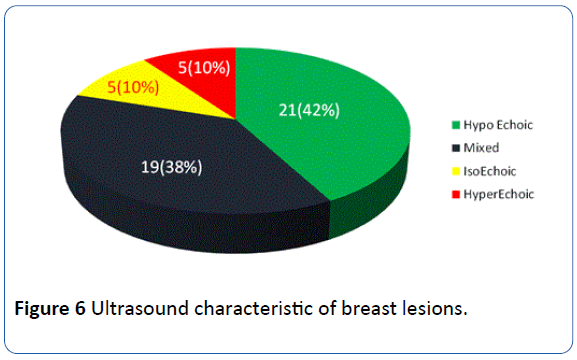
Figure 6: Ultrasound characteristic of breast lesions.
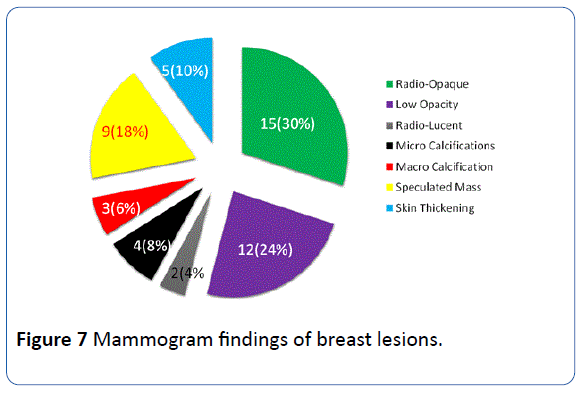
Figure 7: Mammogram findings of breast lesions.
Discussion
Breast feeding lowers breast cancer risk by 4.3% for every year of feeding [7]. The longer the women had breastfed during their lifetime, the less likely they were to get breast cancer [7]. As breast cancer is quite a common disease in developed countries, breastfeeding every child for an extra 6 months would mean about 1,000 fewer cases of breast cancer in a country like Britain each year [7]. Lactation lowers hormones the following breast feeding so it reduces breast cancer risk [8]. Exfoliation of breast tissue during breastfeeding may have a beneficial effect [8]. The breast tissue reduces in size after termination of lactation and goes through a healthy controlled cell death. This will eliminate any cells that developed errors during division, which may potentially lead to breast cancer [8]. Women with deleterious BRCA1 mutations who breast-fed for a cumulative total of more than 1 year had a statistically significantly reduced risk of breast cancer. 8 There was no difference for BRCA2 carriers [8]. Breastfeeding protected against both types of breast tumors regardless of when a woman first gave birth [9]. A modest inverse association between lactation and breast cancer risk has most consistently been observed in premenopausal women [10]. However, these associations have not generally been observed in relation to postmenopausal breast cancer [10]. Most breast cancers in young women and pregnant or lactating women present with a palpable mass [11], whereas most cancers in non-pregnant women older than 40 yrs old are detected by screening mammography before becoming clinically evident [12]. In breast cancer, in previously lactating women the most common presentation is breast mass. The typical US patterns of Breast Cancer are either hypoechoic or isoechoic relative to subcutaneous fat [13]. In our study most of the women ultrasound showed hypoechoic lesions. Malignant lesions (in mammogram) have irregular, speculated margins, greater density than the normal breast tissue [11]. Calcifications which are usually small (<0.5 mm) have a pleomorphic or heterogeneous shape or a finely granular, fine linear, or branching shape [11]. These are similar to the findings in most of our patients.
Conclusion
Breast cancer in lactating women is mostly ductal carcinoma that is present as a mass in upper outer quadrant of the left breast, which is hypo-echoic by ultrasound, radio opaque by mammogram and of poor differentiation. These findings need to be reviewed with a larger number of patients.
17403
References
- Barnes BB, Steindorf K, Hein R, Flesch-Janys D, Chang-Claude J (2011) Population attributable risk of invasive postmenopausal breast cancer and breast cancer subtypes for modifiable and non-modifiable risk factors. Cancer Epidemiol 35: 345-352.
- (2010) The jordan national cancer registry. Cancer incidence in jordan.
- (2008) The jordan national cancer registry. Cancer incidence in jordan.
- (2007) Jordan Department of Statistics: Jordan population and family health survey, Infant feeding practices.
- Hogge JP, De Paredes ES, Magnant CM, Lage J (1999) Imaging and management of breast masses during pregnancy and lactation. Breast J 5: 272-283.
- Jernstrom H, Lubinski J, Lynch HT, Ghadirian P, Neuhausen S, et al. (2004) Breast-feeding and the risk of breast cancer in BRCA and BRCA mutation carriers. J Natl Cancer Inst 96:1094-1098.
- Newcomb PA, Egan KM, Titus-Ernstoff L, Trentham-Dietz A, Greenberg ER, et al. (1999) Lactation in relation to postmenopausal breast cancer. Am J Epidemiol 150: 174-182.
- Conant EF, Dillon RL, Palazzo J, Ehrlich SM, Feig SA (1994) Imaging findings in mucin-containing carcinomas of the breast: correlation with pathologic features. AJR Am J Roentgenol 163: 821-824.
- Shaw de Paredes E, Marsteller LP, Eden BV (1990) Breast cancers in women 35 years of age and younger: mammographic findings. Radiology 177: 117-119.
- Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, et al. (2007) Births: final data for 2005. Natl Vital Stat Rep 56: 1-103.
- Furberg H, Newman B, Moorman P, Millikan R (1999) Lactation and breast cancer risk. Int J Epidemiol 28: 396-402.
- Schousboe JT, Kerlikowske K, Loh A, Cummings SR (2011) Personalizing mammography by breast density and other risk factors for breast cancer: analysis of health benefits and cost-effectiveness. Ann Intern Med 155: 10-20.


