Gomez-Fortty Maria De Los Angeles1*, Gonzelez-Echeverría Kléber Eduardo2 and Esqueda Liquidano Mauricio Armando3
1Neurosurgery Service, San Francisco De Guayaquil Clinical Hospital, Ecuador
2Neurosurgery Service, Hospital Clínica San Francisco De Guayaquil, Ecuador
3Head of the Neurosurgery Service, Naval Hospital of Mexico, Mexico
- *Corresponding Author:
- Gomez-Fortty Maria De Los Angeles
Neurosurgery Service
San Francisco De Guayaquil Clinical Hospital, Ecuador
Tel: + 0988749221
E-mail: Gomezfortty_1998@hotmail.com
Received Date: July 14, 2020; Accepted Date: November 05, 2020; Published Date: November 12, 2020
Citation: Angeles GFMDL, Eduardo GEK, Armando ELM (2020) Calcified Chronic Subdural Hematoma. J Neurol Neurosci Vol.11 No.7:342
DOI: 10.36648/2171-6625.11.7.342
Clinical Image
Simple Skull Tomography
An isodensal image with a wide area of perimeter calcification of left fronto-parieto-occipital extraxial location is observed in a 68-year-old male patient entering with generalized tonic-clonic seizure box, hemiplegia on the right side due to a reduction in brain tissue of up to 200 g, with an increase in extra-brain space by 6 to 11 % allowing parenchyma to adapt to the hematoma and that it is stood [1] (Figure 1).
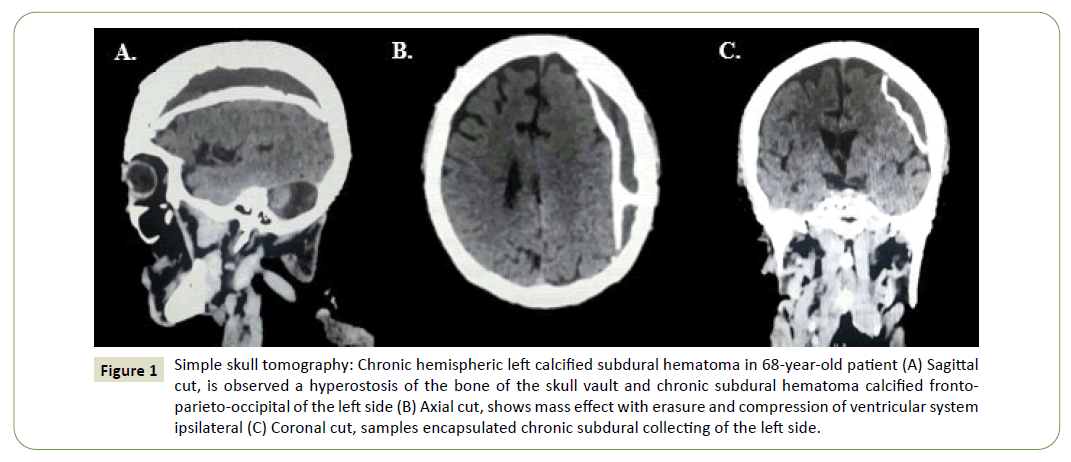
Figure 1: Simple skull tomography: Chronic hemispheric left calcified subdural hematoma in 68-year-old patient (A) Sagittal cut, is observed a hyperostosis of the bone of the skull vault and chronic subdural hematoma calcified frontoparieto-occipital of the left side (B) Axial cut, shows mass effect with erasure and compression of ventricular system ipsilateral (C) Coronal cut, samples encapsulated chronic subdural collecting of the left side.
The clinical presentation of this pathology is often insidious, with symptoms of decreased level of consciousness, problems in gait due to changes in balance, cognitive dysfunction, memory loss, motor deficit (hemiparesias), headache, or aphasia [2].
With the presumptive diagnosis, a left parietal craniotomy was performed, by means of which an encapsulated and calcified lesion was fully exposed on both its parietal and visceral aspects, and which contained a dark red granular substance, totally avascular. Radical resection was performed without surgical complications (Figure 2).
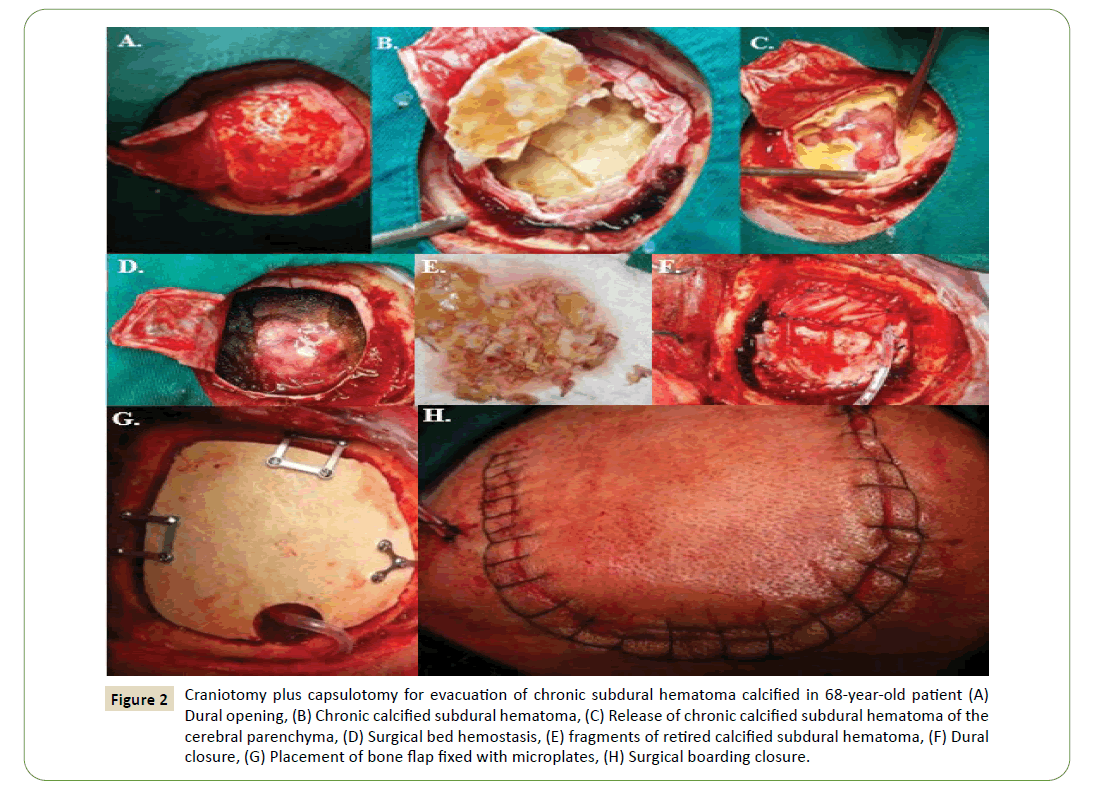
Figure 2: Craniotomy plus capsulotomy for evacuation of chronic subdural hematoma calcified in 68-year-old patient (A) Dural opening, (B) Chronic calcified subdural hematoma, (C) Release of chronic calcified subdural hematoma of the cerebral parenchyma, (D) Surgical bed hemostasis, (E) fragments of retired calcified subdural hematoma, (F) Dural closure, (G) Placement of bone flap fixed with microplates, (H) Surgical boarding closure.
Final result is successful, patient surgical ablation without seizures, regained strength 5/5 in right hemibody, oriented and conscious. It is concluded that chronic subdural hematomas calcification is a rare form of imaging presentation today, known as armoured brain or matryoska brain [3]. Since pseudomembranes are calcified, the chances of brain re-explosion are virtually nonexistent [4]. Finally, the decision of the surgery conforms to the clinical or radiological evidence of mass effect. When there is evidence and the need for a craniotomy approach it could be a better option than trepanation in the management of these entities [4,5].
33699
References
- Balser D, Farooq S, Mehmood T (2015) Traumatic brain injury in the elderly. Arch Med Camaguey 1: 354.
- Ortega Santiesteban O, Gil Alfonso M, Bacallao González L, Hechevarría Álvarez JA, García Díaz M, Alonso Gálvez C. Diagnosis of subdural hematoma: a dynamic clinical and imaging process. Electronic Medical Journal. 2019 Apr; 41 (2): 564-71.
- González AJ, Echabe EA, Dantas CF (2014) Hematoma subdural crónico calcificado:: cerebro blindado. Rev Neurologia 58: 420-421.
- Santarias T, Kolias A, Hutchinson P (2012) Surgical management of chronic subdural hematoma in adults. Oper Neurosurg 2012: 1573-1578.
- García-Pallero MA, Pulido-Rivas P, Pascual-Garvi JM, Sola RG (2014) Chronic subdural hematomas. Internal architecture of the hematoma as a predictor of recurrence. J Neurol 59: 294-300.

