Keywords
Black Stain; Caries experience; ICDAS
Introduction
Dental discoloration is a common cause of aesthetic and clinical problems. Etiology shows differences in terms of appearance, localization, content, severity, degree of tooth attachment [1,2]. Pigments are etiologically separated into three groups and can be listed as: extrinsic, intrinsic, and internalized. Extrinsic pigmentations are localized to the tooth surface by foreign agents. Intrinsic pigmentation occurs when pigmented materials are clustered in the dentin tissues. Internalized discolorations occur when exogenous agents penetrate through defects in the tooth structure and are trapped within the dentin tubules [3,4].
The black stains (BS) are one of the extrinsic discolorations clinically mostly circular, dark black colored, parallel to the gingival margin [5,6]. BS can be observed in both dentitions, primary and permanent, and the prevalence was reported as 1% to 20%, varying according to the country and the population where the study was conducted [7]. However, studies conducted in different countries emphasize that BS formation does not make a significant difference between the sexes [1,8-10].
Content of this black discolored plaque consist a ferric sulfide compound, which occurs as a combination of salivary iron and hydrogen sulfide produced by bacteria which reported to be Actinomyces naeslundii as a common sense [6,7,11-13]. After formation of extrinsic black stained plaque, adhesion to the tooth surface occurs via multiple forces such as Van der Waals, electrostatic, hydrogen bonds and hydrophobic interactions [8,14].
The strong adherence of the black stains makes it difficult for the patient to be removed during daily hygiene routines [15]. Due to esthetic concerns, it is diagnosed by referral to a dentist for professional prophylactic procedures, or by randomly being recognized clinically. Although, curettes, prophylasis paste and discs, ultrasonic devices can clean these stains, they can be reoccurring after a period of time [7,16].
BS’ are distinguished from many other extrinsic colors and have an important place in terms of public health. Many epidemiological studies in this area have shown that patients with BS have a low caries experience [1,8,9,17-20]. The studies have showed the caries-reducing effect of black stains by pointing low DMFT value, which is a parameter that measures the total caries experience, missing teeth and restorations of the individual's entire mouth. Considering that black stains are local occurrences, present study has favored tooth-based evaluation of the caries experience. The International Caries Detection and Assessment System (ICDAS) is a tooth-specific clinical scoring system which determines and codes the activity of lesion [21]. ICDAS is being used for epidemiological analysis, public health research, clinical research, clinical practice and dental education to diagnose the caries status and gives clinicians a treatment protocol [22]. In 2009, aforementioned criteria has improved and were modified, eventually ICDAS II was created. ICDAS II have two-digit coding for detection criteria of coronal caries. The first digit is related to the restoration of teeth that ranges from 0 to 9. The second digit ranges from 0 to 6, used for coding the caries status of teeth from sound enamel to extensive distinct cavity with visible dentin [21]. Plaque removal and Air drying are necessary in the current ICDAS II system [23]. A ball-ended explorer is often used to for visual examination [24]. The aim of our study is to analyze caries status of BS and non-BS teeth by using ICDAS II.
Materials and Methods
This cross-sectional study was carried out in 10 patients with BS from 185 patients attended to Marmara University aged 16-51 years. Detailed anamnesis of patients was recorded after informed consent was taken. All patients had similar oral hygiene habits (brushing teeth with toothpaste at least once a day) and have not been treated with antibiotics within the last 6 weeks with no systemic disease. In addition, patients had no hereditary, morphologically and gender related structural changes (Amelogenesis imperfecta, Dentinogenesis imperfecta, Florosis, Molar-Insizal Hypomineralization etc.) on their teeth. Total of 111 teeth with BS and 144 with non-BS teeth were recorded ICDAS II Scores after visual (naked eye, mirror-sound and digital photography) and radiographic examinations. Examinations were performed by a single researcher visually with ball-ended probes after surface cleaning. All teeth with restorations and prosthetic crowns were excluded from the data and only second digit of ICDAS II were recorded as indices the caries status. Group 1 ICDAS 0 scores has indicated ‘non-carious’; group 2 ICDAS 1-2 were reversible lesion (White spot lesion) and group 3 ICDAS 3,4,5,6 were saved as ‘cavitated carious’ teeth.
Patients were questioned in detail for iron deficiency and whether they have received any treatment for this situation, dietary habits including iron containing foods (red meat, liver, parsley, pumpkin seeds, mussels, legumes, bitter chocolate) the period of time the stains are formed etc. Statistical analysis of data were made using Pearson Chi-Square Test.
Results
There were no caries in the 121 teeth total of 255 teeth examined. The proportion of teeth without caries was found 62.2% and 36.1% respectively among black stained and nondiscolored teeth. The caries status of BS teeth and nondiscolored teeth has shown significantly difference (Chi Square=18.231, p< 0.001). Kappa=0.216, p< 0.001). Therefore, the percentage of being ‘non-carious’ of BS teeth (62.2%) is importantly higher than non-discolored teeth (36.1%).
Kappa is a statistical method that evaluates the fit between two observers. It can be used for a variety of purposes. For example, if "non-discolored" and "BS" examinations done by two people rather than a person, it was necessary to calculate the Kappa index for the analysis of the compatibility between the two, to indicate if they differ. In our study, all teeth were examined by a single examiner, therefore the Kappa value in this paper shows how compatible two groups named “Black Stained” and “Non-discolored” in terms of being "carious" or "non-carious" situation. For this we calculate Kappa=0.216, p< 0.001 for our data. Kappa should have a value between 0 and 1, and the closer the number is to 1, the stronger the fit. Accordingly, Kappa statistics indicate that, there is a moderate (K=0.254) and significant (p< 0.001) agreement between presence of BS and absence of decay.
Additionally, six of total 10 patients were reported as suffering from Fe+ deficiency with different degrees. Four patients were under medication for iron deficiency and the remaining 2 patients were reported to be dietician-controlled.
Discussion
The distribution of the caries cases by the presence of Black Stain (BS) is presented in the Table 1 (Figure 1). As it is seen on the table, the proportion of the teeth without caries is significantly higher among the teeth with BS (36.1%) than the teeth without BS (62.2%), this finding is in accordance with study done by Bath et al, Gasparetto et al. and Koch et al [5,17,18,20].
| Discoloration Status |
Caries Status |
Total |
| Group 1 |
Group 2 (ICDAS 1,2) |
Group 3 |
| (ICDAS 0) |
Reversible lesions |
(ICDAS 3,4,5,6) |
| Non-carious |
Cavitated carious |
| Non-discolored |
Count |
52 |
32 |
60 |
144 |
| % |
36.1% |
22.2% |
41.7% |
100.0% |
| Black Stained |
Count |
69 |
19 |
23 |
111 |
| % |
62.2% |
17.1% |
20.7% |
100.0% |
| Total |
Count |
121 |
51 |
83 |
255 |
| % |
47.5% |
20.0% |
32.5% |
100.0% |
Table 1: The distribution of the caries cases by the presence of Black Stain (BS).
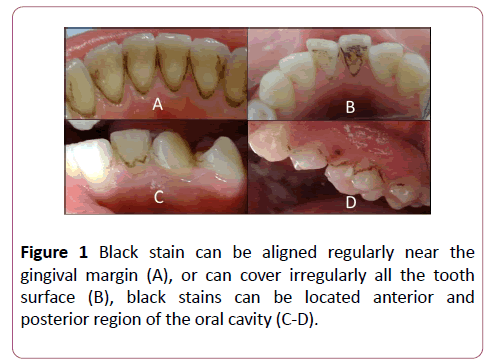
Figure 1: Black stain can be aligned regularly near the gingival margin (A), or can cover irregularly all the tooth surface (B), black stains can be located anterior and posterior region of the oral cavity (C-D).
Recent study on Brazilian population which supports our results has indicated that BS is an inhibitory factor on caries formation [20]. Another study of school-aged children aged 6-12 years in the Potenza area of Italy found that the DMFT records of the mouths with BS were significantly lower and that this correlation would persist in the permanent dentition [5].
While describing black tooth stains, many studies emphasize the location of these stains on the cervical third of the crown [10,12,15]. However, intraoral examinations of our study have shown that these colorations may be present not only in the cervical region but also on the occlusal surfaces (Figure 1). Chromogenic bacteria have been cited for the etiology of these formation and black/brown stains in patients with good oral hygiene and low caries experience [25].
Moreover we observed that stain formation rarely can be seen on restorations such as amalgam and composite fillings (Figure 2). It was also observed that there can be other types of extrinsic discolorations accompanying the black stains (Figure 3).
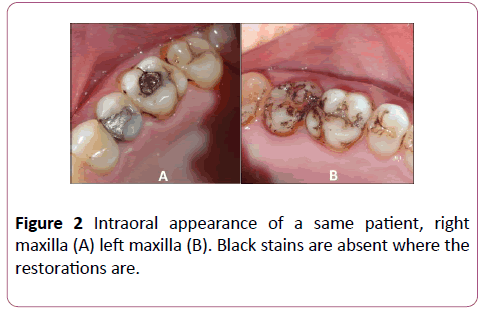
Figure 2: Intraoral appearance of a same patient, right maxilla (A) left maxilla (B). Black stains are absent where the restorations are.
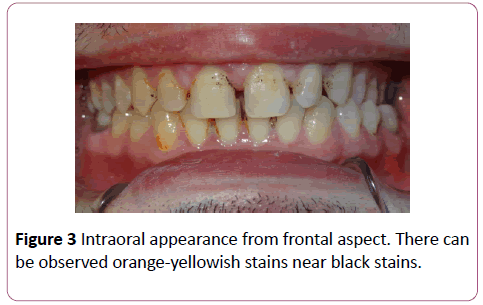
Figure 3: Intraoral appearance from frontal aspect. There can be observed orange-yellowish stains near black stains.
Another question we asked in our study was whether there were any iron deficiencies or iron supplementation in these patients or not. Highly disoriented iron salts of BS have been suggested to be a type of dental plaque in a special structure containing copper, calcium and phosphate [11,26,27]. Studies have been conducted on these stains suggesting that the insoluble iron salts giving black color are ferric sulphite and that this compound has been caused by bacterial hydrogen sulphite and saliva and gingival iron-induced iron reaction [11,28]. It has been shown that iron supplementation drugs or iron-rich diet which increase the amount of iron in saliva, may increase these types of discolorations and enhance bacterial population that causes it [28]. Although, relation between chromogenic bacteria and formation of metal sulfides are frequently presented in studies, no concrete evidence has been showed [8,10,19,25,27,29]. Many studies may be summarized that bacteria related to black stains may create a competitive environment for cariogenic bacteria and this special microflora might reduce caries experience of an individual [13,19,20]. Our findings in this study support that caries formation could be significantly lower in BS teeth.
Conclusion
Black discolored teeth showed less caries scores compared to non-BS teeth. This result can be concluded as that the presence of BS may have preventive effect against caries under the conditions of this pilot study. While the BS formation was local condition, ICDAS II has given tooth-spesific results. We think, further microbiological studies are necessary to examine besides any relation whether BS may protect against caries or not; and the mechanism between Fe+ deficiency, patient’s medication and dietary habits and formation of black stains.
Conflict of Interest
The authors of this paper declare that there is no conflict of interests regarding the publication of this paper.
21525
References
- Akyüz S, Garan A, Kaya MS (2015) Prevalence of black stain and dental caries in children attending a university pediatric dentistry clinic in Istanbul. MUSBED 5: 109-114.
- Hattab FN, Qudeimat MA, Rimawi HS (1999) Dental discoloration: An overview. J Esthet Dent 11: 291-310.
- Sulieman M (2005) An overview of tooth discoloration: Extrinsic, intrinsic and internalized stains. Dent Update 32: 463-471
- Manuel ST, Abhishek P, Kundabala M (2010) Etiology of tooth discoloration-A review. Nig Dent J 18: 2.
- Koch MJ, Bove M, Schroff J, Perlea P, García-Godoy F (2001) Black stain and dental caries in schoolchildren in Potenza, Italy. ASDC J Dent Child 68: 353-355.
- Heinrich-Weltzien R, Bartsch B, Eick S (2014) Dental caries and microbiota in children with black stain and non-discoloured dental plaque. Caries Res 48: 118–125.
- Li Y, Zhang Q, Zhang F, Liu R, Liu H, et al. (2015) Analysis of the microbiota of black stain in the primary dentition. PLOS One 10: e0137030.
- Chen X, Zhan JY, Lu HX (2014) Factors associated with black tooth stain in Chinese preschool children. Clinical Oral Investigations 18: 2059–2066.
- Martin JMG, Garcia MG, Leston JS, Pendas SL, Martin JJD, et al. (2013) Prevalence of black stain and associated risk factors in preschool Spanish children. Pediatrics Int 55: 355–359.
- Zyla T, Kawala B, Antoszewska-Smith J, Kawala M (2015) Black stain and dental caries: A review of the literature. BioMed Res Int.
- Reid JS, Beeley JA (1976) Biochemical studies on the composition of gingival debris from children with black extrinsic tooth stain. Caries Res 10: 363–369.
- Saba C, Solidana M, Berlutti F, Vestri A, Ottolenghi L, et al. (2006) Black stains in the mixed dentition: A PCR microbiological study to the etiopathogenic bacteria. J Clin Pediatr Dent 30: 219-224.
- Slots J (1974) The microflora of black stain on human primary teeth. Scand J Dent Res 82: 484-490.
- Rachid F, Mehdi HE (2016) Black stains in primary teeth: Overview. Pediatr Dent Care 1: 123.
- Suchetha A, Khawar S, Mundinamane DB, Apoorva SM, Bhat D, et al. (2016) All about dental stains: A review. Annals Dent Spec 4: 41-46.
- Ronay V, Attin T (2011) Black Stain-a review. Oral Health Prev Dent 9: 37–45.
- Bhat S (2010) Black tooth stain and dental caries among Udaipur school children. Int J Pub Health Dent 1: 11-15.
- Heinrich- Weltzien R, Monse B, Van Palenstein Helderman W (2009) Black stain and dental caries in Filipino schoolchildren. Community Dent Oral Epidemiol 37: 182-187.
- França-Pinto CC, Cenci MS, Correa MB, Romano AR, Peres MA, et al. (2012) Association between black stains and dental caries in primary teeth: Findings from a Brazilian Population-based birth cohort. Caries Res 46: 170–176.
- Gasparetto A, Conrado CA, Maciel SM, Miyamoo EY, Chicarelli M, et al. (2003) Prevalence of black tooth stains and dental caries in Brazilian School children Braz Dent J 14: 157-161.
- Dikmen B (2015) ICDAS II Criteria International Detection and Assessment System. J Istanbul Univ Fac Dent 49: 63-72.
- Pitts N (2004) ‘ICDAS’– An international system for caries detection and assessment being developed to facilitate caries epidemiology, research and appropriate management. Community Dent Health 21: 193–198.
- Topping GV, Pitts NB (2009) Clinical visual caries detection. Monogr Oral Sci 21: 15-41.
- Chu CH, Chau AM, Lo EC (2013) Current and future research in diagnostic criteria and evaluation of caries detection methods. Oral Health Prev Dent 11: 181-189.
- Watts A, Addy M (2001) Tooth discolouration and staining: a review of the literature. British Dent J 190: 309-316.
- Reid JS, Beeley JA, MacDonald DG (1977) Investigations into black extrinsic tooth stain. J Dent Res. 56: 895–899.
- Tantbirojn D, Douglas WH, Ko CC, McSwiggen PL (1998) Spatial chemical analysis of dental stain using wavelength dispersive spectrometry. Eur J Oral Sci 106: 971-976.
- Adcock KA, Hogan SM (2008) Extrinsic iron staining in infant teeth from iron-fortified formula and rice cereal. J Pediatr Pharmacol Ther 13: 162-165.
- Addy M, Moran J (1995) Mechanisms of stain formation on teeth, in particular associated with metal ions and antiseptics. Adv Dental Res 9: 450–456.


