Case Report - (2015) Volume 3, Issue 4
Chilaiditi's Sign in a Patient on Peritoneal Dialysis
Mak LY1*,Yip PS2 and Yuen MF3
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Queen Mary Hospital, HKSAR, Hong Kong
Division of Nephrology, Department of Internal Medicine, Tung Wah Hospital, HKSAR, Hong Kong
Division of Gastroenterology and Hepatology, Department of Internal Medicine, Queen Mary Hospital, HKSAR, Hong Kong
*Corresponding Author:
Lung-Yi-Mak
Division of Gastroenterology and Hepatology
Department of Internal Medicine, Queen Mary Hospital, HKSAR
Hong Kong
Tel: +852 64310591
E-mail: loeymak@gmail.com
Received date: December 11, 2015; Accepted date: December 28, 2015; Published date: January 03, 2016
Citation:Mak LY, Yip PS, Yuen MF. Chilaiditi’s Sign in a Patient on Peritoneal Dialysis. Ann Clin Lab Res. 2015, 3:4.
Abstract
A 87-year-old gentleman with end stage renal failure on peritoneal dialysis presented to the emergency department for sudden onset shortness of breath. A chest x-ray was obtained, revealing apart from a left sided pneumothorax, there was alarmingly a gas density under the right hemidiaphragm. It is diagnosed as Chilaiditi's sign in a peritoneal dialysis patient.
Case Report
A 87-year-old gentleman, ex-smoker, with end stage renal failure on peritoneal dialysis presented to the emergency department for sudden onset shortness of breath. He is using 2 litres of peritoneal dialysate fluid for dwell, performing 3 exchanges of dialysate per day. A standing chest x-ray was obtained at posterior-anterior view, revealing a left sided pneumothorax, and chest drain was inserted. His left lung reexpaned soon but upon subsequent x-rays, he was found to have gas density shadows under the right hemidiaphragm (Figure 1). The patient did not report any gastrointestinal symptoms, and he had no known liver disease. The patient had another chest x-ray on the same day after he drained out his peritoneal dialysate as per usual peritoneal dialysis schedule, and it showed resolution of the gas density shadows (Figure 2). The diagnosis is Chilaiditi’s sign, which is incidentally found in a patient presented with pneumothorax.
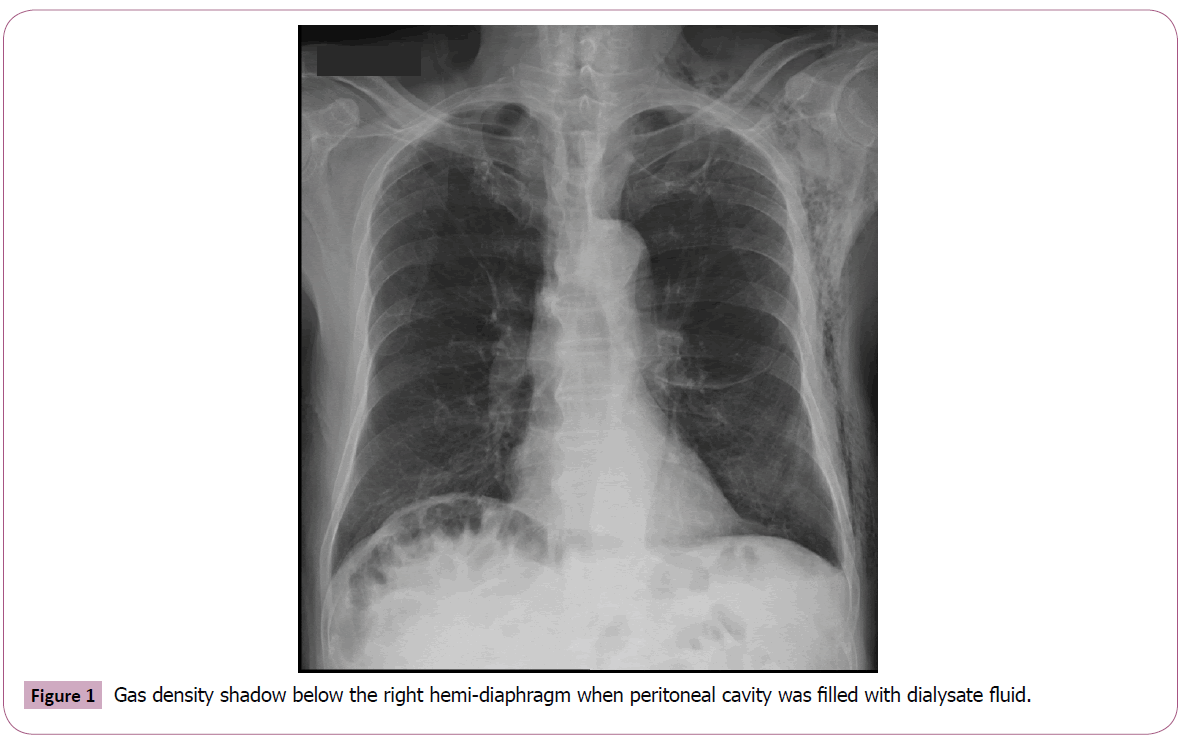
Figure 1: Gas density shadow below the right hemi-diaphragm when peritoneal cavity was filled with dialysate fluid.
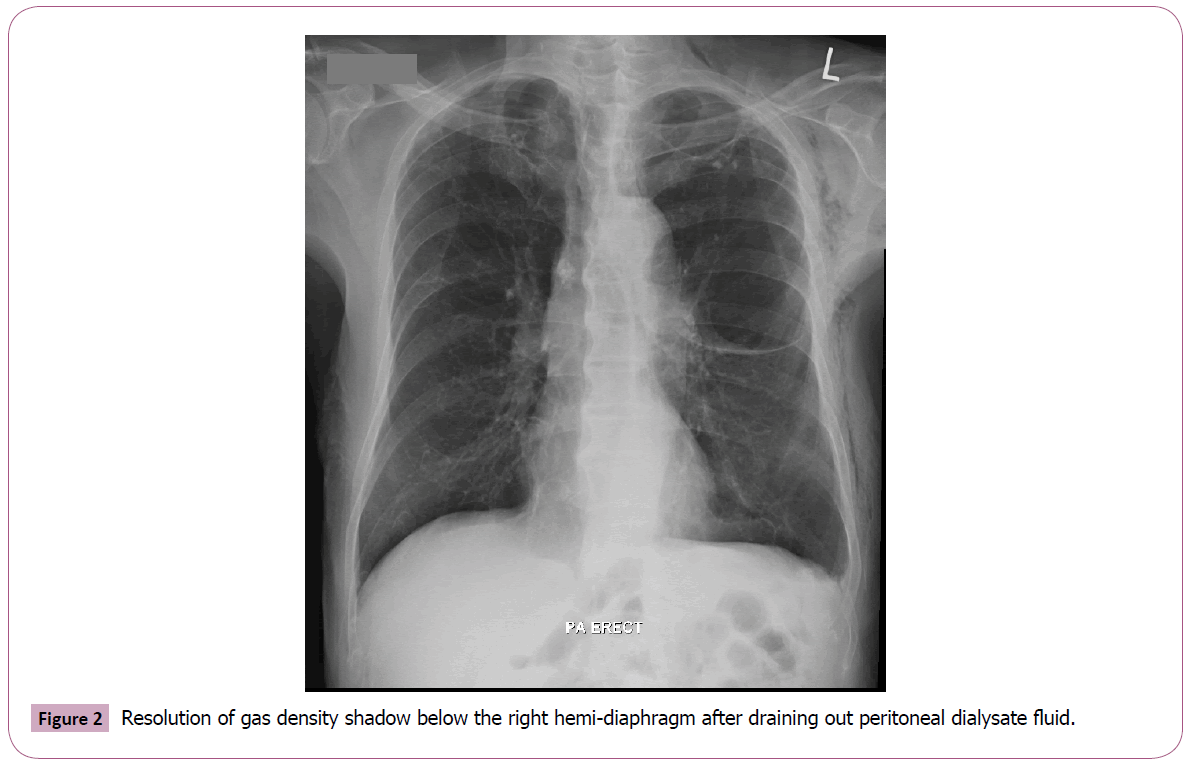
Figure 2: Resolution of gas density shadow below the right hemi-diaphragm after draining out peritoneal dialysate fluid.
Chilaiditi’s sign was first described in 1910 by a Greek radiologist Demetrius Chilaiditi as interposition of small or large bowel loops in the hepatodiaphragmatic space, which is generally an incidental finding [1]. It is regarded as Chilaiditi’s syndrome if the patient develops symptoms involving the gastrointestinal tract, including dyspepsia, abdominal pain, constipation or even intestinal obstruction from volvulus, which is very rare and has only been reported 12 times in the world literature and requires immediate surgical intervention [2]. The infra-diaphragmatic gas density represents intra-luminal air and should be distinguished from pneumoperitoneum.
Chilaiditi’s sign is not an uncommon finding; its incidence in the general population is about 0.28% [3]. Its incidence is higher in patients with cirrhosis with or without ascites. In one observational study, the prevalence was reported to be 5% in patients without ascites; while studies without adjustment for presence of ascites reported the incidence to be as high as 22% (while 73% of them had ascites) [4]. Patients on peritoneal dialysis, by the same token, have higher chance to develop Chilaiditi’s sign. Few reports have been written in patients on peritoneal dialysis [5], and this patient well demonstrated the effect of peritoneal fluid on the bowel loop position, mimicking the effect of ascitic fluid giving rise to Chilaiditi’s sign in cirrhotic patients. Apart from intra-peritoneal fluid due to ascites and peritoneal dialysis, other intestinal, hepatic or diaphragmatic etiologies have also been postulated to contribute to Chilaiditi’s sign such as chronic constipation, aerophagia, chronic lung disease and mental retardation [6]. However, the exact pathogenesis of Chilaiditi’s sign is still unknown.
8033
References
- Nakagawa H (2006) Prevalence and sonographic detection of Chilaiditi’s sign in cirrhotic patients without ascites. American Journal of Roentgenology 187: 589-593.
- Williams A (2004) Chilaiditi's syndrome associated with colonic volvulus and intestinal malrotation-A rare case. Int J Surg Case Rep 5: 335-338.
- Risaliti A (1993) Chilaiditi syndrome as a surgical and nonsurgical problem. SurgGynecolObstet 176:55-58.
- Vessal K, Borhanmanesh F (1976) Hepatodiaphragmatic interposition of the intestine (Chilaiditi's syndrome). ClinRadiol 27: 113-116.
- Ito M (2004) Chilaiditi syndrome in a peritoneal dialysis patient. Kidney Int 86: 214.
- Moaven O, Hodin RA (2012) Chilaiditi syndrome: a rare entity with important differential diagnoses. Gastroenterology &hepatology (N.Y.). 8: 276-278.


