Keywords:
Mortality; Homicide; Colombia; México
Introduction
In the last years, violence and its consequences have obtained major acknowledgment as a topic that generates bigger preoccupation and action in international and regional level. Homicides are the iceberg in this deep and extensive issue. Moreover, it is needed to add other violent facts where there are no fatal outcomes, which causes physical or mental damages (temporal or permanent disabilities) to the victims, to their member families, for example, robberies, assaults, abuses, physical violation, kidnapping, harassment, threats, and highlighted in recent times, the issue of enforced disappearances [1,2].
In 2010, the Americas Region contributed 31% of violent deaths worldwide, near to 144,000 people. The homicide rate per 100,000 populations in all regions increased to 15.6, which represents more than double the world average [3-5]. The countries with the biggest homicides rates in recent years have been Honduras, with a rate above 80 deaths per 100.000 population; Salvador with 67 deaths per 100.000 population, Venezuela with 50 deaths per 100.000 population; Colombia has had a similar rate as in the past decade. Among México, Brazil and Colombia has generated in average 74.000 homicides each year: 11,000 in México, 23,000 in Colombia and 40,000 in Brazil [6-8].
The proportion of homicides in the region, for all ages, show that Brazil had 56% of incidence, while Argentina had 1% of all cases. In-between 2000 to 2009, the homicides rates for young people between 10 to 29 years were up with respect to the general population. In Brazil, they increased 56%, in Colombia 49% and in México 41%. In this group of countries, the risk of death by homicide had increased to almost 50% [4,5,9].
Colombia and Mexico have common characteristics that have been strengths for their social and economic development. Nevertheless, they have also been determinants for the generation of this problem: the presence of two oceans has allowed both sides to export and import illicit drugs. In both countries there is a strong problem of corruption of its ruling parties, confidence in institutions is low [9]. The perception of security is also low [10] assaults, robberies, fights, intolerance and the lack of peaceful resolution of conflicts are present circumstances in cities such as Mexico City, Guadalajara, Monterrey, Bogotá, Cali and Medellín [11-13].
The term violence contains a network of highly complex social relations for which different definitions have been given from different areas of knowledge; however, in the present work we address only that what has been termed as manifest violence, that affects the life or physical integrity of individuals and groups, so that their manifestations are quantifiable; in it the deaths as homicides are registered. In the previous mentioned countries there is sufficient evidence to document this problem by comparing the differences and/or similarities between the two countries that share the category of being dangerous countries in the region.
Based on the above, in this comparative analysis, it tries to pose what has been called the visible part of violence, and that is one in which is presented as a direct, tangible fact that affects the life or physical integrity of individuals or groups so that their manifestations become quantifiable (homicide, suicide, rape, among others). We are aware that this vision leaves out the violence whose causality is directly identified in the structural conditions of society and its consequences cannot be attributed to specific subjects nor can their impact be easily identified. In the world report on violence, this phenomenon is made explicit by pointing out the impossibility of calculating the cost of human affliction and pain, both almost invisible and hardly measurable. In this category violence that is hidden in workplaces is not included even in medical and social institutions responsible for caring for people [1]. Based on the previous description, the objective of this article is to analyze and compare mortality patterns for homicides between two Latin American countries: Colombia and Mexico from 2000 to 2015.
Methodology
Study design
A longitudinal comparative study of mortality by homicidal violence between Colombia and Mexico analyzed from 2000 to 2015. We used databases of both countries: for Colombia, the records from the National Department of Statistics (DANE); [14] for Mexico records from the General Direction of Epidemiology of the Federal Ministry of Health, concentrated in the National Health Information System (SINAIS) [15]. Cause records were extracted from events classified as violent deaths with the codes of the International Classification of Diseases in its tenth version (ICD 10), grouped as follows (Table 1).
| Sl. no |
Death mechanism |
Code ICD |
| 1 |
Strikes without weapons/rape |
Y04 a Y05 |
| 2 |
Poisoning |
X85 a X90 |
| 3 |
Hanging/Strangulation |
X91 a X92 |
| 4 |
Firearm |
X93 a X98 |
| 5 |
Sharp weapon |
X99 a Y00 |
| 6 |
Sharp weapon |
Y06 a Y07 |
| 7 |
Other causes |
Y01 a Y03, Y08 a Y09 |
Table 1: Death mechanism according to the International Classification of Diseases. X version.
Processing of information
The variables analyzed for both countries were: country (Colombia, Mexico), year (2000/2015), age, sex (male, female), death mechanism (Table 1) and entity of occurrence of the death (in Colombia, departments and in Mexico, federal states). Age was grouped generating five-year groups (0 to 4, 5 to 9, 10 to 14, 15 to 24, 25 to 34, 35 to 49, 50 to 64, 65 to 74, and 75 and more). Moreover, age it was divided in less than 10, 10 to 19, 20 to 49, 50 to 59 and up 70 years old. Specific rates were calculated with the population projections reported by the National Population Council for Mexico [16] and by Dane [17] for Colombia. All rates are reported per 100,000 populations.
Analysis of information
A descriptive and trend comparative analysis was carried out by country, year, age groups, sex and geographical region of occurrence of death. Proportion and confidence intervals were obtained (95% CI). The specific mortality rate was calculated according to entity of occurrence of death between the first year and the last year of the period of study. The behaviour of mortality rate was estimated, and moreover, the average rate was calculated for each age group for the study period.
The standardized mortality rates were estimated by country and year of death occurrence, using the direct method of standardization with 95% CI. The population of WHO was used as reference. With this estimation, based on 2000 findings, the risk was established for each country in several mortality categories such as: very low (below 5th percentile), low (between 5th and 25th percentile), medium (between 25th and 50th percentile), high medium (between 50th and 75th percentile), very high (above 95th percentile). These results were geo-referenced in maps. ArgGIS for the geo-referencing was used.
A multivariate analysis was carried out, with logistic regression, anterograde step to step. Country that was used as dependent variable (0=México, 1=Colombia), and as independent variables were used sex (0=female, 1=male), the age variable was re-categorized in the following way: 0=2000/2006, 1=2007/2015. Age variable was worked as a group variable in the previous described groups. The death mechanism variable was handled categorical as described in Table 1, leaving as reference the group blows without weapons/rape. The indicators were analyzed with 95% con CI and significant differences with P values less than 0.05 were taken. All statistical analyzes were performed, using the statistical package Stata version 13.2.
Ethical issues
This work received the approval of the Institute of Public Health of Javeriana University in the Project “After the evidence of the increase in violent mortality in México: Analysis of homicides”.
Results
Between 2000 and 2015, they were 576,998 deaths by homicides in both countries, 55.6% occurred in Colombia.
Colombia
In Colombia, a decreased trend in mortality rate by homicides was observed, in average 20,057 deaths-years and 55 deaths-day. This behaviour changed, they had 87 deathsdays in 2002 to 34 deaths-day in 2015, and it was a descent to about 157%. This decrease was greater in the deaths that occurred in men, with 6.5 deaths less per year, mainly between 20-24 years old, where the decrease it was 15.5 deaths-year.
Analysis by territorial entities: departments (in Colombia) and municipalities, it showed that mortality proportion by homicides was more frequent in those areas with higher poblational density. Antioquia (with 20.7% of all deaths in study period) and Valley of Cauca (18.5%); both departments have cities very permeated by drug cartels: Medellin and Cali, respectively. Between 2002 and 2015 mortality standardized rates in 90.9% of all entities decreased (Figure 1).
In 2000, the departments with higher proportion of mortality were Putumayo, Guaviare and Caquetá. They are located in the Amazonic region, Antioquia, North's Santander, Caldas and Risaralda; they are located in the Andina region. Valley of Cauca is located in the Pacific region. Between 2000 and 2015, several entities in different areas of the country showed a decrease in the proportion of mortality by homicides, such as Guania (87.1%), Antioquia (81%) and Guaviare (79.6%). Nevertheless, they were three entities which increased these proportions: San Andrés (118%), Vichada (78.8%) y Amazonas (5.8%) (Figure 2).
México
In México, the homicides trend in the study period, had increased with an average of 44 deaths-days, but with important changes itself. In 2002, 28 deaths-days occurred, whereas in 2015, they were 57 deaths-days. That situation generated an increase of 105.8%. The average increase was 0.8 deaths-years. It started in 2008, and affected more men with 1,5 death-year and the most affected group was 25-29 years old (Figure 1).
In the Mexican republic, there were increases higher than 100% in Mortality Standardized Rate (Figure 2). It was observed mainly in states such as Zacatecas, Guanajuato, Baja California, Colima, Guerrero, Tabasco, Nuevo León, and Coahuila y Chihuahua. Although in Guerrero the mortality rates climbed to 149%, it was the federative state that registered the mortality rate higher in 2015: 76 deaths per 100,000 populations. Also, it is very important to highlight that in several states the mortality rates declined during the study period. Quintana Roo, Querétaro y San Luis Potosí had the greatest decrease (Figure 2).
The higher proportion of deaths, both in Mexico as in Colombia had occurred in the group of 20-39 years-old, with near to 54.3% and 61.0%, respectively (Table 2). In both countries, the men had been the most affected, with a ratio of 8/1 (Mexico) and 11/1 (Colombia) (Table 2). In both countries, the mechanism of death by homicides that most generated mortality was firearms: 82.0% in Colombia and 61.5% in México. In the second group of causes, sharp weapons were more frequently involved. They were more prevalent in Mexico than in Colombia. In both countries, women were the most affected by this kind of weapon (Table 3).
| Age groups |
Women |
Men |
Total |
| Colombia |
México |
Colombia |
México |
Colombia |
México |
| N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
| <5 |
542 |
2.06 |
1,327 |
4.61 |
678 |
0.23 |
1,682 |
0.74 |
1,220 |
0.38 |
3,009 |
1.18 |
| 5 a 9 |
323 |
1.23 |
510 |
1.77 |
482 |
0.16 |
707 |
0.31 |
805 |
0.25 |
1,217 |
0.48 |
| 10-14 |
765 |
2.91 |
901 |
3.13 |
2,090 |
0.71 |
2,012 |
0.89 |
2,855 |
0.89 |
2,913 |
1.14 |
| 15-19 |
3,541 |
13.47 |
3,293 |
11.44 |
33,871 |
11.5 |
19,089 |
8.4 |
37,412 |
11.66 |
22,382 |
8.74 |
| 20-24 |
4,122 |
15.68 |
3,789 |
13.17 |
57,583 |
19.54 |
33,471 |
14.73 |
61,705 |
19.23 |
37,260 |
14.55 |
| 25-29 |
3,776 |
14.36 |
3,528 |
12.26 |
51,885 |
17.61 |
35,287 |
15.52 |
55,661 |
17.34 |
38,815 |
15.16 |
| 30-34 |
2,979 |
11.33 |
3,210 |
11.15 |
40,686 |
13.81 |
33,375 |
14.68 |
43,665 |
13.61 |
36,585 |
14.29 |
| 35-39 |
2,674 |
10.17 |
2,823 |
9.81 |
31,994 |
10.86 |
29,136 |
12.82 |
34,668 |
10.8 |
31,959 |
12.48 |
| 40-44 |
2,187 |
8.32 |
2,246 |
7.8 |
23,466 |
7.96 |
21,992 |
9.68 |
25,653 |
7.99 |
24,238 |
9.46 |
| 45-49 |
1,595 |
6.07 |
1,712 |
5.95 |
16,795 |
5.7 |
15,916 |
7 |
18,390 |
5.73 |
17,628 |
6.88 |
| 50-54 |
1,114 |
4.24 |
1,309 |
4.55 |
11,309 |
3.84 |
11,157 |
4.91 |
12,423 |
3.87 |
12,466 |
4.87 |
| 55-59 |
663 |
2.52 |
946 |
3.29 |
6,943 |
2.36 |
7,841 |
3.45 |
7,606 |
2.37 |
8,787 |
3.43 |
| 60-64 |
449 |
1.71 |
760 |
2.64 |
4,365 |
1.48 |
5,443 |
2.39 |
4,814 |
1.5 |
6,203 |
2.42 |
| 65-69 |
352 |
1.34 |
655 |
2.28 |
2,686 |
0.91 |
3,871 |
1.7 |
3,038 |
0.95 |
4,526 |
1.77 |
| 70-74 |
252 |
0.96 |
590 |
2.05 |
1,635 |
0.55 |
2,701 |
1.19 |
1,887 |
0.59 |
3,291 |
1.29 |
| 75 and more |
958 |
3.64 |
1,181 |
4.1 |
8,156 |
2.77 |
3,622 |
1.59 |
9,114 |
2.84 |
4,803 |
1.88 |
| Total |
26,292 |
100 |
28,780 |
100 |
2,94,624 |
100 |
2,27,302 |
100 |
3,20,916 |
100 |
2,56,082 |
100 |
Table 2: Comparative Mortality by homicides, quinquenal groups between. Colombia and México. 2000-2015.
Differences
In Mexico, the mortality trend by homicides increased, whereas in Colombia, it declined (Figures 1 and 2). In the study period, there were bigger changes in mortality adjusted rates by homicides for both countries. At the beginning of the period of observation, Colombia had a rate six times higher than Mexico, but this rate dropped in the last years, while in Mexico, this behaviour was opposed. In 2015, the rates ratio between both countries descended to 1.5 times.
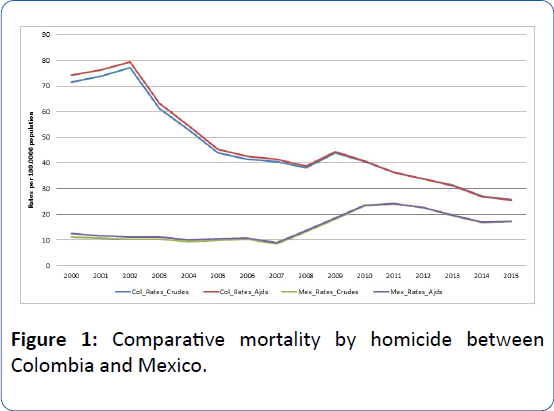
Figure 1: Comparative mortality by homicide between Colombia and Mexico.
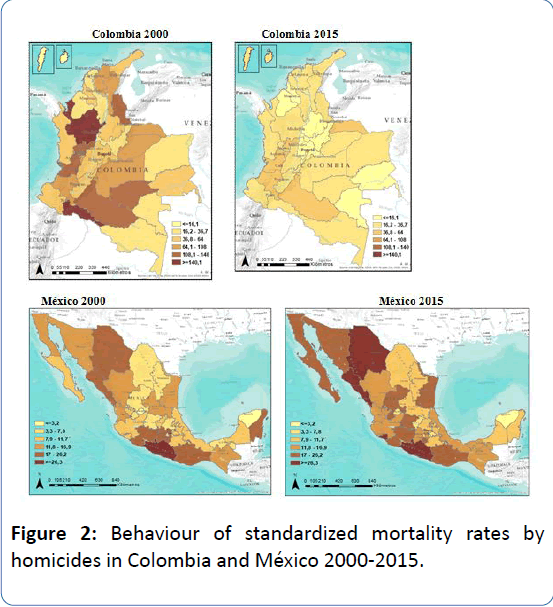
Figure 2: Behaviour of standardized mortality rates by homicides in Colombia and México 2000-2015.
In Colombia, the mortality rate by homicides in the men group of 20-29 decreased. The rates, at the end of the study period dropped to 2/3 parts. Contrary, in México, the men between 20-29 years-old were the ones that mortality rose the most, in average 1,5 times. Mexico showed the higher proportion of deaths by homicides in life extreme ages (less than five years old and 65 years old and up) (Table 2).
The mechanism of death by homicide was classified as other (undetermined), it was porcentually higher (0.4%) in México than in Colombia (0.04%). With respect to women, among the mechanisms more used we could identify which related to physical force such as strangulation, hanging, beatings, poisoning, situations that generated greater suffering; these kind of deaths were more frequent in Mexico than in Colombia. In Mexico, strangulation cases were three times more observed compared to Colombia; in men were similar facts, the hanging was four times more frequent in Mexico (Table 3).
| |
Women |
Men |
Total |
| Colombia |
México |
Colombia |
México |
Colombia |
Mexico |
| N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
N |
% |
| Strikes without weapons/rape |
49 |
0.19 (0.13,0.24) |
323 |
1.12 (1.00,1.25) |
153 |
0.05 (0.04,0.06) |
1,900 |
0.84 (0.79,0.87) |
202 |
0.06 (0.05,0.07) |
2,223 |
0.87 (0.83,0.90) |
| Poisoning |
94 |
0.36 (0.28,0.43) |
292 |
1.01 (0.90,1.13) |
182 |
0.06 (0.05,0.07) |
505 |
0.22 (0.20,0.24) |
276 |
0.09 (0.07,0.09) |
797 |
0.31 (0.29,0.33) |
| Hanging/Strangulation |
1375 |
5.2 (5.0,5.5) |
5,029 |
17.5 (17.0,17.9) |
3,229 |
1.10 (1.05,1.13) |
14,202 |
6.3 (6.1,6.3) |
4,604 |
1.43 (1.39,1.47) |
19,231 |
7.5 |
| Firearm |
18,594 |
70.7 (70.2,71.3) |
11,967 |
41.6 (41.0,42.2) |
2,44,438 |
83.0 (82.8,83.1) |
1,45,545 |
64.0 (63.8,64.2) |
2,63,032 |
82.0 (81.8,82.1) |
1,57,512 |
61.5 (61.3,61.7) |
| Sharp weapon |
5,369 |
20.4 (19.9,20.9) |
5,332 |
18.5 (18.1,19.0) |
42,766 |
14.5 (14.4,14.6) |
34,688 |
15.3 (15.1,15.4) |
48,135 |
15.0 (14.8,15.1) |
40,020 |
15.6 (15.5,15.8) |
| Negligence |
126 |
0.48 (0.39,0.57) |
320 |
1.11 (0.99,1.23) |
153 |
0.05 (0.04,0.06) |
412 |
0.18 (0.16,0.19) |
279 |
0.09 (0.07,0.09) |
732 |
0.29 (0.26,0.30) |
| Other causes |
685 |
2.6 (2.4,2.8) |
5,517 |
19.2 (18.7,19.6) |
3703 |
1.26 (1.21,1.29) |
30050 |
13.2 (13.1,13.4) |
4388 |
1.37 (1.32,1.40) |
35567 |
13.9 (13.6,14.0) |
| Total |
26,292 |
100 |
28,780 |
100 |
2,94,624 |
100 |
2,27,302 |
100 |
3,20,916 |
100 |
2,56,082 |
100 |
Table 3: Comparative Mortality according to death mechanism Colombia-México 2000-2015.
We used multiple analysis, and especially logistic regression, step to step. The country was used as a dependent variable. It was identified that higher death likelihood was found between people that died in Colombia (compared to Mexico) between 10-19 years-old (OR: 1.47 CI 95%:1.38-1.57), with respect to minors than 10 years-old. In other group ages this likelihood was lesser and dropped significantly in people between 50-69 years old (OR: 0.91 CI 95%: 0.85-0.97) with respect to minors than 10 years-old. The death likelihood was slightly higher in men compared to women (OR: 1.07 CI 95%:1.05-1.10). The death likelihood by homicides, for those who died in Colombia with respect to Mexico, was bigger by firearms (OR: 21.5 CI 95%:18.6-24.9) and by sharp weapons (OR: 16.9 IC 95%: 14.6-19.6) (Table 4).
| |
OR |
95% CI |
P Value |
| Age groups |
|
|
|
|
| Less than 10 |
1 |
|
|
|
| 10 to 19 |
1.47 |
1.38 |
1.57 |
0 |
| 20 to 49 |
1.15 |
1.08 |
1.22 |
0 |
| 50 to 69 |
0.91 |
0.85 |
1 |
0.005 |
| 70 and more |
0.71 |
0.66 |
0.77 |
0 |
| Death mechanism |
|
|
|
|
| Strikes without weapons / rape |
1 |
|
|
|
| Poisoning |
3.86 |
3.15 |
4.73 |
0 |
| Hanging / Strangulation |
3.1 |
2.67 |
4 |
0 |
| Firearm |
21.6 |
18.62 |
24.96 |
0 |
| Sharp weapon |
17 |
14.59 |
20 |
0 |
| Negligence |
4.79 |
3.89 |
5.9 |
0 |
| Other causes |
1.51 |
1.3 |
1.76 |
0 |
| Sex |
|
|
|
|
| Women |
1 |
|
|
|
| Men |
1.07 |
1.05 |
1.1 |
0 |
Table 4: Comparative mortality by homicides Colombia México 2000-2015 logistic regression model.
Discussions
Mortality due to homicides is a multifactorial event and for its control and prevention, it needs the design and implementation of multisectorial actions with strong political commitment, huge scholar and laboral opportunities, direct incidence on social economic determinants, among others. In despite of the great decline that was observed in Colombia and the increase that occurred in Mexico, the mortality adjusted rate by homicides in both countries is twice or three times above average with respect to the region,8 wherever the most affected have been men between 15-34 years.
According to WHO, the biological risk factors, in conjunction with individual elements, explain the higher risk of aggressions, which when interacting with circumstances of familiar, social, community and cultural order and other external elements, help in the increase and manifestation of the violent homicides.1 Among the circumstances where aggressive facts are generated we can find fights, robberies and isolated murderer; mainly they are done by delincuencial groups such as gangs, drug traffickers, criminal bands, outlaw groups such as guerrilla, paramilitary or state forces [18-23]. In Colombia, and also in the last years, in Mexico, the main motivator of homicide deaths have been the drug dealing, where organized bands and hired assassin were added. The elimination of cartel leaders has generated division, fight for territories, routes and alliances to produce, store, move and distribute narcotics [7,9,11,24-26].
In Colombia, despite the declining trend in the study period, between 2008 and 2009 occurred a slight increase in the mortality rate, derived from disturbance of public order in Antioquia and Valley departments (together added more than 42% of homicides). That situation was due to the reactivation of criminal bands and reorganization of narcotic groups, among others. Another explanation was the open report about the “false positive phenomenon”, those circumstances generated perverse incentives to military forces if they murdered civilians and after they were presented as killed in combat [27-29].
Some factors have acted in pros and cons of declined mortality rate by homicides in Colombia and the increase in Mexico from 2007. Among others, we can find impunity, corruption (to judges, military, municipal, regional and national authorities, the absence of authority, the lack of government, and minimal social policies of inclusion. All these circumstances increase the “breeding ground”, where the most affected are young people. That situation was planted clearly by WHO in the World Report of 2003 [1,7,24,27].
These findings, partially are coincidence with Hernandez and cols analysis: they reported that northeast states are the most affected by violence and drug trafficking in the last years: Tamaulipas, Chihuahua and Nuevo León [30] Moreover, these states in the north borderline, had complexed situation in violence, similar to reports in other borderlines, for example, borderline Salvador-Guatemala, place used for drug trafficking and where the mortality by homicide has been higher than in other places [31].
In Mexico there has been a high level of corruption in their institutions and military forces, with illegal processes of importation of guns from the USA, which are used no only for illegal and violent operations, but as interchange of drug that narcotrafficants have received from cartels of Colombia, Mexico and Central America [32]. Also, associated to corruption, it is possible to find impunity, with minimal advances in criminal researches, which has happened in those entities with higher level of corruption [33] That situation have antecedents since the 90’s; that has generated the concepts of “Failed States”, weak and with a lot of problems for its performance (lack or weakness in the justice system, huge work in some judges, with skills, materials and humans resources deficient, among others), causing opportunities from members of organized crime that affected them and didn’t let them work with efficiency [13,24,34-36].
It is known that violence not necessarily happens in poverty circles, in other words, not all poor people are violent; nevertheless, it is true that social inequality or depressed environments have higher likehood of occurrence of violence [5]. The entities (states and departments) where more deaths due to homicide have occurred, they weren’t among those poorest in both countries. In Colombia: Antioquia and Valle have contributed with more than 41% of deaths. However, they weren’t the departments with the worst social economic conditions, although in each city it is possible to see some circumstances associated with inequality processes. For example, Medellin, Antioquia's capital had the higher Gini in home in the middle of the study period [9,37-39].
In México, there are different studies that had reported that political empresarial elites had been promoters of inequality social processes [40,41]. Some authors had reported that in México “There are notorious inequity in health associated with higher levels of social exclusion”, that had been reflected in mortality excess in some municipals with higher or very higher margination index located in states such as Chiapas, Oaxaca and Guerrero [6]. That situation has been used by delincuencial groups who offer benefits, better incomes to people of excluded zones or with higher level of margination.
In Colombia, there are some explanatory hypothesis about the decline observed, based on studies and local reports. From 2002 was priorized in a public agenda, the Politics of Democratic Security, which maybe, contributed to the decrease of the mortality rate by homicide [42]. Moreover, from the 90’s, several Mayors of the bigger cities created politics for restrictions in carrying firearms, to alcohol ingestion and strengthening of the public forces to control and reduce the organized delinquents [43,44].
The experience in control of firearms started from 1993 in Cali and from 1997 in Bogotá; based on that practice was constituted how one security strategy flag's. After, in the beginning of new millennium, that strategy was adopted in Medellin and neighboring municipalities, moreover in other capital cities such as Bucaramanga, Pereira, Cucuta and Cartagena [45,46]. In Cali, it was observed that during the times of restriction of alcohol consumption, that the Mortality rate by homicides dropped [47,48].
It is necessary to have caution with the results shown in this article due to some possible limitants. Firstly, the information about deaths in each countries could have sub register problems or wrong classification. Nevertheless, this condition is less possible because both organizations that produce this information (DANE in Colombia and SINAIS in México) have evaluation and rigorous reclassifications systems that minimize the possible measurement mistakes. The second, we didn’t made analysis by socioeconomic stratum neither by social stratum or education level for each country due to information in the last variable (schooling) had sub register up to 20%; it is possible that some imputation processes could have improve that problematic situation.
The third, the source of secondary registries by homicides didn’t identify motives, causes or determinants likely associated to the occurrence of these events (impossible to identify if they were fights, intolerance, drug trafficking, passional problems, revenge acts, among others). For this reason, the hypothesis that we have done are expeculatives, based on literature revision, according to the experience and work of each author by country. However, in spite of all these possible limitants, this work joins to the evidence body and findings of this issue. It generates hypotheses about behavior of violent deaths in two Latin American countries, which have more than 50% Spanish speech population in the region, with some characteristics in common but also with some differences.
Beyond these limitations that we can find in mortality analysis by potential problems in some sources consultated, the evidence reviewed, it constitutes patterns, differences and similarities with relation to a common phenomenon that both Latin American Countries have lived. Also, let to identify and compare some specific characteristics, which are causing this public health problem, involving mainly people in productive ages. It is necessary; from these finding to generate new research questions with the purpose of controlling the consequences most severe to violence, where one the biggest findings had been the different patterns to execute violence against women in Mexico.
From some years, several public health experts, with respect to mortality by homicides, have suggested the need of designing and implementing inclusive preventive actions, “without neglecting the care and rehabilitation of those affected” [1,5,11,12]. Although there are evidences that repressive systems with strong institutions have caused a drop in homicides rates, also it is important to design and promote inter-sectorial strategies to improve higher connivance and welfare level for people both countries [49,50]. Ideally, the interventions must be designed, planned, accorded and implemented with the accompaniment of affected communities, and the support of the civil society, academic people, guils, and local government, if not, it will be difficult to leave this vicious circle.
It is imperative to continue professionalizing the police members, to increase training processes and wages, and mainly, to extract them from the corruption circles. A state policy, it is necessary which not only would impact the mortality by violence, but also other public health events, where it would be possible to promote some mechanisms to distribute the wealth. This would improve the inequality and would impact several events of external causes and others that produce high burden disease such as peri and maternal events, cardiovascular events, metabolic events, among others [51,52].
Acknowledgements
This work was possible thanks to the internal project supported by Pontifical Javeriana University of Bogota. In addition, we are very grateful to the National Institute of Public Health of Mexico, National Institute of Health of Colombia and Entornos Foundation, which supported the academic work of other authors.
23876
References
- Krug E, Dahlberg L, Mercy J, Zwi A, Lozano R (2003) Violence, A global public health problem. Pan American Health Organization, USA.
- Buvinic M, Morrison A (1999) Violence as an obstacle to development. Econo Soc Cons Viol 9: 1-8.
- UNODC (2015) World drug report. United nations office on drugs and crime, Vienna, Austria.
- Briceño-León R (1999) Violence and despair; The other social crisis in Latin America. Latin America Today, Spain.
- Briceño-León R (2008) Homicidal violence in Latin America. Latin America Today, Spain.
- Gonzáles-Pérez G, Vega-López M, Romero-Valle S, Cabrera-Piraval C (2008) Social exclusion and inequity in health in Mexico: A Socio-spatial Analysis. Pub Health 10:15-28.
- Dávila-Cervantes CA, Pardo-Montaño AM (2014) Magnitude and trend of mortality from homicides in Colombia and Mexico, 2000-2011. Rev Panam Salud Publica 36:10-16.
- Pan American Health Organization (2014) Health surveillance and disease prevention and control health information and analysis. Basic health indicators of the Americas for 2011-2012. PAHO, USA.
- Cohen M, Rubio M (2007) Violence and crime in Latin America solutions paper. Copenhagen consensus center and the Latinobarómetro corporation report. Inter-American development bank, Saint Joseph, USA.
- Concha-Eastman A. Crime and violence: causes and prevention policies. Measurement of violence: conceptual and practical problems. Pan Am Health Org 20: 201.
- Concha-Eastman A (2000) Violence is preventable. A challenge for the municipalities. Program of non-communicable diseases, division of control and prevention of diseases. Pan Am Health Org 20: 001.
- Escalante F (2009) Can Mexico be Colombia? violence, drug trafficking and state. New Society 220: 84-96.
- NDS (2016) National department of statistics. Population projections for Colombia, departments, age groups and sex, Colombia.
- NIPHM (2016) Federal health secretariat. National health information system of the general directorate of epidemiology. National institute of public health, Mexico.
- CONAPO (2015) National population council. Projections data of Mexico 1990 to 2005, Italy.
- Ahmad O, Boschi-Pinto C, López A, Murray C, Lozano R (2018) Age standardization of rates. WHO, Geneva, Switzerland.
- NILMFC (2014) National institute of legal medicine and forensic sciences. National reference center group on violence. Behavior of the homicide. Colombia 2014. Forensic data for life, Colombia.
- INEGI (2015) National institute of geography and statistics of Mexico. Preliminary data of homicides to 2014, Mexico.
- Portillo N (2003) Studies on youth gangs in El Salvador and Central America: a review of their participatory dimension. Notes of Psychol 21: 475-493.
- Liebel M (2004) Youth gangs in Central America or the difficult search for justice in a violent society. Desacatos J Soc Sci 14: 85-104.
- Velásquez-Rivera E (2007) History of Paramilitarism in Colombia. History 26:134-153.
- Lasso-Toro P (2004) When the uprooting is lived. Education and forced displacement: A look from the Aguablanca District, William of Ockham, UK.
- Cubides F (2004) Drug trafficking and war in Colombia: The paramilitaries. In violence and collective strategies in the Andean region: Bolivia, Colombia, Peru and Venezuela, IFEA-IEPRI-Norma, Columbia.
- Rubio M (2005) The Mara trout and voracious. Organized Youth Violence in Central America. Inter-American Development Bank, Working Paper, USA.
- Montoya-Prada A (2009) Wage earners of death. Sicariato and criminality in Colombia. Lat Am Cit Secur 9: 61-74.
- Cardona M, García H, Giraldo C, López M, Suárez C, et al. Homicides in Medellín, Colombia, between 1990 and 2002: actors, motives and circumstances. Cad Saude Public 21: 840-851.
- Pachón M (2009) Successes, dangers and failures of the democratic security policy of the Álvaro Uribe administration. Politic science, Colombia.
- CINEP (2009) Popular research and education center, Special report April 2009-False positives, CINEP, Columbia.
- Hernández-Bringas H, Narro-Robles J (2010) The homicide in Mexico, 2000-2008. Population Papers. 63: 243-271.
- Dudley S (2010) Drug trafficking organizations in Central America: Carriers, Mexican Cartels and Maras. University of San Diego, California. USA.
- Arias-Henao D (2014) Construction of narco identities in Colombia and Mexico. International relations, Geneva, Switzerland.
- Gonzáles-Pérez G, Vega-López M, Cabrera-Pirava C, Vega-López A, Muñoz A (2012) Mortality due to homicides in Mexico: trends, socio-geographical variations and associated factors. Cien Saude Colet 12: 3195-3208.
- Chabat N (2005) Drug trafficking and state: The discreet charm of corruption. Letras Libres, Mexico.
- Morales-Oyarbide C (2011) The war against drug trafficking in Mexico. Weakness of the state, local order and failure of a strategy. Social Sci 50: 1-35.
- Emmerich N (2014) Corruption, politics and drug trafficking. work document. Faculty of studies for graduates. University of Belgrade, Serbia.
- Duque L, Klevens J, Montoya N (2005) Socially undesirable behaviors associated with aggressors and resilient. A case-control study in Medellín, Colombia 2003-2005. Public Health Fac 25: 21-36.
- Bonilla-Mejía L (2008) Regional differences in the distribution of income in Colombia. Working document on regional economy. Bank of the Republic. Cartagena, Columbia.
- Tejada D (2012) Social production of violence in Santiago de Cali: an exploration from social mediators. Fac. Nac. Pub Health 30(1): 57-59.
- Alonso A (2010) The political-business elites as promoters of social inequality in Mexico. Under the volcano, Reynal & Hitchcock publishers, UK.
- Eibenschutz C, Támez C (2008) Inequality and erroneous social policies produce inequity in Mexico. Pub Health 10: 119-132.
- Salas-Quijano S, Chaparro-Narváez P, Cotes-Cantillo K, León W, Castañeda-Orjuela C, et al. (2005) Homicidal violence in Colombia: Another relevant problem in public health. Strategic monitor J Med 8: 67-71.
- Casas DP (2005) Urban security and police in Colombia. Security and democracy foundation, Columbia.
- Moreno C, Cendales R (2011) Mortality and potential years of life lost due to homicides in Colombia, 1985-2006. Rev Panam Public Health 30: 342-353.
- Aguirre K, Restrepo J (2010) The control of weapons as a strategy to reduce violence in Colombia: relevance, status and challenges. Criminal Mag 52: 265-284.
- Wallace A (2014) Epidemiology to fight murders: The recipe that works for Cali, BBC Mundo, UK.
- United Nations Office on D Crime (2014) Global study on homicide 2013: trends, contexts, data, Geneva, Switzerland.
- Sanchez A, Villaveces A, Krafty R, Park T, Weiss HB, et al. (2011) Policies for alcohol restriction and their association with interpersonal violence: A time-series analysis of homicides in Cali, Colombia. Int J Epidemiol 11: 1-10.
- Carrión F (2003) From urban violence to citizen coexistence "Between crime and punishment, citizen security and democratic control in Latin America and the Caribbean Ed. Lilian Bobea, Caracas: New Society, Bepress, USA.
- Cívico A (2015) Rudolph Giuliani and urban security, Espectador, Columbia.
- Cortez A (2006) Inequality, poverty and health in Colombia. Medical Colombia, University Hospital in Medellín, Colombia.
- Zurita B, Lozano R, Ramírez T, Torres J (2003) Inequality and inequity in health. Kaleidoscope of health, UK.


