Kamaldeep Singh1, Savita Devi1 and Pranay P Pankaj2*
1Lovely Faculty of Applied Medical Sciences, Lovely Professional University, Punjab, India
2Department of Zoology, Nagaland University, Lumami, Nagaland, India
*Corresponding Author:
Pranay P Pankaj
Department of Zoology, Nagaland University, Lumami-798 627, Nagaland, India
Tel: +919771162090
E-mail: pranaypunj@gmail.com
Received March 14, 2016; Accepted April 05, 2016; Published April 08, 2016
Citation: Singh K, Devi S, Pankaj PP (2016) Diabetes Associated Male Reproductive Dysfunctions: Prevalence, Diagnosis and Risk Factors. Int J Drug Dev & Res 8: 007-010
Keywords
Diabetes mellitus; Male reproductive dysfunctions; Delayed sexual maturation; Glycaemic control; Retrograde ejaculation; Sexual performance
Introduction
DM is an idiopathic disease that deals with the chronic metabolic disorder of carbohydrate, lipid and protein by occurrence of improper secretion and action of insulin or both. Secondary complications like arteriosclerosis, nephropathy, neuropathy and microanginopathy can also devoted through DM [1]. The characteristics symptoms may present with DM are polyuria, polydipsia, blurring of vision and body weight loss [2]. The harshness depends on how long presence of disease and how much time it took to be controlled. In modern societies, the DM is one of the most leading public health threats worldwide and its prevalence is increasing more rapidly day by day [3,4].
Sexual dysfunction (SD) is linked to DM has already been perceived earlier in 10th century. Pathogenesis may include vascular insufficiency, neuropathy and some psychological problems [5,6] which later on develop into SD such as impotence or ED, ejaculation disorder (pre mature or delayed ejaculation) and decrease libido [7,8].
DM is responsible for biochemical variations and other pathological changes which dramatically leads to disturbance in spermatogenesis [9], retrograde ejaculation [10] or ED and ends up with decrease sexual appetite. DM is reported for reduction of sperm quality and function due to alteration in testicular cells and concerned hormones particularly sex hormones due to failure of glucose homeostasis [11-14]. Decreased motility, vitality of semen and semen ejaculation without change in viscosity were already observed in insulin dependent diabetes mellitus (IDDM). Plasma levels of testosterone, FSH and LH were infancy in such subjects [15].
Most of the complications due to DM have been studied widely but SDs related to male are still incompletely understood. The aim of the present review is to discuss diabetic effects on male reproductive functions, its prevalence, suggested risk factors and etiological pathways.
Prevalence of DM associated SD in male
The worldwide frequency of IDDM is differing from its low range of 1-2 per 100,000 in Japan to a more than 40 per 10,000 in Finland. The predictions of data for NIDDM are more difficult due to its heterogeneity in appearance though 5-7% prevalence rate had been noted worldwide. Report hypothesized that DM had very little complication upon male infertility or RD. Similar report on prevalence of ED indicated that patients who had such disorder and hospitalized were found to be increased with age. Prevalence rate in males with age of 20-24 years recorded were 5.7% which rose up to 52.4% in aged between 55-59 years.
Johannes et al. estimated ED were ≥ 50% of man with DM worldwide. ED comes within 10 years after first diagnosis of DM and its percentage is to be higher than non diabetic male. The chance of occurrence of insulin resistance (%) is 3 times more prone in men with ED [15]. It is reported that men with DM may develop ED within 5-10 years. The 6% and 52% prevalence rates were seen in age group between 20-24 years and 55-95 years respectively [16-18].
Similar studies done by Richardson and Vinik in patients suffering from type 1 DM since 10 years; ED were observed in 1.1%, 55% and 75% of men in age group of 21-30 years, 50-60 years and the age more than 60 years respectively [19]. It was also reported that IDDM counted to 40% whereas 52% occupied in impotence by NIDDM. Overall the proper explanation on prevalence of ED in DM through studies did not differentiate between T1DM and T2DM.
Clinical features and risk factors
Generally two major types of sexual problems are observed in diabetic patients. First major type of sexual problem is associated with hyperglycaemia which resulted into reduction in sexual appetite, progression of erectile failure, lethargy, tiredness and malaise whereas second type of sexual problem comprises disturbances of sexual functions by progressive and irreversible decline in sexual function, impotence as well as psychological stress.
Undoubtedly in DM, the most prominent sexual problem is difficulty in maintaining or obtaining erection due to neuropathy. ED is correlated with poor metabolic control, advancing in age, neurological damage, consumption of alcoholic beverages, progression of DM, drug addiction, micro and macro vasculopathy and other factors [20]. Clinically, most information related to ED in diabetics is hidden due to social stigma which finally leads to continuous and progressive deprivation of energy in trying of erection activity (Figure 1). Severity of ED increased with advancing age day by day with change in shape of penis and penile trauma caused during erection along with premature ejaculation [21].
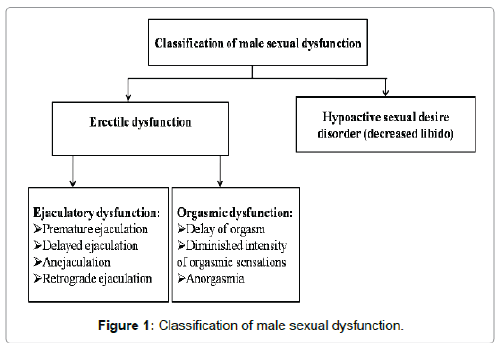
Figure 1: Classification of male sexual dysfunction.
Altered ejaculation such as retrograde ejaculation in which semen flow backward direction in to the bladder instead of flowing through anterior urethra is one of the common problems in DM [22]. Passed urine ejaculation appears cloudy which further can be diagnosed by high number of spermatozoa in urine. In one of the study, only 1.08% persons have been noted with retrograde ejaculation on other hand 45.94% persons were found to be impotent within population although studies were still inadequate regarding prevalence of ejaculatory alteration induced from DM.
Progression of DM may lead to complication of infertility and testicular atrophy [22]. Mild glucose intolerance or controlled diabetics with less fertility and sperm density are not affected in spermatogenesis [23] though the alteration in sperm motility from DM is still debated [24]. Other abnormalities including decreased tubules diameter, hyalinized tubular walls, cellular debris or occluded lumina from epithelial cells, exfoliated germ cells, abnormalities in sertoli cells and leydig interstitial cells as well as micro-vascular changes were already reported.
Approximately 30-60% of diabetic men have been observed suffered from erectile impotence and its prevalence depends mainly upon age factors. In general, impotence due to DM has been divided into two main categories: first category usually occurs when diagnosis of erectile failure observed during the treatment of poor glycaemic control. It consists of loss of sexual drive in erectile failure from various degrees of induction. On other hand second type is characterized with progressive and irreversible decline in sexual function as in longer standing of DM [25].
Moreover other common related risk factors which are recognized as to develop ED in diabetic men include hyperglycaemia, hypertension, obesity, sedentary lifestyle, smoking, metabolic syndrome and autonomic neuropathy [16,26-28]. Some diabetic complications such as micro vascular [29-31] and macro vascular [32,33] also play important role to increase the risk for developing ED in diabetic men. Generally patients are using large number of drugs to manage DM which further may cause SD either by effecting on ejaculation through penis function or sex drive. Literature survey revealed that subjects with increased BMI and T1DM were at higher risk as compared to increased BMI and T2DM.
Some other risk factors which are associated with DM that reduce sexual interests are depression [34], hypogonadism [35-38], coronary artery disease, renal failure and use of certain drugs such as antidepressant or antihypertensive (Figure 2).
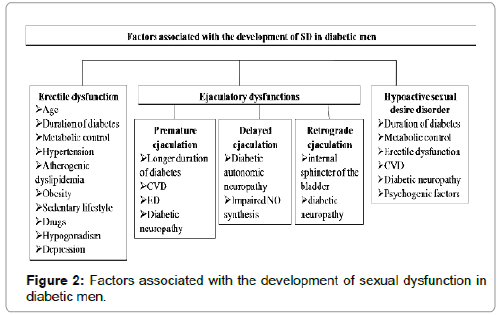
Figure 2: Factors associated with the development of sexual dysfunction in diabetic men.
Etiological factors and patho-physiology of SD
The etiologies of SDs are mainly based on physical and psychological factors. SD is developing in a complex psychosomatic fact in which physical and psychological factors are widely involved. One study reported that DM had damaging effects on testosterone production which further effect on local endocrine transmitters by impaired LH response to GnRH stimulation of basal normal gonadotropin levels. Similarly young diabetic men with good glycaemic control had increased basal LH level as well as GnRH stimulation response.
Recent researches revealed that abnormalities in internal arteries which are associated with stenosis and atheroma altered the blood supply to erectile tissue and cells which further rose impotence or SD in diabetic men. There are some evidences which suggested that pelvic autonomic neuropathy have major contribution to ED of many diabetic men.
The patho-physiology of ED in diabetic men is multifactorial and no single cause is reasonable. DM further rises to development of advance glyceted end products (AGEs). Generally, the formation of AGEs are based upon the non enzymatic reaction between glucose and lipoprotein or nucleic acid [39] which leads to decrease thickening, elasticity, increase atherosclerosis and conversion in endothelial function [40]. The relationship between AGEs with diabetic ED is based on generation of free radical oxygen which comes from quenching of NO and oxidative cell damage have major role in relaxation of cavernosum smooth muscle. High levels of effects are particularly seen on the potassium channel which is mainly responsible for subsequent relaxation of cavernosal smooth muscles and intracellular facilitation of the release of calcium. Early development of diabetic ED takes place on damage of potassium channels [41].
Micro-vascular and macro-vascular prominent complications arose in DM particularly from peripheral neuropathy and autonomic neuropathy [42]. Most of the literature survey shown early autonomic and somatic nerve dysfunction was seen in diabetic patients. A central neuropathic mechanism may also play critical role to the neuropathy induced by DIED [43].
Production of NO takes place from the endothelium of arteries of the penis. The formation of cGMP does not going to interfere with NO in relaxation of the corpus cavernosum [44] whereas the high level of superoxide radicals present at cavernosal tissue. DIED have decreased level of NO synthase that results into another possible pathways leading to smooth muscle and cavernosal dysfunction [45]. It is also hypothesized that guanylyl cyclase activity impairs in DM by decreased production of cGMP. Furthermore, ineffective endothelial dysfunction rapidly delivers the functional syncytium of the corpora cavernosa that leads to decrease NO and cGMP that involve significantly in the development of diabetes ED [46].
Recent researches have shown that the transduction pathway for endothelial involving GTP-binding protein, Rho-kinase, RhoA and its effectors agent might play a role in development of diabetic ED. It is suggested that the RhoA/Rho-kinase pathway interfere ED through decreased production of NO in the penis [47].
Conclusion
DM is a growing public health leading disease, which causes cardiovascular, psychological, and sexual dysfunctions. It is well known cause of MSD, with prevalence rates approaching 50% in both type 1 and T2DM. Day by day, the prevalence of MSD in diabetic patients is increasing. The pathophysiology of DM induced MSD is multi factorial and no single etiology is at the forefront. The major problems that can be observed after DM induced MSD are erectile dysfunction, retrograde ejaculation, altered spermatogenesis and impotence. Researches reveal that there are many hormones which can alter the production of testosterone, but correct aetiology is still a mystery. So in that condition, need to more work out for identification of specific aetiology for DISD (Figure 3). If we talk about it treatment, there were no such particular treatment for DISD. SD can by controlled and prevent from further enhancement by some therapy like medical, surgical, alternative and behaviour therapy. However the medical therapy can help in prevention of SD that includes testosterone replacement therapy and intracavernosal vasoactive injection.
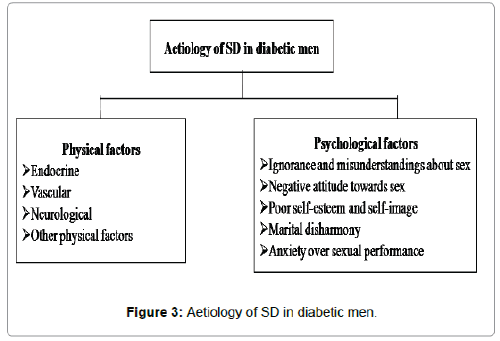
Figure 3: Aetiology of SD in diabetic men.
9483
References
- Pankaj PP, Varma MC (2013) Potential role of Spirulinaplatensis in retaining altered blood parameters in alloxan induced diabetic mice. Int J Pharm Pharm Sci 5: 450-456.
- Pankaj PP (2015) Efficacy of Spirulinaplatensis in improvement of the reproductive performance and easing teratogenicity in hyperglycemic albino mice. Indian J Pharmacol 47: 430-435.
- Priyadarshani N, Pankaj PP, Varma MC (2010) Evaluation of estrous cycle in normal and alloxan-monohydrate induced diabetic Swiss albino mice- Musmusculus. Columban J Life Sci 11: 97-101.
- Priyadarshani N, Pankaj PP, Varma MC (2011) Hypolipidemic effects of aqueous leaf extract of Moringaoleifera Lam. (Moringaceae) in alloxan induced diabetic mice- Musmusculus. J Haematol & Ecotoxicol 6: 81-90.
- Pankaj PP (2011) Hypoglycemic activity of Aloe vera juice in alloxan induced diabetic mice- Musmusculus. Modern J Life Sci 1: 85-90.
- Devi S, Singh K, Pankaj PP (2016) Prevalence, pathogenesis and diagnosis of sexual dysfunctions in diabetic women. Int J Pharm Bio Sci 7: 221-225.
- Macfarlane I, Bliss M, Jackson JGL, Williams G (1997) The history of diabetes. In: Pickup J, Williams G (eds.), Textbook of Diabetes. 2nd edn. Oxford: Blackwell Science,pp: 1-19.
- Clark W (2004) Testosterone and diabetes. What's the connection? Diabetes Self Manag 21: 100-103.
- De Berardis G, Pellegrini F, Franciosi M, Belfiglio M, Di Nardo B, et al. (2007) Clinical and psychological predictors of incidence of self-reported erectile dysfunction in patients with type 2 diabetes. J Urol 177: 252-257.
- Fedele D (2005) Therapy Insight: sexual and bladder dysfunction associated with diabetes mellitus. Nat Clin Pract Urol 2: 282-290.
- Stanworth RD, Kapoor D, Channer KS, Jones TH (2011) Dyslipidaemia is associated with testosterone, oestradiol and androgen receptor CAG repeat polymorphism in men with type 2 diabetes. ClinEndocrinol (Oxf) 74: 624-630.
- Maric C, Forsblom C, Thorn L, Waden J, Groop PH (2010) Association between testosterone, estradiol and sex hormone binding globulin levels in men with type 1 diabetes with nephropathy. Steroids 75: 772-778.
- Miralles-García JM, García-Díez LC (2004) Specific aspects of erectile dysfunction in endocrinology. Int J Impot Res 16 Suppl 2: S10-12.
- Chandrashekar V, Bartke A (2005) The impact of altered insulin-like growth factor-I secretion on the neuroendocrine and testicular functions. Minerva Ginecol 57: 87-97.
- Johannes CB, Araujo AB, Feldman HA, Derby CA, Kleinman KP, et al. (2000) Incidence of erectile dysfunction in men 40 to 69 years old: longitudinal results from the Massachusetts male aging study. J Urol 163: 460-463.
- Giuliano FA, Leriche A, Jaudinot EO, de Gendre AS (2004) Prevalence of erectile dysfunction among 7689 patients with diabetes or hypertension, or both. Urology 64: 1196-1201.
- Guay A, Jacobson J (2007) The relationship between testosterone levels, the metabolic syndrome (by two criteria), and insulin resistance in a population of men with organic erectile dysfunction. Journal of Sexual Medicine 4: 1046-1055.
- Roth A, Kalter-Leibovici O, Kerbis Y, Tenenbaum-Koren E, Chen J, et al. (2003) Prevalence and risk factors for erectile dysfunction in men with diabetes, hypertension, or both diseases: a community survey among 1,412 Israeli men. Clin Cardiol 26: 25-30.
- Richardson D, Vinik A (2002) Etiology and treatment of erectile failure in diabetes mellitus. CurrDiab Rep 2: 501-509.
- Kleinman KP, Feldman HA, Johannes CB, Derby CA, McKinlay JB (2000) A new surrogate variable for erectile dysfunction status in the Massachusetts male aging study. J ClinEpidemiol 53: 71-78.
- Fairburn CG, Wu FC, McCulloch DK, Borsey DQ, Ewing DJ, et al. (1982) The clinical features of diabetic impotence: a preliminary study. Br J Psychiatry 140: 447-452.
- Greene LF, Kelalis PP (1968) Retrograde ejaculation of semen due to diabetic neuropathy. Journal of Urolog 98: 693-696.
- Rodriguez-Rigau LJ (1980) Diabetes and male reproductive function. Journal of Andrology 1: 105-110.
- Hicks JJ, Rojas L, Rosado A (1973) Insulin regulation of spermatozoa metabolism. Endocrinology 92: 833-839.
- Fairburn CG, McCulloch DK, Wu FC (1982) The effects of diabetes on male sexual function. Clin Endocrinol Metab 11: 749-767.
- Ponholzer A, Temml C, Mock K, Marszalek M, Obermayr R, et al. (2005) Prevalence and risk factors for erectile dysfunction in 2869 men using a validated questionnaire. EurUrol 47: 80-85.
- Bortolotti A, Fedele D, Chatenoud L, Colli E, Coscelli C, et al. (2001) Cigarette smoking: a risk factor for erectile dysfunction in diabetics. EurUrol 40: 392-396.
- Nicolosi A, Moreira ED Jr, Shirai M, Bin MohdTambi MI, Glasser DB (2003) Epidemiology of erectile dysfunction in four countries: cross-national study of the prevalence and correlates of erectile dysfunction. Urology 61: 201-206.
- Siu SC, Lo SK, Wong KW, Ip KM, Wong YS (2001) Prevalence of and risk factors for erectile dysfunction in Hong Kong diabetic patients. Diabet Med 18: 732-738.
- Vinik AI, Maser RE, Mitchell BD, Freeman R (2003) Diabetic autonomic neuropathy. Diabetes Care 26: 1553-1579.
- Chew SK, Taouk Y, Xie J, Nicolaou TE, Wang JJ, et al. (2013) Relationship between diabetic retinopathy, diabetic macular oedema and erectile dysfunction in type 2 diabetics. Clin Experiment Ophthalmol 41: 683-689.
- Heruti RJ, Uri I, Arbel Y, Swartzon M, Galor S, et al. (2007) Erectile dysfunction severity might be associated with poor cardiovascular prognosis in diabetic men. J Sex Med 4: 465-471.
- Chew KK, Bremner A, Jamrozik K, Earle C, Stuckey B (2008) Male erectile dysfunction and cardiovascular disease: is there an intimate nexus? J Sex Med 5: 928-934.
- Anderson RJ, Freedland KE, Clouse RE, Lustman PJ (2001) The prevalence of comorbid depression in adults with diabetes: a meta-analysis. Diabetes Care 24: 1069-1078.
- Kapoor D, Aldred H, Clark S, Channer KS, Jones TH (2007) Clinical and biochemical assessment of hypogonadism in men with type 2 diabetes: correlations with bioavailable testosterone and visceral adiposity. Diabetes Care 30: 911-917.
- Dhindsa S, Prabhakar S, Sethi M, Bandyopadhyay A, Chaudhuri A, et al. (2004) Frequent occurrence of hypogonadotropichypogonadism in type 2 diabetes. J Clin Endocrinol Metab 89: 5462-5468.
- Mulligan T, Frick MF, Zuraw QC, Stemhagen A, McWhirter C (2006) Prevalence of hypogonadism in males aged at least 45 years: the HIM study. Int J ClinPract 60: 762-769.
- Chandel A, Dhindsa S, Topiwala S, Chaudhuri A, Dandona P (2008) Testosterone concentration in young patients with diabetes. Diabetes Care 31: 2013-2017.
- Romeo JH, Seftel AD, Madhun ZT, Aron DC (2000) Sexual function in men with diabetes type 2: association with glycemic control. J Urol 163: 788-791.
- Wang H, Eto M, Steers WD, Somlyo AP, Somlyo AV (2002) RhoA-mediated Ca2+ sensitization in erectile function. J Biol Chem 277: 30614-30621.
- Büyükafar K, Un I (2003) Effects of the Rho-kinase inhibitors, Y-27632 and fasudil, on the corpus cavernosum from diabetic mice. Eur J Pharmacol 472: 235-238.
- Ming XF, Viswambharan H, Barandier C, Ruffieux J, Kaibuchi K, et al. (2002) Rho GTPase/Rho kinase negatively regulates endothelial nitric oxide synthase phosphorylation through the inhibition of protein kinase B/Akt in human endothelial cells. Mol Cell Biol 2: 8467-8477.
- Rees RW, Ziessen T, Ralph DJ, Kell P, Moncada S, et al. (2002) Human and rabbit cavernosal smooth muscle cells express Rho-kinase. Int J Impot Res 14: 1-7.
- Bivalacqua TJ, Champion HC, Usta MF, Cellek S, Chitaley K, et al. (2004) RhoA/Rho-kinase suppresses endothelial nitric oxide synthase in the penis: a mechanism for diabetes-associated erectile dysfunction. ProcNatlAcadSci USA 101: 9121-9126.
- Chua R, Tar M, Melman A, Di Santo ME (2006) Streptozotocin induced diabetes results in time-dependent up regulation of the endothelin/rho-kinase pathway in rat corpus cavernosum smooth muscle. J Sex Med 3: 25.
- Costabile RA (2003) Optimizing treatment for diabetes mellitus induced erectile dysfunction. J Urol 170: S35-38.
- Park JK, Lee SO, Kim YG, Kim SH, Koh GY, et al. (2002) Role of rho-kinase activity in angiotensin II-induced contraction of rabbit clitoral cavernosum smooth muscle. Int J Impot Res 14: 472-477.


