Keywords
Disease trends; cVDPVs; Democratic Republic of Congo
Background
Immunization of children with multiple doses of oral poliovirus vaccine (OPV), using both routine immunization (RI) and supplementary immunization activities (SIAs) remain essential in poliomyelitis eradication [1]. The key advantages of OPV include ease of administration and efficient induction of mucosal immunity, thereby limiting poliovirus shedding and person-to-person transmission [1]. However, the OPV contains a live, attenuated vaccine-virus. When this vaccine is administered, the attenuated vaccine virus replicates in the intestine and enters into the blood stream triggering a protective immune response [2]. During the replication process of attenuated vaccine-virus, some viruses may mutate and become neurovirulent [3]. This neurovirulent virus is referred to as vaccine-derived poliovirus (VDPV) [4]. VDPVs are further categorized as 1) cVDPVs when evidence of person-to-person transmission in the community exists; 2) iVDPVs, which are isolated from persons with primary immunodeficiencies; and 3) aVDPVs, which are either clinical isolates from persons with no known immunodeficiency and no evidence of transmission, or sewage isolates that are unrelated to known cVDPVs or iVDPVs and whose source is unknown [5,6]. cVDPVs differ from the majority of vaccine-related isolates by having genetic properties consistent with prolonged replication or transmission [4]. Based on molecular characteristics, it has been reported that there was evidence of multiple genetic recombination events between poliovirus and other non-polio enteroviruses, particularly coxsackievirus [7]. cVDPVs are operationally defined as OPVrelated isolates having >1% nucleotide (nt) sequence divergence from the parental OPV strain (usually determined by sequencing the genome region encoding the major viral surface protein, VP1) [6]. The vaccine-virus is able to circulate in communities for a prolonged period of time uninterrupted, can mutate and reacquire neurovirulence which could cause paralysis [8]. As longer the population immunity is lower, these viruses can survive, replicate and exchange genetic material with other enteroviruses as they spread through a community [8,9]. But in case of the population which is fully immunized against poliomyelitis, it will be protected against the spread of both WPV and cVDPVs [9].
In 2000, about 18 countries in the world have reported poliomyelitis outbreaks associated with cVDPVs [10]. In Africa; several countries were affected including Madagascar in 2001-2002 and 2005 [11], in the Northern states of the Nigerian Federation (2005-2015), in Cameroon, Chad and the Democratic Republic of Congo (DRC) [9]. However, the number of countries with circulation of indigenously emergent cVDPVs decreased from 18 countries in 2000 to four (Pakistan, Nigeria, Madagascar, and South Sudan) in 2015. This substantial achievement could chiefly be attributed to the high quality of Acute Flaccid Paralysis (AFP) surveillance in conjunction with wide coverage of immunization of children [8]. Indeed, the solution to eliminate cVDPVs in the community is the same for all polio outbreaks: vaccinate every child several times with oral polio vaccine to stop polio transmission, regardless of whether the virus is WPV or cVDPVs. Since the key factors of VDPV emergence include 1) continued use of OPV at low rates of coverage; 2) prior elimination of the corresponding WPV serotype, emphasis on use of monovalent OPV and bivalent OPV (types 1 and 3) in mass campaigns; 3) poor AFP surveillance. It is crucial to begin the introduction of inactivated polio vaccine (IPV), which is not associated with cVDPVs and boosts immunity when administered in combination with OPV.
The aim of this study was to determine the disease trend and the genetic makeup of cVDPVs strains isolated in DRC during 2008-2016.
Materials and Methods
Study design
A retrospective descriptive study was conducted using secondary AFP surveillance data routinely collected from 2008 to 2016 by NRPL located at Kinshasa. All AFP cases reported nationwide during the studied period were considered for this study.
Virus isolation using RD and L20B cell lines
Stool samples collected from AFP patients were processed in the laboratory according to WHO manual, 2004 [12]. Briefly, chloroform-treated and clarified 20% (weight/volume) stool suspensions were prepared from stool specimens and inoculated onto monolayer Human rhabdomyosarcoma (RD) and murine L20B (a derivative of murine L cells expressing the PV human receptor) cells. Inoculated cells were observed daily for the appearance of cytopathic effect (CPE). Positive cultures were harvested and stored at -20°C while negative cultures were observed for five days and re-passaged onto a new monolayer for additional five days (Figure 1). Isolates showing CPE on L20B were selected as polioviruses (PVs) and subjected to further characterization as described below.
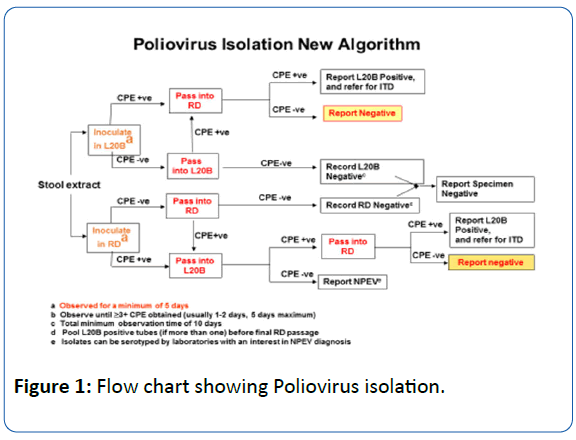
Figure 1: Flow chart showing Poliovirus isolation.
Molecular characterization
Intratypic differentiation by real time polymerase chain Reaction
Poliovirus serotyping was performed by real-Time Reverse Transcriptase Polymerase Chain Reaction using cell culture supernatants according to the protocol recommended by WHO [8,9]. The Intratypic differentiation (ITD) method was carried out using PVs group, serotype-specific, and Sabin strain-specific primers sets, in order to determine whether the PVs isolated are from the wild type, sabin strain or cVDPV and the serotype involved [13].
RNA extraction and genomic amplification and sequencing for VDPV type
After the identification of cVDPVs by ITD method, the cell culture supernatants of cVDPVs isolates were extracted using QIAamp® Viral RNA Mini Kit according to the manufacturer’s instructions (Qiagen, Courtaboeuf, France). The amplification of the full-length VP1 protein coding gene was done using specific primers reported elsewhere [14]. VDPV from DRC were sequenced by Sadeuh et al, following the manufacturer’s protocol; briefly: After purification using QIAquick Gel Extraction kit (Qiagen, Courtaboeuf, France). Purified PCR products were subjected to direct sequencing using the Big Dye terminator v3.1 kit (Applied Biosystems) and an ABI Prism 3140 automated sequencer (Applied Biosystems). The sequencing of each amplicon was performed in both directions using PCR primers as reported [7,14,15].
Results and Discussion
Socio demographic features
During the study period, a total of 71 cVDPV cases were obtained. Two largest outbreaks occurred in 2010 and 2012 with 19, and 17 cases (Table 1). The majority of cases were provided by Katanga followed by Maniema Province. However, few cases were reported from Bandundu Province (Table 1). Most of cVDPVs cases were children under 5 years of age and 80% infected children had known immunization status, fever and experienced sudden onset of paralysis. The number of males affected was more than that of females (Table 2). Eighty percent of VDVPs cases occurred during the rainy season versus 20% in the dry season.
| Year |
Source of isolates |
Province |
cVDPVs by serotype |
Total |
| cVDPV1 |
cVDPV2 |
cVDPV3 |
| 2008 |
AFP patients |
KAT, ORT |
- |
13 |
- |
13 |
| 2009 |
AFP patients |
KAT, KOC |
- |
5 |
- |
5 |
| 2010 |
AFP patients |
MAN, KOC, EQ |
- |
19 |
- |
19 |
| 2011 |
AFP patients |
KAT |
- |
13 |
- |
13 |
| 2012 |
AFP patients |
KAT |
- |
17 |
- |
17 |
| 2013 |
AFP patients |
|
|
0 |
|
0 |
| 2014 |
AFP patients |
KAT |
- |
1 |
- |
1 |
| 2015 |
AFP patients |
BDD |
- |
1 |
- |
1 |
| 2016 |
AFP patients |
ORT, EQ |
- |
2 |
- |
2 |
Province Abbreviation: KAT=Katanga, ORT=Province Orientale, KOC=Kasai Occidental, MAN=Maniema, EQ= Equateur, BDD= Bandundu
Table 1: Circulating Vaccine-derived polioviruses (cVDPVs) detected in DRC, 2008-256 2016.
Cells line culture
A total of 16,649 stools samples were collected through the country during the study period (n=16,649, most of the cases had two stool samples collected at an interval of 24-48 hrs). The cells line culture was carried out at the NRLP in Kinshasa. Thus, virus isolation using RD and L20B cell lines classified 1,040 isolates as PVs since they have showed CPE effect on L20B cell line while 998 isolates showed only CPE effect on RD suggesting that they could be non-polio enterovirus (NPEV). All isolates which did not grow in cell culture and were considered as free of enterovirus.
Molecular characterization
The ITD by Real time Polymerase Chain Reaction was carried out at the National Reference Polio laboratory (NRPL) in Kinshasa, capital city of DRC. Of the 1,040 isolates classified as PVs: 201 were classified as WPVs, 71 as cVDPVs, and 768 as OPV strains. All cVDPVs collected, were characterized as cVDPV type 2.
As demonstrated by others, studies done on sequencing of cVDPV from DRC, reported various genetic recombination to other human enteroviruses of species C (HEV-C), especially coxsakievirus A (CV-A): CV- A11, CV-A13, CV-A17, and CV-A20 [15,16].
Discussion
One of the main goals of the WHO Global Polio Eradication Initiative (GPEI) has been the live, attenuated OPV [17,18]. Once WPV transmission has been stopped globally like in the DRC, the vaccine-viruses will be the only source of live polioviruses in the community and could potentially lead to the re-emergence of polio. Therefore, AFP surveillance and children immunization play a key role [19,20]. Accordingly, the AFP surveillance team in conjunction with the DRC Expanded Program for immunization (EPI) resolved to eliminate all cVDPVs outbreaks nationwide. Thus, the two largest cVDPV outbreaks occurred in 2010 and 2012 were rapidly stopped with 2-3 rounds of high-quality supplementary immunization activities. Our findings were similar to the study done in Madagascar and in Pakistan, suggesting that high rates of OPV coverage prevents all poliovirus spread, including spread of VDPVs [11,21]. The comparison of clinical features between cVDPVs and other patients with AFP showed that non-significant differences were observed, since all groups of patients presented with similar clinical features. Similarly, previous studies done in Nigeria reported similar results [22]. However, children under 5 years of age and males were more infected than other age groups. This could be related to the immune response which is not stronger in this age group (Table 2) [22]. Most cases of cVDPVs occurred during the rainy season, specifically between January-April and September-December. One of the reason could be because the transmission into humans seems to be during high the rainy season than dry season. All cVDPVs outbreaks with increased cases number occurred in DRC, exhibited the risks accompanying low Rate of Immunization OPV coverage and underscored the need to balance poliovirus immunity to all serotypes in all populations. Indeed, counter measures against cVDPVs have been taken, thus since 2014 the cases of cVDPV isolates declined significantly (Table 1). Overall, all cVDPV reported in this study were classified as cVDPV type 2 (cVDPVs 2). Since the WPV2 was eradicated worldwide in 1999, therefore the weakened type 2 strains in trivalent OPV is no longer needed to protect children from wild polio, but causes 90% of all cVDPV. Switching to bivalent OPV that does not contain the type 2 component will reduce the risk of cVDPV. As described by Sadeuh et al, preliminary studies on cVDPVs from DRC, HEV- C seems to be a priviled recombinants with mutated OPV, particularly the CV-A ( CV-A13, CV-A17, CV-A11, CV-A20) [15,23].
| Age Group |
Total Number |
Sex |
Immunization Status |
Clinical Symptoms |
| M |
F |
<3 dose |
>3 dose |
Unknown |
Fever |
Asymmetrical |
Paralysis Onset |
| 0-5 |
69 |
39 |
30 |
50 |
15 |
4 |
69 |
0 |
69 |
| 6-11 |
2 |
2 |
0 |
0 |
0 |
2 |
2 |
0 |
2 |
| >12 Years |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
0 |
Table 2: Circulating Vaccine-derived polioviruses (cVDPVS) Characteristics by age 258 group in DRC, from 2008-2016.
Conclusion
From 2008 to 2016, the cases of cVDPVs in DRC decreased significantly. Although WPV and cVDPVs have virtually disappeared since 2012 and 2014 respectively, it is recommended to follow up steps to stop cVDPVs and avoid potential cVDPVs re-emergence. Since Coxsakievirus seems to be the OPV privileged partner for recombination, it is crucial to investigate the role of others non-polio enterovirus among AFP patients.
Declaration
Ethics approval and consent for participating and publishing
There is no special ethical approval granted since the poliomyelitis sentinel surveillance protocol was implemented as part of routine public health surveillance by the Ministry of Health and was therefore considered a service. Verbal informed consent was obtained from the parents or caregivers of each child before his/her sample collection in order to participate at any enteroviruses study involving their stools samples and publish results for improving healthcare.
Competing interest
Authors declare no competing interest.
Funding
HK was financially supported by the INTRA-ACP Mobility (scholarship for postgraduate student).
Acknowledgment
The authors are grateful to all the staff from the Virology Department of Institut National de Recherche Biomedicale (INRB) in Kinshasa for their direct and indirect contributions to this work.
20009
References
- Centers for Disease Control and Prevention (2009) Progress toward interruption of wild poliovirus transmission worldwide. MMWR Morb Mortal Wkly Rep 59: 545-550.
- Sutter RW, Kew OM, Cochi SL, Aylward RB (2013) Poliovirus vaccine-live. In: Plotkin SA, Orenstein WA, Offit PA, eds. Vaccines. Sixth ed. London, England, pp: 598-645.
- Sutter RW, Kew OM, Cochi SL, Plotkin SA, Orenstein WA, et al. (2008) Poliovirus vaccine-live, Vaccines, 5th eds, WB Saunders Company, Philadelphia, pp: 631-685.
- Kew OM, Sutter RW, de Gourville EM, Dowdle WR, Pallansch MA (2005) Vaccine-derived polioviruses and the endgame strategy for global polio eradication. Annu Rev Microbiol 59: 587-635.
- Burns CC, Diop OM, Sutter RW, Kew OM (2014) Vaccine-derived polioviruses. J Infect Dis 1: S283-S293.
- Diop OM, Burns CC, Wassilak SG, Kew OM (2013) Update on vaccine-derived polioviruses-worldwide. MMWR Morb Mortal Wkly Rep 63: 242-248.
- Kilpatrick DR, Ching K, Iber J, Chen Q, Yang SJ, et al. (2014) Identification of vaccine-derived polioviruses using dual-stage real-time RT-PCR. J Virol Methods 197: 25-28.
- World Health Organization (2016) Global Polio Eradication Initiative. Polio this week as of 04 May 2016. Geneva, Switzerland.
- Sadeuh-Mba SA, Bessaud M, Massenet D, Joffret ML, Endegue MC, et al. (2013) High frequency and diversity of species C enteroviruses in Cameroon and neighboring countries. J Clin Microbiol 51: 759-770.
- Adu FD, Iber J, Bukbuk D (2007) Isolation of recombinant type 2 vaccine-derived poliovirus (VDPV) from a Nigerian child. Virus Res 127: 17-25.
- Rakoto-Andrianarivelo M, Rousset D, Razafindratsimandresy R, Chevaliez S, Guillot S, et al. (2005) High frequency of human enterovirus species C circulation in Madagascar. J Clin Microbiol 43: 242-249.
- Stanway G, Williams CH (2009) Enteroviruses and Diabetes. J Med Virol 81: 200.
- Kilpatrick DR, Nottay B, Yang CF, Yang SJ, Da Silva E, et al. (1998) Serotype-specific identification of polioviruses by PCR using primers containing mixed-base or deoxyinosine residues at positions of codon degeneracy. J Clin Microbiol 36: 352-357.
- Bessaud M, Jegouic S, Joffret ML, Barge C, Balanant J, et al. (2008) Characterization of the genome of human enteroviruses: design of generic primers for amplification and sequencing of different regions of the viral genome. J Virol Methods 149: 277-284.
- Sadeuh-Mba SA, Kavunga H, Joffret ML, Yogolelo R, Endegue-Zanga MC, et al. (2016) Enterovirus Genetic landscape and macro evolution among coxsakieviruses A and Vaccine-derived Polioviruses in the Democratic Republic of Congo.
- Gumede N, Lentsoane O, Burns CC, Pallansch M, de Gourville E, et al. (2013) Emergence of vaccine-derived polioviruses, Democratic Republic of Congo, 2004-2011. Emerg Infect Dis 19: 1583-1589.
- Joffret ML, Jegouic S, Bessaud M, Balanant J, Tran C, et al. (2012) Common and diverse features of cocirculating type 2 and 3 recombinant vaccine-derived polioviruses isolated from patients with poliomyelitis and healthy children. J Infect Dis 205: 1363-1373.
- Combelas N, Holmblat B, Joffret ML, Colbere-Garapin F, Delpeyroux F (2011) Recombination between poliovirus and coxsackie A viruses of species C: A model of viral genetic plasticity and emergence. Viruses 3: 1460-1484.
- Centers for Disease Control and Prevention (2006) Progress toward interruption of wild poliovirus transmission-worldwide, January 2005-March 2006. MMWR Morb Mortal Wkly Rep 55: 458-462.
- Tebbens RJ1, Pallansch MA, Kew OM, Cáceres VM, Jafari H, et al. (2006) Risks of paralytic disease due to wild or vaccine-derived poliovirus after eradication. Risk Anal 26: 1471-1505.
- Burns CC, Shaw J, Jorba J (2013) Multiple independent emergences of type 2 vaccine-derived polioviruses during a large outbreak in northern Nigeria. J Virol 87: 4907-4922.
- Wassilak S (2001) Outbreak of Type 2 Vaccine-Derived Poliovirus in Nigeria: Emergence and widespread circulation in an underimmunized population. J Infect Dis 7: 898-909.
- Sadeuh-Mba S, Bessaud M, Massenet D, Joffret ML, Endegue MC, et al. (2012) Enteroviruses in Cameroon and neighbouring countries: High frequency and diversity of species C enteroviruses. J Clin Microbiol.


