Ping-I Lin1,2*, Drew H Barzman2,3
1Division of Biostatistics and Epidemiology, Cincinnati Children’s Hospital Medical Center, Ohio, USA
2Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati College of Medicine, Ohio, USA
3Division of Child and Adolescent Psychiatry, Cincinnati Children’s Hospital Medical Center, Ohio, USA
*Corresponding Author:
Ping-I Lin
Cincinnati Children's Hospital Medical Center
MLC, 5041 3333 Burnet Avenue
Cincinnati, OH, 45229 USA
Tel: 513-636-0000
E-mail: pingi.lin@gmail.com
Citation: Lin PI, Barzman DH. Disentangling Cognitive Defects in Chronic Depression and Repetitive Mild Traumatic Brain Injury. J Neurol Neurosci. 2016, 6:3. doi: 10.21767/2171-6625.100024
Received Date: July 13, 2015; Accepted Date: November 02, 2015; Published Date: November 04, 2015
Keywords
Depression; Mild traumatic brain injury; Cognitive defects; Medial temporal lobe dysfunction
Introduction
It has been estimated that 15-35% of patients with mild traumatic brain injuries (mTBI) might suffer from subsequent depressive disorder [1,2]. Patients with post-mTBI depression have reported more cognitive symptoms [3,4]. On the other hand, mTBI superimposed on depressive disorder may increase the risk of suicidal attempts [5]. Specifically, mTBI-related depression may be characterized by depressive rumination and impaired autobiographical memory [6]. Here, we presented a case report of repetitive mild traumatic brain injury and chronic depression, of which the neuropathology was confirmed using the neuroimaging study.
Case description
Ms. C is a 52-year-old female patient, who started to experience mixed depressed and anxious moods at the age of 35. After two mild traumatic brain injuries (mTBI) due to repetitive suicidal attempts, she began to show aggravated depressed mood. Her depression-related symptoms included anhedonia, rumination, and somatic delusions centered on her excessive concerns about bowel movements (e.g., she felt that she became “overweight” due to feces in her colons, although her body mass index was only 19). She kept asking the clinician to prescribe more high-potency laxatives to her despite repetitive reassurances. Her depressive symptoms had limited responses to selective serotonin reuptake inhibitor, serotonin norepinephrine reuptake inhibitor, and triclyclic antidepressant for 2 months. Under the impression of repetitive mTBI superimposed on chronic depression with cognitive impairments, we performed Mini-Mental State Examination (MMSE) at two time points (on admission date and 28th day during this hospitalization).
We hence speculated that her cognitive impairments might stem from specific form of cerebral dysfunctions, such as frontal lobe lesions. Therefore, we administered Frontal Assessment Battery (FAB) test on the 28th day and found her FAB score was 11 (maximal score is normally 18 from six items). Her performance was particularly poor at two items: “Conflicting instructions (sensitivity to interference)” and “Go–No-Go (inhibitory control).” Her Wechsler Adult Intelligence Scale--Revised (WAIS-R) test shows that her FIQ, VIQ, and PIQ, were above average, respectively. Additionally, she was found to have poor performances in visual searching and graphical memory tasks. Her Mini-Mental State Examination (MMSE) score was consistently normal (30 out of 30) throughout the treatment course. We further used single-photon emission computed tomography (SPECT) with Technetium-99m (Tc-99m) and found perfusion defects at bilateral medial temporal lobes (Figure 1). After augmented antipsychotic medications, including quetiapine (500 mg/day) and aripiprazole (15 mg/day), we began to notice the improvement of depressive symptoms (Hamilton-Depression Rating Scale score dropped below 12) on 60th day, while her FAB score remained 11 (out of 18). However, her ruminations and suicidal ideations became less frequent. Therefore, she was discharged and received outpatient care at a regular basis.
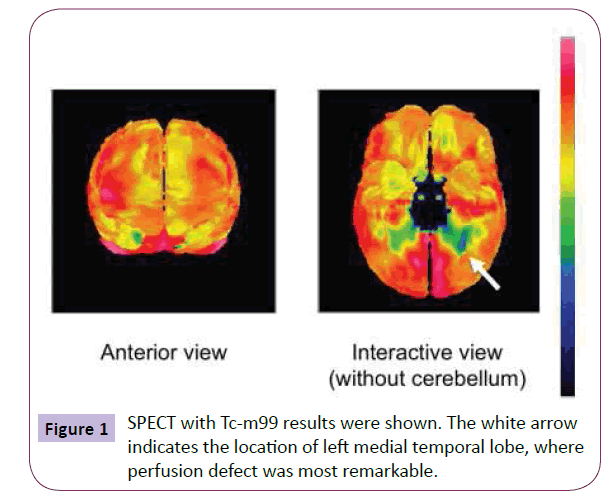
Figure 1: SPECT with Tc-m99 results were shown. The white arrow indicates the location of left medial temporal lobe, where perfusion defect was most remarkable.
Discussion
In the current report, we have described a patient with repetitive mTBI superimposed on her depressive disorder, and how her neuroimaging findings might explain her atypical clinical course. The patterns of her symptoms were speculated to stem from mild cognitive defects, which might be attributable to either chronic depression or repetitive mTBI.
Although the patient’s SPECT results did not show perfusion defects in the frontal lobe, the patient’s mild frontal lobe function impairment might stem from the medial temporal lobe impairment that impacted the fronto-temporal network defects [7]. We noticed that while her depressed mood was improved, the severity of her frontal-lobe impairments remained the same. Therefore, her atypical cognitive symptoms were likely driven by repetitive mTBI rather than chronic depression. However, her probable somatic delusion partially subsided after her depressed mood was improved. It is likely that her somatic delusion might have been attributable to both her severe depressed mood and asymmetric temporal lobe perfusions. Previous studies have reported that various types of somatic delusion may be associated with asymmetric temporal lobe perfusions [8-10]. Specifically, medial temporal lobe dysfunctions are characterized by impaired declarative memory, working memory, spatial perception, and visual discriminating capacities [11,12]. Therefore, the patient’s cognitive deficits and delusion were likely related to medial temporal lobe dysfunctions. In addition, repetitive mTBI may also cause accumulation of phosphorylated tau protein in neurons and astrocytes in a pattern that is unique from other tauopathies, such as Alzheimer's disease; such tau abnormalities lead to perivascular neurofibrillary tangles and neuritis, which predispose to degeneration affecting medial temporal lobe [13]. The system consists of the hippocampal region and the adjacent perirhinal, entorhinal, and parahippocampal cortices [14], and hence functional disturbances in this region can cause a wide range of mild cognitive impairments.
In summary, we have demonstrated a case with mTBI superimposed on depressive disorder. The patient’s clinical presentation (i.e., treatment-resistant, repetitive suicidal attempts, somatic delusion, and specific cognitive defects in memory and spatial perceptions) were partially consistent with medial temporal lobe dysfunction commonly seen in repetitive mTBI. Our patient’s clinical presentations were only partially consistent with typical symptoms related to with medial temporal lobe dysfunction, while her somatic delusions could not be explained by medial temporal lobe dysfunction. On the other hand, her chronic depression could not account for most specific cognitive deficits, which might be more likely to be attributable to mTBI, but might have exacerbated those symptoms. Therefore, some, but not all, of these cognitive deficits were moderately alleviated after her depressive symptoms subsided.
The current SPECT findings might lend some support to this pathological process related to repetitive mTBI with the lesion located in the medial temporal lobes. Treating depression may improve cognitive deficits following mTBI [15], which we observed in this case. Further research is warranted to clarify clinical and neurobiological correlates that may predict the prognosis for this condition.
Acknowledgements
P-I.L. and DB are supported by Cincinnati Children’s Hospital Research Foundation.
7179
References
- Busch CR, Alpern HP (1998) Depression after mild traumatic brain injury: a review of current research. Neuropsychol Rev 8: 95-108.
- Rapoport MJ, McCullagh S, Streiner D, Feinstein A (2003) The clinical significance of major depression following mild traumatic brain injury. Psychosomatics 44: 31-37.
- Lange RT, Iverson GL, Rose A (2011) Depression strongly influences postconcussion symptom reporting following mild traumatic brain injury. J Head Trauma Rehabil 26: 127-137.
- Rapoport MJ, Kiss A, Feinstein A (2006) The impact of major depression on outcome following mild-to-moderate traumatic brain injury in older adults. J Affect Disord 92: 273-276.
- Oquendo MA, Friedman JH, Grunebaum MF, Burke A, Silver JM, et al. (2004) Suicidal behavior and mild traumatic brain injury in major depression. J NervMent Dis 192: 430-434.
- Bessell AL, Watkins ER, Williams WH (2008) Depressive rumination reduces specificity of autobiographical memory recall in acquired brain injury. J IntNeuropsycholSoc 14: 63-70.
- Rao V, Mielke M, Xu X, Smith GS, McCann UD, et al. (2012) Diffusion tensor imaging atlas-based analyses in major depression after mild traumatic brain injury. J Neuropsychiatry ClinNeurosci 24: 309-315.
- Uezato A, Yamamoto N, Kurumaji A, Toriihara A, Umezaki Y, et al. (2012) Improvement of asymmetrical temporal blood flow in refractory oral somatic delusion after successful electroconvulsive therapy. J ECT 28: 50-51.
- Hayashi H, Akahane T, Suzuki H, Sasaki T, Kawakatsu S, et al. (2010) Successful treatment by paroxetine of delusional disorder, somatic type, accompanied by severe secondary depression. ClinNeuropharmacol 33: 48-49.
- Hayashi H, Oshino S, Ishikawa J, Kawakatsu S, Otani K (2004) Paroxetine treatment of delusional disorder, somatic type. Hum Psychopharmacol 19: 351-352.
- Lee AC, Rudebeck SR (2010) Investigating the interaction between spatial perception and working memory in the human medial temporal lobe. J CognNeurosci 22: 2823-2835.
- Barense MD, Henson RN, Lee AC, Graham KS (2010) Medial temporal lobe activity during complex discrimination of faces, objects, and scenes: Effects of viewpoint. Hippocampus 20: 389-401.
- Stein TD, Alvarez VE, McKee AC (2014) Chronic traumatic encephalopathy: a spectrum of neuropathological changes following repetitive brain trauma in athletes and military personnel. Alzheimers Res Ther 6: 4.
- Squire LR, Stark CE, Clark RE (2004) The medial temporal lobe. Annu Rev Neurosci 27: 279-306.
- Chamelian L, Feinstein A (2006) The effect of major depression on subjective and objective cognitive deficits in mild to moderate traumatic brain injury. J Neuropsychiatry ClinNeurosci 18: 33-38.

