Mohammad Alanazy1* and Anas Mohammad Albarrak2*
1Department of Internal Medicine, Neurology division, Kink Khalid University Hospital, Saudi Arabia
2Prince Satam Bin AbdulazizUniverstiy, Alkharj, Saudi Arabia
- *Corresponding Authors:
- Mohammad Alanazy
Department of Internal Medicine, Neurology division. Kink Khalid University Hospital, Saudi Arabia
Tel: 0096611-4699414
E-mail: dranazy@gmail.com
Anas Mohammad Albarrak
Prince Satam Bin Abdulaziz Universtiy, Alkharj, Saudi Arabia.
Tel: 00966553184884
E-mail: Dr.albarrak@gmail.com
Received date: January 14, 2016; Accepted date: January 25, 2016; Published date: January 29, 2016
A 60-year-old right-handed woman presented with acute disorientation. Neurological examination showed impaired short-term memory, disorientation to time and place, and flattened right nasolabial fold. Brain MRI showed acute ischemic stroke in the territory of anterior choroidal artery (AChA) involving left mesial temporal, globuspallidus, posterior limb of internal capsule and lateral thalamus. The classic clinical findings in AchA stroke include contralateral hemiparesis, hemianaesthesia and hemianopia. Disorientaiton occurs only in 2.7% of AChA stroke [1]. Recognition of such an uncommon presentation of AChA stroke is important to avoid missing an opportunity for thrombolysis in soma for sale the appropriate clinical setting.
Background
Anterior choroidal artery (AChA) usually originates from the internal carotid artery and supplies critical brain areas important for vision and motor control. These include the optic tract, lateral geniculate nucleus and lateral aspect of thalamus, posterior limb of the internal capsule, lateral aspect of the midbrain, and the choroid plexus [1]. The AChA syndrome is a rare disease that presents with hemiplegia, hemianaesthesia and hemianopsia as a result of cerebral infarction in the anterior choroidal artery territory [2]. The syndrome may also be associated with neuropsychological disorders, including left neglect syndrome in right-sided lesions and disorders of speech in left-sided lesions [2-4]. However, a considerable variability in the case presentation have been reported mainly due to the incorrect diagnosis of earlier reports using computed tomography (CT) and the fact that the posterior limb of the internal capsule (PLIC) can be sometimes supplied by perforators arising from the middle cerebral artery 4. The majority of the anterior choroidal artery infarctions are due to occlusion of AchA or its branches without any evidence of carotid disease or cardiogenic embolism [3,4].
Case Report
A 60-year-old right-handed woman presented with acute disorientation. Neurological examination showed impaired short-term memory, disorientation to time and place, and flattened right nasolabial fold. Brain MRI showed acute ischemic stroke (Figure 1) in the territory of AChA involving left mesial temporal, globuspallidus, posterior limb of internal capsule and lateral thalamus (Figure 1).
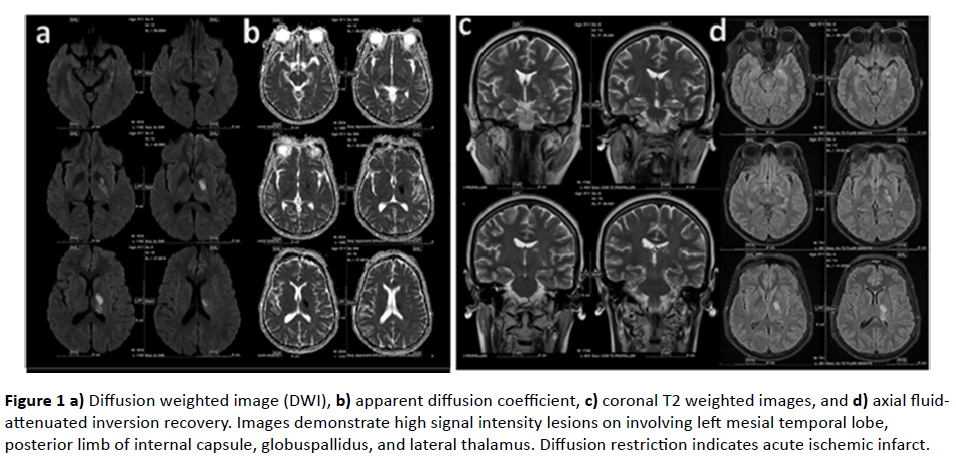
Figure 1 a) Diffusion weighted image (DWI), b) apparent diffusion coefficient, c) coronal T2 weighted images, and d) axial fluidattenuated inversion recovery. Images demonstrate high signal intensity lesions on involving left mesial temporal lobe, posterior limb of internal capsule, globuspallidus, and lateral thalamus. Diffusion restriction indicates acute ischemic infarct.
Discussion
We are reporting disorientation as a rare presentation of the AChA syndrome. Classically, AChA syndrome presents with hemiplegia, hemianaesthesia and hemianopsia [2]. For example, a review of 112 patients diagnosed with AchA infarction in Spain showed that the most common presentation were contralateral hemiparesis (77.6%), sensory dysfunction (75.8%), aphasia in the dominant hemisphere (17%), contralateral hemianopia (14.2%), and ataxia (12.5%) [3]. Another review of 124 patients diagnosed with AchA infarction over a 10 year in a medical center in South Korea showed that the frequent neurologic manifestations were dysarthria (85%), hemiparesis (81%), facial palsy (73%), ataxia (31%), sensory deficit (28%), and visual field defect (14%) [4]. On the other hand, disorientation and distributed consciousness were only seen in 2.7% and 4.7% (respectively) of the patients diagnosed with AchA infarction [3,4]. The variability of the presentation may be directed by the different mechanisms of infraction (small or large artery), the extent of the lesion, and the presence of collateral circulation [3,4]. Recognition of such an uncommon presentation of AChA stroke is important to avoid missing an opportunity for early thrombolytic therapy which was found to be a critical determinant factor for stroke evolution [5]. This report highlights the importance of typical MRI findings in the diagnosis a unilateral AChA stroke.
Disclosures
The authors report no disclosures relevant to this manuscript.
Authors Contribution
Both authors contributed equally to data collection, writing and reviewing the manuscript.
8351
References
- Wiesmann M, Yousry I, Seelos KC, Yousry TA (2001) Identification and anatomic description of the anterior choroidal artery by use of 3D-TOF source and 3D-CISS MR imaging. AJNR Am J Neuroradiol 22: 305-310.
- Decroix JP, Cambier J, Masson M (1985) The anterior choroidal artery syndrome. Presse Med 14: 1085-1087.
- Ois A, Cuadrado-Godia E, Solano A, Perich-Alsina X, Roquer J (2009) Acute ischemic stroke in anterior choroidal artery territory. J Neurol Sci 281: 80-84.
- Sohn H, Kang DW, Kwon SU, Kim JS (2013) Anterior choroidal artery territory infarction: lesions confined to versus beyond the internal capsule. Cerebrovasc Dis 35: 228-234.
- Wu MC, Tsai LK, Wu CC (2014) Thrombolytic therapy is an only determinant factor for stroke evolution in large anterior choroidal artery infarcts. J Stroke Cerebrovasc Dis 23: 1089-1093.

