Keywords
Dextrocardia, Situs inversus totalis, Mitral stenosis, Cardiopulmonary bypass (CPB)
Introduction
Dextrocardia is a rare congenital cardiac anomaly with the heart in the right side of the chest which can often be associated with other complex congenital heart diseases such as a single ventricle, double outlet or double inlet ventricles and tricuspid atresia [1,2].
Dextrocardia is defined as abnormal condition in which the main cardiac axis points to the right and not because of pulling or pushing of heart [3] which may be associated with situs solitus, situs inversus, or situs ambiguous. The prevalence rate of dextrocardia ranged from 0.37-0.53% per 10,000 live birth in different studies [4,5]. Dextrocardia with situs inversus totalis means, heart and all other body organs are the mirror image of one another [6]. The incidence of dextrocardia with situs inversus totalis is 1/10,000 to 50,000 births [7]. Dextrocardia in adults are usually diagnosed incidentally during routine examination or radiographic examination for some purposes. Dextrocardia is also confused with dextroposition in which the heart is displaced towards the right hemithorax due to some abnormalities such as diaphragmatic hernia, right pneumonectomy, or right pulmonary hypoplasia etc [8].
It is very important to diagnose situs inversus totalis in patients with acquired valvular diseases to prevent errors during the procedure. It is really a challenging position during such a procedure where surgeons need to modify their approach with poor exposure of cannulation sites and diseased valves. Here we report the first case of double valve replacement in patient with dextrocardia and situs inversus totalis in our institute.
Case Report
A 51-years- old man was admitted in our department with symptoms of exertional and non exertional dyspnea, palpitation, light headedness, orthopnea, giddiness and lethargy. He has been experiencing these symptoms since last ten years whereby diagnosed dextrocardia in a local hospital but became severe recently in last 2 years. He had been followed up for the above mentioned symptoms due to moderate mitral stenosis (MS) and moderate severe aortic stenosis (AS) and aortic regurgitation (AR) since last ten years in the local hospital. He was non-hypertensive, non-diabetic and had no surgical history. He was in Class III cardiac functional capacity of New York Heart Association (NYHA). On his physical examination, grade 4/6 pansystolic murmur was heard all over the precordium, breath sounds were diminished. ECG showed atrial fibrillation (AF) with ventricular rate of 86/min. Chest X-ray showed dextrocardia (Figure 1A and 1B).
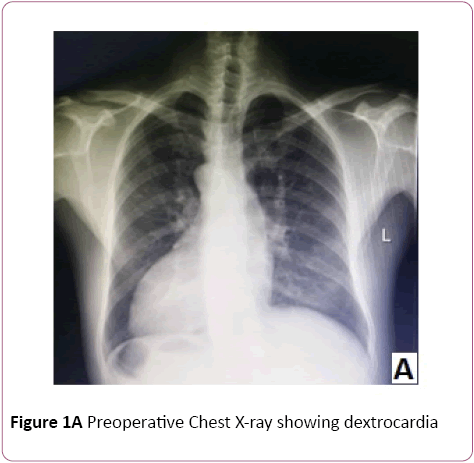
Figure 1A: Preoperative Chest X-ray showing dextrocardia
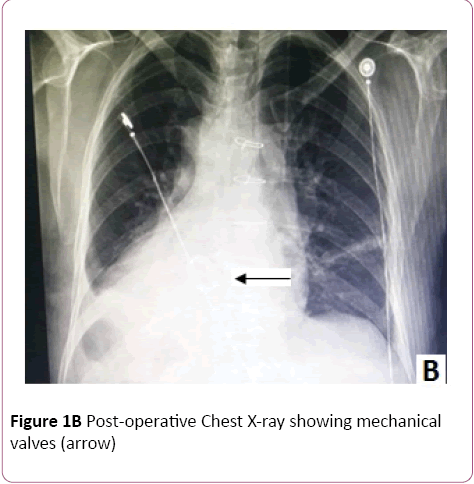
Figure 1B: Post-operative Chest X-ray showing mechanical valves (arrow)
Transthoracic echocardiography revealed dextrocardia, moderate mitral stenosis, moderately severe combined aortic stenosis and aortic regurgitation, mild to moderate tricuspid regurgitation, atrial fibrillation, decompensated heart with weak left ventricular anterior wall motion. He had a left ventricular end-systolic diameter of 47.51 mm and an enddiastolic diameter of 60.53 mm and ejection fraction of 43%. He had a left atrial anteroposterior diameter of 46 mm, right atrial size of 39 mm 51 mm (Figure 2).
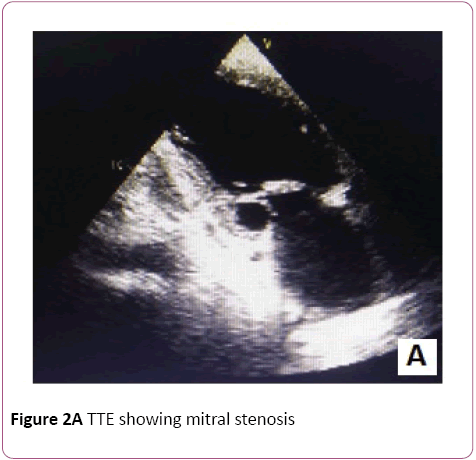
Figure 2A: TTE showing mitral stenosis
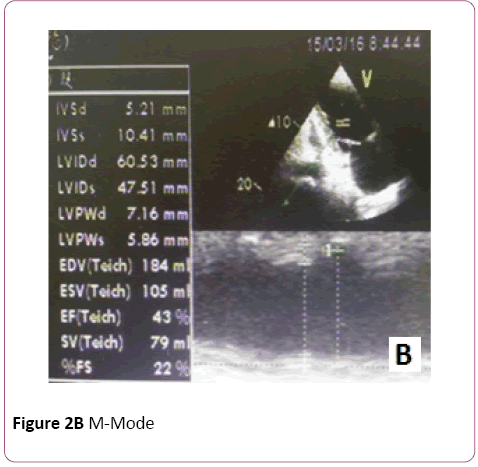
Figure 2B: M-Mode
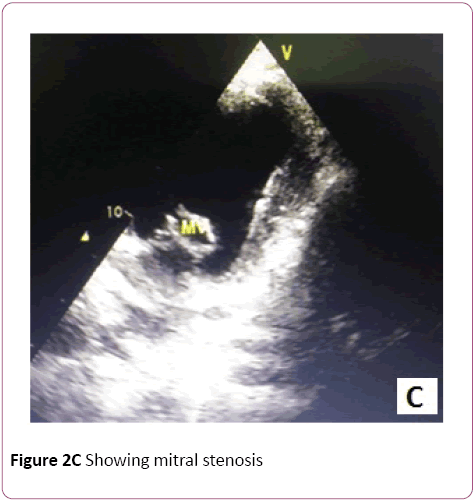
Figure 2C: Showing mitral stenosis

Figure 2D: Aortic regurgitation
Preoperative CTA was performed and it was found that coronary arteries were normal as shown in the following Figures (Figure 3).
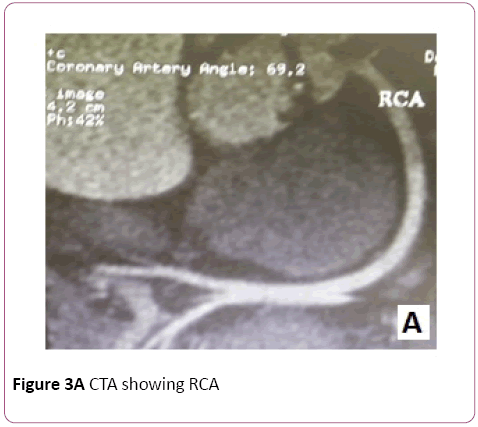
Figure 3A: CTA showing RCA

Figure 3B: CTA showing LAD
A preoperative thoraco-abdominal contrast enhanced CT was performed to find out any abdominal abnormalities and to confirm the type of dextrocardia. It was confirmed that patient was having dextrocardia with situs inversus totalis (Figure 4).
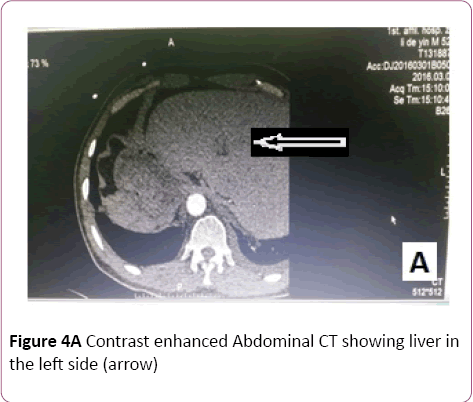
Figure 4A: Contrast enhanced Abdominal CT showing liver in the left side (arrow)
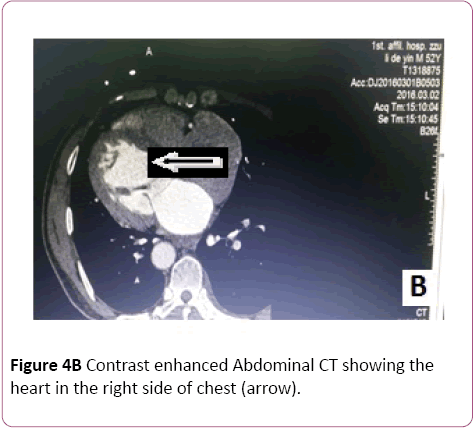
Figure 4B: Contrast enhanced Abdominal CT showing the heart in the right side of chest (arrow).
Moderate hypothermia was applied. We also used ice water for intraoperative myocardial tissue protection. Cardioplegic arrest was achieved by direct antegrade blood cardioplegia infusion into the coronary ostia after aortotomy since this patient had Aortic regurgitation. The left vent was placed in the left superior pulmonary vein.
Surgical technique
After sufficient anesthesia, Operator was standing on the left with the assistants in the right side. Following a median sternotomy and pericardiotomy, superior and inferior vena cava was widely separated from the pericardium for cannulation and decannulation without lifting the heart. Arterial cannulation was performed on ascending aorta and venous cannulation was done through bicaval cannulation of the superior and inferior vena cava (Figure 5).
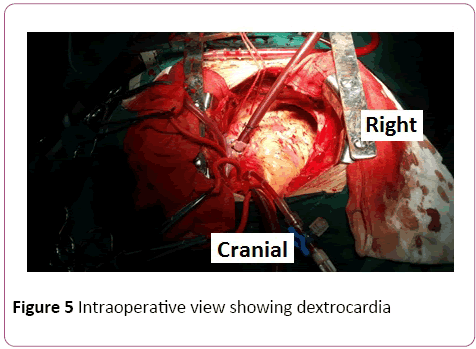
Figure 5: Intraoperative view showing dextrocardia
The incision on the right atrium was done from the surface of right auricle to the front side of the right atrium and parallel to the atrio-ventricular groove extending upto the ceiling of the left atrium. Following the right atriotomy, a septal incision was performed in the center of the fossa ovalis and extended to the inferior fossa ovalis to join with the right atrial atrium. The mitral valve was exposed by placing retractor to the walls of the left atrium. Intraoperative finding revealed that the commissures were fused with each other and repair of the mitral valve was not feasible. Anterior leaflet was incised while posterior leaflet was secured. Mechanical mitral valve replacement was done using sorin 27 mm with 2-0 prolene continuous suture. Aortic valve was calcified with fusion of the commissures. Leaflets were incised leaving about 2 mm in the annulus. Incised leaflets of both valves were also sent for histopathological examination as shown in Figure 6. Histopathological examination confirmed the hyaline degeneration of the valves due to rheumatic heart disease. A mechanical aortic valve, sorin 21 mm was replaced by interrupted suturing. Atrial septum was closed using 3-0 prolene suture. Ascending aorta was closed using 4-0 prolene suture. A de-vega procedure was performed for the tricuspid regurgitation. After de-airing, aortic clamp was removed and heart started beating spontaneously. After proper observation, CPB weaned off and closed the chest. Patient was taken to the ICU. The patient had an uneventful recovery after the surgery and discharged on the postoperative tenth day (Figure 6).
Figure 6A: Histopathological examination mitral valve
Figure 6B: Aortic valve showing hyaline degeneration
Discussion
Human heart develops from a primitive cardiac tube, forming the morphologically distinct left and right ventricles. The primitive heart tube may loop either to the left (levo or L) or to the right (dextro or D). In D-loop, morphologic right ventricle is in the right of morphologic left ventricle while in Lloop morphologic right ventricle is in the left of morphologic left ventricle, The D-loop is the normal (solitus) cardiac loop and L-loop is a mirror-image (inversus) loop [9].
Dextrocardia usually coexist with various other congenital heart disorders and situs anomalies [10] such as situs solitus, situs inversus and isomerism in which situs solitus is the most common form [11]. In situs solitus, whole viscera are in normal position. In situs inversus, viscera which are normally present on the right side are situated on the left, while viscera which are normally on the left are situated on the right. In such patients, inferior vena cava may be interrupted within the liver. And can lead to difficulties during inferior vena cava cannulation for CPB establishment. Situs inversus totalis is a very rare condition. Dextrocardia with situs inversus usually have structurally normal heart.
Patients with dextrocardia are believed to have a normal life span. The incidence of CAD in population with dextrocardia is similar to that of the general population [12]. The first case of rheumatic MS in a dextrocardia patient with situs inversus was described by Owen [13]. The anatomy of the patient is almost always challenging in case with dextrocardia. It is very important decision for the surgeon where to stand during surgery. Saad et al. [14] addressed regarding the position of surgeon performing surgery on a patient with dextrocardia.
Our patient had a typical case of dextrocardia with total situs inversus. All the visceral organs were mirror images of one another. Various approaches have been described in patient with dextrocardia for mitral valve replacement but still double valve replacement is rare. St Rammos et al. [15] established CPB by cannulating the aorta and the left common femoral vein. In our case, we established CPB through usual manner of cannulating aorta, superior vena cava and inferior vena cava without any heart positioner. Yokoyama et al reported a case of mitral valve replacement via a transseptal approach in conjunction with aortic root replacement in a patient with dextrocardia and situs inversus in which they stood on the left side of the patient [16]. Moreover, ?ahin et al. [17] reported on a case of mitral valve replacement surgery via the transseptal approach in a patient with dextrocardia and situs inversus, but they did not mention where the surgeon stood.
Our patient had an uneventful recovery after the surgery. The ICU stay time was 12 hours and total hospital stay time was 12 days including 2 days before surgery.
Conclusion
Proper understanding of the anatomy with coexisting anomalies is the key to success in performing surgeries in such a rare and challenging case of dextrocardia with situs inversus totalis. We suggest to stand the surgeon in the left side of the patient and to separate superior and inferior vena cava widely from the pericardium for better exposure in cannulation and decannulation without lifting the heart which can prevent the danger of left ventricular rupture.
9803
References
- Hutha JC, Hagler DJ, Seward JB, Tajik AJ, Julsurd PR, et al. (1982) Two dimensional echocardiographic assessment of dextrocardia: a segment approach. Am J Cardiol 50: 1351-1360.
- Bohun CM, Potts JE, Casey BM, Sandor GG (2007) A populationbasedstudy of cardiac malformations and outcomes associated with dextrocardia. Am J Cardiol 100:305-309.
- Arcilla RA, Gasul BM (1961) Congenital dextrocardia, Clinical, angiocardiographic, and autopsy studies on 50 patients. J Pediatr 58:39-58.
- (1980) Report of the New England Regional Infant Cardiac Program. Pediatrics 65:375-461.
- Ferencz C, Correa-Villasenor A, Loffredo CA, Wilson PD(1997) Genetic and environmental risk factors for majorcardiovascular malformations: The Baltimore-Washington Infant Study, 1981-1989. NewYork: Futura.
- Oliveira N, Oliveira F, Dias E, Borges L, Cássio I (2015)LericheSyndrome in a Patient with SitusInversusTotalis. Ann VascSurg 29:5-8.
- Garg N, Agarwal BL, Modi N, Radhakrishnan S, Sinha N (2003) Dextrocardia: an analysis of cardiac structures in 125 patients. Int J Cardiol 88:143-55.
- Bharati S, Lev M (1979) Positional variations of the heart and its component chambers.Circulation 59:886-887.
- Van Praagh R, Van Praagh S, Vlad P, Keith JD (1964) Anatomic types of congenital dextrocardia:diagnostic and embryological implications. Am J Cardiol 13:510–531.
- Cobiella J, Muñoz C, Arís A (2005) Complex cardiac surgery in apatient with dextrocardia and polysplenia. Rev Esp Cardiol 58:1236-1238.
- Lev M, Liberthson RR, Eckner FA, Arcilla RA (1968) Pathologicanatomy of dextrocardia and its clinical implications.Circulation 37:979-999.
- Khalil S, Kamal A, Ahmed S (2005) Acute myocardial infarction in a patient with dextrocardia and situsinversus. J Electrocardiol 38:412-413.
- Owen SA (2003) A case of complete transposition of viscera, associated with mitral stenosis; including a description of the electrocardiographic tracings. Heart 113:1911-1912.
- Saad RA,Badr A, Goodwin AT, Dunning J (2009) Should you standon the left or the right of a patient with dextrocardia who needs coronary surgery? Interact Cardiovasc Thorac Surg 9: 698-702.
- St Rammos K, Bakas AJ, Panagopoulos FG (1996) Mitral valve replacement in a Jehovah's Witness with dextrocardia and situssolitus. J Heart Valve Dis 5:673-674.
- Yokoyama Y, Satoh H, Abe M, Nagashima M, Kurata A, et al. (2011) Cardiac surgery for annuloaorticectasia and mitral regurgitation in an adult patient with dextrocardia. Gen Thorac Cardiovasc Surg 59:341-343.
- Sahin MA, Guler A, Kaya E (2011) Mitral valve replacement in a patient with situsinversus and dextrocardia. Thorac Cardiovasc Surg 59:305-306.


