Kapil Dev1, Venkateshaiah R Pallav i2 and Uttam D Bafn a2
1Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, Bangalore, India
2Department of Gynecologic Oncology, Kidwai Memorial Institute of Oncology, Bangalore, India
Corresponding Author:
Kapil Dev
Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, Bangalore, India
Tel: 918197010684
E-mail: dr.kapil2010@gmail.com
Received date: September 06, 2016; Accepted date: September 17, 2016; Published date: September 21, 2016
Citation: Dev K, Pallavi VR, Bafna UD. “Drop Recurrence” External Genitalia Recurrence in Carcinoma Cervix after Previous Surgery. Arch Can Res. 2016, 4:3.
Cervical cancer is the most common cancer in women in India and diagnosed new cases around 1,32,000 and 74,000 deaths annually. Although, a progress in the management of cervical cancer has been accomplished over the past 5-6 decades, including introduction of PAP smear into screening as well as surveillance and addition of systemic platinum based chemotherapy to radiation therapy with proved definite benefits, the rate of recurrence in optimally treated cervical cancer is still significant. Up to 10% to 25% women with cervical cancer stage IB-IIA without lymph node involvement experience a recurrence, which is higher among patients with advance stages with lymph node involvement and locally advanced disease, and ranges up to 70%. The majority of the recurrences in cervical cancer are pelvic failure in comparison to distant recurrence, irrespective of the stage at diagnosis and prior treatment taken.
Commentary
Cervical cancer is the most common cancer in women in India and diagnosed new cases around 1,32,000 and 74,000 deaths annually [1]. Although, a progress in the management of cervical cancer has been accomplished over the past 5-6 decades, including introduction of PAP smear into screening as well as surveillance and addition of systemic platinum based chemotherapy to radiation therapy with proved definite benefits, the rate of recurrence in optimally treated cervical cancer is still significant. Up to 10% to 25% women with cervical cancer stage IB-IIA without lymph node involvement experience a recurrence, which is higher among patients with advance stages with lymph node involvement and locally advanced disease, and ranges up to 70% [2-5]. The majority of the recurrences in cervical cancer are pelvic failure in comparison to distant recurrence, irrespective of the stage at diagnosis and prior treatment taken [6,7]. “Drop metastasis” has been earlier described as endometrioid adenocarcinoma of cervix in a patient with endometrioid adenocarcinoma of endometrium. It is not yet validated in squamous cell carcinoma of cervix as squamous cell carcinoma of vulva and/or vulvo-vaginal junction. Thus, we are presenting here this phenomenon as well as “Drop recurrence”, describing squamous cell carcinoma of vulva and/or vulvo-vaginal mucocutaneous junction in a patient with a history of cervical squamous cell carcinoma.
A 41-year woman presented with vaginal ulcer and mucous discharge per vaginam for a period of 4 weeks. Earlier she had been diagnosed carcinoma cervix stage IIB, for which she underwent concurrent chemo radiotherapy followed by radical hysterectomy type I, two years back. After that, she was on regular surveillance as per our institutional protocol. Examination of the patient revealed an ulcero-proliferative lesion over inner surface of left labia majora, of size approximate 1.5 × 1 cm (Figure 1). The rest of the pelvic examination was within normal limits. Histopathological examination of biopsy showed non-keratinizing squamous cell carcinoma (Figure 2). CECT abdomen pelvis and thorax suggested no evidence of disease elsewhere. She underwent wide local excision, and histopathology report made a remark of recurrent lesion with tumor free margins in all directions.
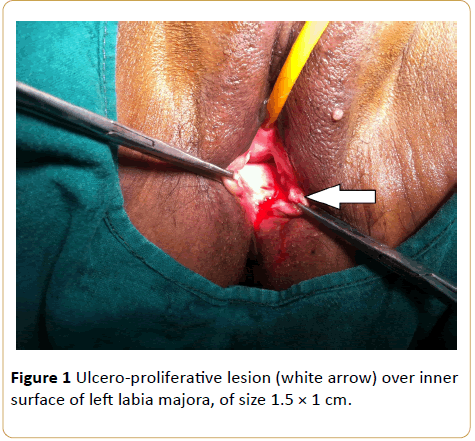
Figure 1: Ulcero-proliferative lesion (white arrow) over inner surface of left labia majora, of size 1.5 × 1 cm.
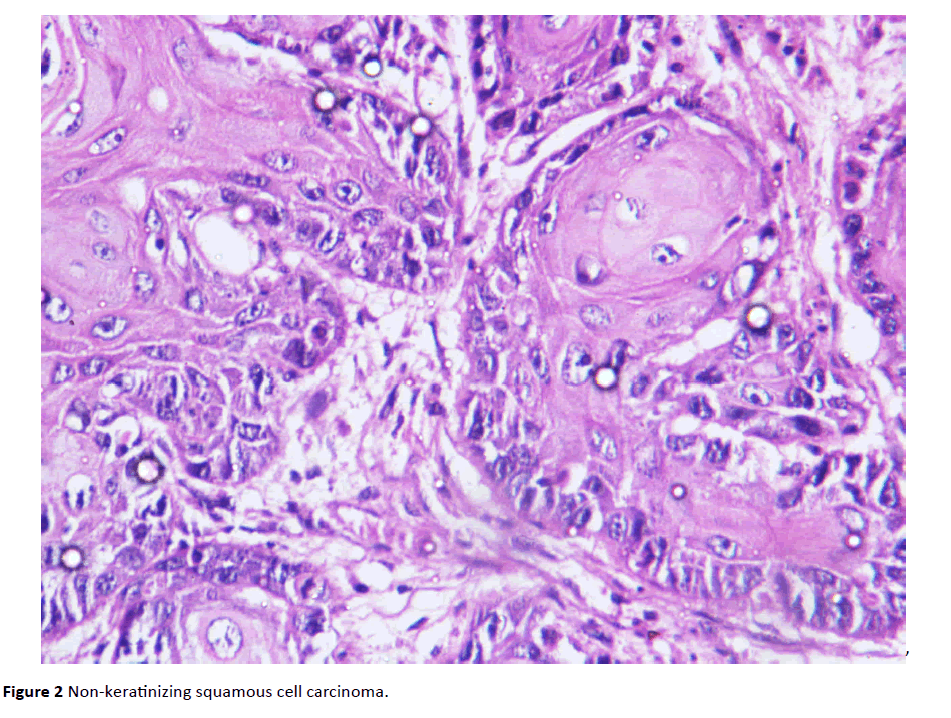
Figure 2: Non-keratinizing squamous cell carcinoma.
The reported rate of recurrence in carcinoma cervix stage IIB-III is in the range of 23% to 42%. [6] Vaginal stump is the most common site of recurrence among pelvic failure cases following surgical treatment of cervical cancer, ranging from 56% to 80%, followed by the pelvic lymph node and pelvic side walls [8]. Isolated vulval recurrence is reported rarely after multimodality treatment for cervical cancer. This case presents an isolated recurrence at vulva after a period of two years from primary treatment. A variety of symptoms including pelvic pain, anorexia, vaginal bleeding, discharge, cachexia and psychological problems may be the presentation in recurrent cervical cancer. Most of the recurrence occurs within two years of completion of treatment. The mechanism of these recurrences is might be the dislodgement and landing of tumor cells over the mucosal surface of the vulva and hens developing a lesion after a latent period during surveillance. Several factors affecting treatment are patient’s performance status, site of recurrence, size of recurrence and prior treatment received. The overall survival in these patients with pelvic recurrence is variable and has been reported in literature with a wide range of 6% to 77% [8,9]. Patients with central recurrence of size less than 3 cm, 10 -year survival was observed up to 48%, and that with non-palpable recurrence was up to 78%. [10] In view of favorable and isolated small recurrence with good performance status, present case had undergone wide local excision.
We are putting this presentation particularly to define a new term “Drop recurrence” in cervical cancer following surgery.
13747
References
- WHO/ICO (2007-2008) Information centre on HPV and cervical cancer (HPV Information Centre). Summary report on HPV and cervical cancer statistics in India.
- Delgado G, Bundy B, Zaino R (1990) Prospective surgical-pathological study of disease-free interval in patients with stage IB squamous cell carcinoma of the cervix: A Gynecologic Oncology Group study. Gynecol Oncol 38: 352-357.
- Zaino RJ, Ward S, Delgado E (1992) Histopathologic predictors of the behaviour of surgically treated stage IB squamous cell carcinoma of the cervix. A Gynecologic Oncology Group study. Cancer 69: 1750-1758.
- Burghardt E, Baltzer J, Tulusan AH (1992) Results of surgical treatment of 1028 cervical cancers studied with volumetry. Cancer 70: 648-655.
- Stehman FB, Bundy BN, DiSaia PJ (1991) Carcinoma of the cervix treated with radiation therapy. I. A multi-variate analysis of prognostic variables in the Gynecologic Oncology Group. Cancer 67: 2776-2785.
- Perez CA, Grigsby PW, Camel HM (1995) Irradiation alone or combined with surgery in stage IB, IIA, and IIB carcinoma of the uterine cervix: update of a nonrandomized comparison. Int J Radiat Oncol Biol Phys 31: 703-716.
- Fagundes H, Perez CA, Grigsby PW (1992) Distant metastases after irradiation alone in carcinoma of the uterine cervix. Int J Radiat Oncol Biol Phys 24: 197-204.
- Webb MJ, Symmonds RE (1980) Site of recurrence of cervical cancer after radical hysterectomy. Am J Obstet Gynecol 138: 813-817.
- Jobsen JJ, Lee JW, Cleton FJ (1989) Treatment of locoregional recurrence of carcinoma of the cervix by radiotherapy after primary surgery. Gynecol Oncol 33: 368-371.
- Ito H, Shigematsu N, Kawada T (1997) Radiotherapy for centrally recurrent cervical cancer of the vaginal stump following hysterectomy. Gynecol Oncol 67: 154-161.

