Maria Ayub*, Saira Amir, Kainat Firdous, Sumiya Khan and Ishrat Iqbal
Jinnah University for Women, Pakistan
*Corresponding Author:
Maria Ayub
Lecturer, Faculty of Pharmacy, Jinnah University for Women
Karachi 74600, Pakistan
Tel: +923313119160
E-mail: maria.ayub2000@gmail.com
Received date: May 13, 2016; Accepted date: June 16, 2016; Published date: June 26, 2016
Citation: Ayub M, Amir JS, Firdous K, et al. E. coli the Most Prevalent Causative Agent Urinary Tract Infection in Pregnancy: Comparative Analysis of Susceptibility and Resistance Pattern of Antimicrobials. Arch Clin Microbiol. 2016, 7:4. doi:10.4172/1989-8436.100054
Copyright: © 2016 Ayub M et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Urinary Tract Infections (UTIs) are the most common infections reported in pregnant women, however the causes of UTI in pregnant women is the change in physiological and anatomical patterns, leading to serious consequences to fetal development and maternal health. The percentages of development of UTI associated morbidity in females are about 40 to 50%, while 5% chances are present in males. However, these chances are deliberately increased in pregnancy. The species responsible for gestational UTIs are the same as that of nonpregnant UTIs out of which about 80 to 90% of UTIs are caused by Escherichia coli (E.coli). For the estimation of the most prevalent UTI pathogen in pregnant female a random data has been utilized by the laboratory reports of gestational UTIs. The results have found E.coli as the most prevalent pathogen involved in gestational UTIs and other prevalent agents include Enterococcus species, Klebsiella species, Group B Streptococcus species, Group B Staphylococcus species and other less prevalent species include Citrobacter 8%, Acinetobacter and Pseudomonas species. The resistance pattern of several antibiotics against E.coli are as follow: Norfloxicin 67%, Olfloxicn, Amox-clav, Ceftriaxone and Cefuroxime 43%, Ciprofloxacin 33%, Cefepime 29%, Piperacillin and Tazobactam, Amikacin, Nitrofurantoin and Fosfomycin 14%, whereas Meropenem is found to be 0% resistant (100% sensitive). Resistance patterns of antibiotics against the second most prevalent organism (Enterococcus species) are: Amikacin 100%, Norfloxicin and Gentamycin; Ofloxicin and ciprofloxacin 83%; Meropenem, Cefepime and Fosfomycin 40%; Cefuroxime 33%, Ceftriaxone and Nitrofurantoin 17%, Amox-Clav and Vancomycin 0% (100% sensitivity). Whereas, the third most commonly found resistant organism follows the pattern: Nitrofurantoin 75% resistant, Amox-Clav 50%; Ofloxicin, Ciprofloxacin, Amikacin, Cefuroxime, Norfloxicin, Fosfomycin are resistant about 25%. Whereas, Cefepime, Meropenem, Ceftriaxone are 0% resistant. The results have clearly shown E.coli as the most prevalent microorganism in gestational UTIs.
Keywords
UTI; Pyelonephritis; Morbidity; Mortalities; Gestational UTI
Introduction
Urinary Tract Infections (UTI) are one of the most common bacterial infections of the human beings. Women are however more prone to be affected by UTI compared to men, [1] Urinary tract infections along with its associated problems leading to complications which are the causative agent of nearly 150 million mortalities yearly, worldwide. The morbidity may be developed in 40% - 50% of females and 5% of males [2] The probability of UTI has been observed to be elevated during pregnancy [1] Pregnant women are at an increased chance of bacterial ascension to the renal system and may cause pyelonephritis commonly known as kidney infection [3] relatively due to dilation of the renal pelvis and ureters by the eighth week of gestation [4]. Along with the humoral and immunological changes during normal gestation [5]. Bacteriuria that leads to the pyelonephritis during pregnancy is associated with imperfect consequences for both the maternal and neonatal health, including maternal sepsis and anemia, Preterm Birth (PTB) Low Birth Weight (LBW), and perinatal mortality [6]. The species causing UTIs during gestation are the same as those found in non-conceiving patients. Escherichia coli are responsible for about 80 to 90 percent of infections. Other gram-negative rods including Proteus mirabilis and Klebsiella pneumoniae are also commonly found. Gram-positive organisms such as group B Streptococcus and Staphylococcus saprophyticus are less commonly found in cases of UTI. Group B Streptococcus has salient consequences for the management of gestation. Less commonly found organisms that may cause UTI include enterococci, Gardnerella vaginalis and Ureaplasma ureolyticum [7-9]. The mechanism of UTI in pregnant patients has been demonstrated by obstruction of urine outflow by the conceiving uterus [10]. This relatively simple supposition does not regard the receptor etiology of the ascending UTI or gestational alteration of the immunity. Gestational pyelonephritis is related to multiple complexities, as listed above. We have formerly investigated that gestational pyelonephritis is usually caused by E.coli having adhesions of the Dr Family (E.coli), an antibiotic resistant microorganism accomplished by invading renal interstitial tissue, discharging leukocytes and persisting in epithelial cells. Epidemiological studies of UTIs evaluate that the prevalence of Asymptomatic Bacteriuria (ABU) is 4-10%, cystitis 1-4%, and pyelonephritis 1-2%, with the rate similarity in expecting and non-expecting women [11].
Methodology
The designed study is based on a type of prospective data which has been collected by mean of taking a prefatory analysis of laboratory data, collected randomly from a mean population of 50 pregnant UTI patients and the pattern of resistance of different antibiotics has been discussed. Concerning the most prevalent pathogens in pregnant women UTIs focusing mainly on E.coli. The total discrete time period taken for the whole data collection was probably 2 to 3 weeks.
Result
From the whole analyzed data, it has been concluded that the most prevalent organism in pregnant women UTI is Escherichia coliE.coli). The other prevalent organisms include: Enterococcus species and Klebseilla species respectively. Out of which E.coli accounts for 28% cases of UTIs in pregnancy, Enterococcus species and Klebseilla species account for 24% and 12% cases during pregnancy.
Table 1 Elucidates different UTI organisms along with their relative classes, invading percentages and their complications. However the result has estimated that Escherichia coli 28%, Enterococcus species, 24%, Klebsiella species and Group B Streptococcus species, 12% Group B Staphylococcus species and Citrobacter species, 8% Acinetobacter species and Pseudomonas species 4% are found to be effective UTI organisms with their respective percentages to invade.
| Major Class |
Pathogens |
Percentage |
Complications |
| Gram -ve |
Escheria coli |
28% |
Pyelonephritis, preterm birth, low birth weight, and increased perinatal mortality, Eclampsia. |
| Gram +ve |
Enterococcus species |
24% |
| Gram -ve |
Klebsiellaspecies |
12% |
| Gram +ve |
Group B Streptococcus species |
12% |
| Gram +ve |
Group B Staphylococcus species |
8% |
| Gram -ve |
Citrobacter species |
8% |
| Oxidase -ve |
Acinobacterspecies |
4% |
| Gram -ve |
Pseudomonas species |
4% |
Table 1: Percentage frequencies of micro-organism implicated in UTI during pregnancy along with their complications.
Figure 1 Illustrate the percentage resistance of gram negative pathogen E.coli to different antibiotics used to treat UTI. The figures have clearly shown that E.coli was found to be resistant from agents: Piperacillin and Tazobactam, Amikacin, Fosfomycin, Nitrofurantoin for about 14% and 43% from Olfloxicn, Amox-clav, Ceftriaxone and Cefuroxime while 33% from Ciprofloxacin, 29% with Cefepime, 67% Norfloxicin, Piperacillin and Tazobactam, Amikacin, Nitrofurantoin and Fosfomycin 14% and dramatically its 0% resistant with Meropenem.
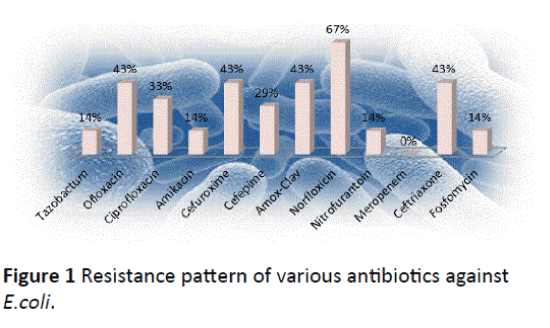
Figure 1: Resistance pattern of various antibiotics against E.coli.
Figure 2 Statical evaluation has estimated percentage resistance of different antibiotics used in UTI treatment against the second most prevalent pathogen Enterococcus Species. It has been evaluated from the data that Amikacin, Norfloxicin, Gentamicin show resistivity about 100%, Ciprofloxacin and Ofloxicin 83%, Cefepime, Fosfomycin and Meropenem 40%, while the percentage resistance of Cefuroxime is 33%, 17% of Ceftriaxone and Nitrofurantoin. Meanwhile it is 0% resistant with Piperacillin and Tazobactam, Amox-Clav and Vancomycin which means 100% sensitive.
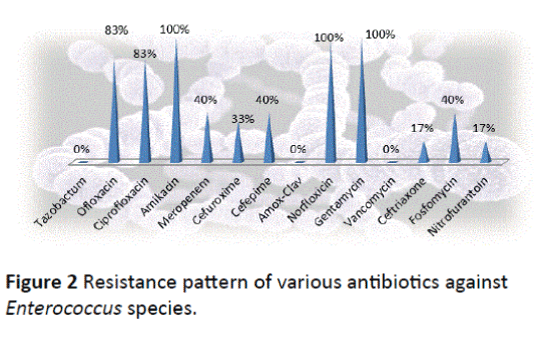
Figure 2: Resistance pattern of various antibiotics against Enterococcus species.
Analyzed data, it has been concluded that the most prevalent organism in pregnant women UTI is Escherichia coli (E.coli). The other prevalent organisms include: Enterococcus species and Klebseilla species respectively. Out of which E.coli accounts for 28% cases of UTIs in pregnancy, Enterococcus species and Klebseilla species account for 24% and 12% cases during pregnancy respectively.
Figure 3 Data showing percentage resistance of antibacterial agents against third most abundantly found pathogen Klebsiella species in gestational UTIs. The found resistance to Nitrofurantoin is 75% and 50% to Amox-clav, 25% with Ofloxicin, Ciprofloxacin, Amikacin, Cefuroxime, Norfloxicin, Fosfomycin while the data has shown 0% resistance against Piperacillin and Tazobactam, Cefepime, Meropenem, Ceftriaxone.
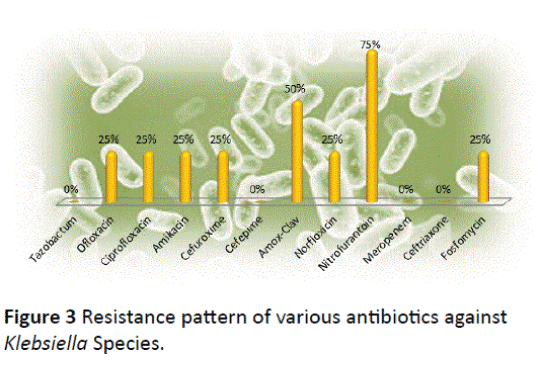
Figure 3 Resistance pattern of various antibiotics against Klebsiella Species.
Discussion
Urinary tract infections are consequence of microbial growth in urinary tract, these infections are the single most common bacterial infections of mankind [12]. Whereas in pregnancy, it involves the lower urinary tract of the bladder [13]. UTI has been reported in 20% cases of pregnant UTIs and the most common cause of admission in obstetrical wards [14]. UTIs have greater chances to develop in pregnancy. UTIs are more consistently managed in pregnancy than in case of other than pregnancy. Urine samples should be sent for culture and sensitivity testing and empiric treatment should be started while awaiting results. Nitrofurantoin, Trimethoprim or Cephalexin is appropriate antibiotic choices (although may be restricted according to pregnancy trimester). Quinolones, e.g. Norfloxicin, should not be used during pregnancy [15]. From the whole analyzed data there is shown the most commonly used antibiotics in gestational UTI treatment, the pathogen culture were collected from the urine analysis of pregnant women. The most prevalent pathogen found to be responsible for UTI is remained E.coli but with percentage of 28%, which is a deviated figure from the other read, past researches which have shown E.coli for about 80 to 90% cause of UTI in pregnant females. As there are many medications used in UTI treatments and most of them have developed resistance to their respective pathogens. However, the highest resistant antibiotic found is Norfloxicin with a percentage resistance of 67% against E.coli pathogen despite of this a past research which has shown Amoxicillin and Ampicillin 20-40% resistant in case of UTI caused by E.coli [16], it has a remarkable and clear indication that resistance emergence is now turned towards drugs other than Penicillins which are no longer considered as empirical therapy for UTI caused by E.coli [16]. Moreover, Fluoroquinolones have been more frequently prescribed for the treatment of such infections, thus increased resistance of Fluoroquinolones has also been reported. Meropenem is found to be the best agent with 100% sensitivity for E.coli in pregnant UTI. Against Enterococcus UTIs, it has been found the Amikacin, Norfloxicin and Gentamicin are the most resistant drugs with a percentage resistance of about 100%, high-level resistance to Gentamicin is primarily due to a bifunctional modifying enzyme AAC(6′)-Ie/APH(2′)-Ia possessing both 6′- acetyltransferase and 2′-phosphotransferase activities and resist all Aminoglycosides except that of streptomycin [17] whereas aph(2′)-Ib is a gene that has been described in E. faecium and its presence resists all amino-glycosides except streptomycin and Amikacin [18]. While the most sensitive agent found to be 100% sensitive to Piperacillin and Tazobactam, Amox-Clav and Vancomycin. However against Klebsiella species it has been found that most resistant agent is Nitrofurantoin with 75% developed resistance. According to several past Nitrofurantoin is said to be a safer agent during pregnancy in UTIs. Case control studies and case series have involved thousands of pregnant women who received Nitrofurantoin but have reported no elevation in major malformations in neonates [19-21]. Whereas one past study found that nitrofurantoin is effective to treat asymptomatic bacteriuria with a cure rate of 86% in a seven day course of therapy in patients with susceptible bacterial strains [22,23]. On the other hand, Piperacillin and Tazobactam, Cefepime, Meropenem, Ceftriaxone are found to be the most sensitive agents with sensitivity 100% in case of UTIs associated with Klebsiella species.
Conclusion
From the whole analyzed data, it has been concluded that the most prevalent organism in pregnant women UTI is Escherichia coli(E.coli). The other prevalent organisms include: Enterococcus species and Klebseilla species respectively. Out of which E.coli accounts for 28% cases of UTIs in pregnancy, Enterococcus species and Klebseilla species account for 24% and 12% cases during pregnancy respectively.
9694
References
- Foxman B (2002) Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am J Med 113: 5S-13S.
- Totsika M, Moriel DG, Idris A, Rogers BA, Wurpel DJ, et al. (2012) Uropathogenic Escherichia coli mediated urinary tract infection.Curr Drug Targets 13: 1386-1399.
- Nicolle LE, Friesen D, Harding GK, Roos LL (1996) Hospitalization for acute pyelonephritis in Manitoba, Canada, during the period from 1989 to 1992, impact of diabetes, pregnancy, and aboriginal origin. Clin Infect Dis 22: 1051-1056.
- Fried AM (1979) Hydronephrosis of pregnancy: ultrasonographic study and classification of asymptomatic women. Am J ObstetGynecol 135: 1066-1070.
- Ramzan M, Bakhsh S, Salam A (2004) Risk factors in urinary tract infection. Gomal J Med Sci 2: 50-53.
- Schnarr J, Smaill F (2008) Asymptomatic bacteriuria and symptomatic urinary tract infections in pregnancy. Eur J Clin Invest 38: 50-57.
- Patterson TF, Andriole VT (1987) Bacteriuria in pregnancy. Infect Dis Clin North Am 1: 807-822.
- Barr JG, Ritchie JW, Henry O, Sheikh ME, Deeb KE (1985) Microaerophilic/anaerobic bacteria as a cause of urinary tract infection in pregnancy. Br J ObstetGynaecol 92: 506-510.
- McDowall DR, Buchanan JD, Fairley KF, Gilbert GL (1981) Anaerobic and other fastidious microorganisms in asymptomatic bacteriuria in pregnant women. J Infect Dis 144: 114-122.
- Gabbe SG, Simpson JL, Niebyl JR (2007) Obstetrics: Normal and Problem Pregnancies. Philadelphia: Churchill Livingstone.
- Nowicki B (2002) Urinary tract infection in pregnant women: old dogmas and current concepts. Curr Infect Dis Rep 4: 529-535.
- Theodor M (2007) Prevalence and antibiogram of urinary tract infections among prison inmates in Nigeria. The Internet Journal of Microbiology 3: 12-23.
- Brook GF, Butel JS, Moses SA (2001) JawetzMelmick and Adelberg’s Medical Microbiology. McGrawHill 22: 637-638.
- Bacak SJ, Callaghan WM, Dietz PM, Crouse C (2005) Pregnancyassociated hospitalizations in the United States, 1999-2000. American Journal of Obstetrics and Gynecology 192: 592-597.
- Clinical Knowledge Summaries (CKS) (2009) Urinary tract infection (lower)-women.
- Widmer M, Gulmezoglu AM, Mignini L, Roganti A (2011) Duration of treatment for asymptomatic bacteriuria during pregnancy. Cochrane Database Syst Rev 12: CD000491.
- Courvalin P, Carlier C, Collatz E (1980) Plasmid-mediated resistance to aminocyclitol antibiotics in group D streptococci. J Bacteriol 143: 541-551.
- Chow J (2000) Aminoglycoside resistance in enterococci. Clin Infect Dis 31: 586-589.
- Briggs GG, Freeman RK, Yaffe SJ (2005) Drugs in pregnancy and lactation. Philadelphia, PA: Lippincott Williams & Wilkins 268-1153.
- Hailey FJ, Fort H, Williams JC, Hammers B (1983) Foetal safety of nitrofurantoinmacrocrystals therapy during pregnancy: a retrospective analysis. J Int Med Res 11: 364-369.
- Czeizel AE, Rockenbauer M, Sorensen HT, Olsen J (2001) Nitrofurantoin and congenital abnormalities.Eur J ObstetGynecolReprodBiol 95: 119-126.
- Macejko AM, Schaeffer AJ (2007) Asymptomatic bacteriuria and symptomatic urinary tract infections during pregnancy. UrolClin North Am 34: 35-42.

