Keywords
Community-directed intervention; Community health workers; Intervention; Implementation; Under-five children; Antimalarial drugs
Introduction
Community-directed Intervention (CDI) is an intervention approach in which communities themselves direct and execute the planning and implementation of a health intervention [1].
CDI first began in 1995 when the African Program for Onchocerciasis Control (APOC) developed and adopted a community-directed approach for the distribution of Ivermectin to residents in remote areas. The success of this approach for the intervention of Onchocerciasis led to the extension of the strategy for the intervention of the other diseases in Africa [1]. A joint funding from the United Nations Development Plan/World Bank/UNICEF/WHO Tropical Disease Research Program sponsored a three-year (2005 to 2008) multi-country study in Nigeria, Uganda and Cameroon to see if the strategy would be effective on four additional intervention: Vitamin A supplementation, distribution of insecticide bed nets, direct observed treatment of Tuberculosis (DOT) and home-management of simple malaria. Based on the successful results registered from the pilot study, it was recommended that the CDI approach be adopted for the other health interventions in areas already practicing CDI of Onchocerciasis [2].
Although CDI was already implemented for the distribution of Ivermectin against Onchocerciasis in the Ndop Health District, it was however not until 2016 that CDI of malaria program was implemented in this health district, with a comprehensive training of Community Health Workers (CHWs) including training on home diagnosis and management of simple malaria and distribution of Insecticide-treated bed nets (ITNs) [3].
Local health services and partners initially introduce the intervention and explain the community-directed approach and how it can be planned, run and controlled by the community. Subsequently, the process is taken charge of by the community. The nearest health facility provides training and supervision as well as the commodities needed. The communities themselves organise and conduct their census, maintain treatment registers and decide when and where to carry out distribution interventions [2]. Selected community members (Community Health workers) are trained for the delivery of health services. The community keeps records which are periodically submitted to the local health facility. By so doing, a partnership is created and maintained between the community and the health facility [4].
Community Health Workers (CHWs) working under the CDI of malaria program play a vital role in primary health care of the community. They act as first line intervention providers for health issues in the community. Trained CHWs play active roles in preventive and health promotion activities in malaria interventions including population mobilization, voucher distribution, distribution and hang-up of ITNs. In addition, they are trained on the rapid diagnosis, home management and follow-up of simple malaria and the timely referral of complicated malaria to appropriate health facilities [5].
Cameroon is ranked 18th among the first 20 countries worldwide which have the highest child mortality rate, with an overwhelming under-five mortality rate of 90. One deaths per 1000 live births in 2017. Malaria, though preventable and treatable, is the leading cause of death among the under-five population in Cameroon, accounting for more than 40% of deaths in this age group in Cameroon [6].
The use of Insecticide-treated bed nets is one of the measures of primary prevention of malaria. In 2009, UNICEF worked in collaboration with the Cameroonian government to secure funds from the Global Fund for Health to fight AIDS, Tuberculosis and malaria with a target of increasing bed net coverage from 13% to over 80% by the year 2015. However, as of 2012, only 13% of under-fives in Cameroon slept under ITNs and 54.8% by 2014 [7].
Based on facts presented by the WHO, an estimated 216 million cases were reported in 91 countries in 2016, which marked an increase of 5 million from 2015. Mortality due malaria was reported to be 445,000 deaths in 2016, a result similar to 446,000 recorded in 2015. The African region claims the highest proportion of malaria cases with 90% of the cases and 91% of the deaths recorded in 2016. African countries occupy 14 of the first 15 countries which carry 80% of the global burden of malaria, with Nigeria alone accounting for 27% of malaria cases and 24% of malaria deaths in 2016 [8].
Children below 5 years are usually more susceptible to malaria especially in high transmission areas. Malaria remains a major cause of mortality, claiming the life of child every two minutes. Although the number of malaria deaths in this age group has declined from 440,000 in 2010 to 285,000 in 2016, more than two thirds of malaria deaths (70%) occur in this age group [6].
Although a decreasing trend was observed in the general national prevalence of malaria from 41% in 2008, through 36% in 2010 to 31% in 2011, as well decreasing malaria-related deaths from 29% in 2009 to 19% in 2011 [4], there was a sudden 35.45% increase of malaria deaths from 2012 (3209 deaths) to 2013 (4348 deaths). Likewise, the under-five deaths in Cameroon due to malaria saw a decrease from 67% through 66% to 62% in 2010, 2011 and 2012 respectively, but then a sudden rise to 69% in. Malaria accounted for 22% of the deaths in health care facilities in 2013, with under-five mortality due to malaria in 2015 reported at 7028 deaths [9].
Community health workers play an important role in primary health care. They act as first-responders to community members. The activities of the CHW under the CDI of malaria include prevention education, early diagnosis and home management of simple malaria (HMM).
CHW carry out health education and promotion through voucher distribution, distribution and hang-up of ITNs and dissipating health information on effective parasite and vector preventive measures. There is demonstrated increase in the coverage of distribution and use of ITNs when CHWs are involved than when it is done from a focal point [10].
Furthermore, they are trained to carry out and interpret RDT of malaria and to treat positive cases of uncomplicated malaria. However, the reliance on CHWs to carry out RDTs and prescribe treatment remains controversial. While a majority of CHW demonstrate a mastery of the effective use and interpretation of RDTs, some demonstrate otherwise [11]. Nevertheless, proper training and monitoring as well as adherence to guidelines have been shown to subsequently improve their performance in carrying out critical steps of the diagnosis procedure [12].
Through regular home visits carried out by the CHW, children presenting with fever start receiving treatment as early as within the first 24 hours of onset hence decreasing progression to fatal complicated malaria-related deaths [13]. This has a great impact especially in remote areas where health facilities are not easily accessible or where there is a shortage of personnel in the health facilities.
Complicated cases of malaria are timely referred to the appropriate health facilities for proper management. They are trained to identify signs and symptoms which warrant referral to the health facilities. Studies on the referral pattern of CHWs shows increased referral among those using RDTs prior to treatment initiation compared with those who used just presumptive diagnosis from signs and symptoms [14].
The presence or absence of a host of factors either potentiate or hinder the performance of CHWs.
These factors could be grouped into personal (age, marital status, level of education), professional (e.g., training, supervision, job security), organisational (e.g., infrastructure, availability of work material, transport) and external workenvironmental factors such as co-worker relationship, community acceptance and appreciation [15].
A minimum of secondary level education as well as monthly meeting with supervisor have been shown to be positively associated with optimal service delivery performance by the CHWs [16].
However, there is need to ensure consistent availability of equipment supplies and transport to improve their credibility to and acceptability by the communities they serve [3].
Human resources constitute a major factor in health interventions [17]. Cameroon experiences a shortage of medical personnel with less than two doctors for every 10,000 people. Thus, certain health treatments are usually provided by nurses. This overwhelming medical workforce shortage necessitates the contribution and corporation of the members of the community in both preventive and basic treatment services. Intervention programs make use of the potentials of the human resource from the community by recruiting, training, financing and supervising community health workers [17]. Community members willing to take up the duty to serve as community health workers are required to be meeting up with the minimum physical, mental, intellectual and integrity requirements and be properly trained and periodically supervised to ensure quality health service delivery to the community [18].
The effective function of CHWs decreases morbidity and mortality caused by malaria of community members especially in children below five years of age. The CDI strategy makes use of these possible functions and capabilities of the CHWs in malaria intervention. Therefore, for this intervention to be effective in the roll-back of malaria, the CHWs should have a solid knowledge on and a positive attitude towards the intervention, as well proper required practices. In addition, there should be favourable working conditions, proper monitoring and supervision as well as a consistent reliable supply of intervention materials [19].
Although previous intervention programs (both national and international) have been operational in the Ndop health district prior to the introduction of the CDI of malaria, they have not been satisfactorily effective in the roll-back of malaria in the district; hence he reasons for his study.
Objectives of the Study
General objective
To evaluate the effectiveness of the Community-directed intervention in the roll-back of malaria among the under-five population of the Ndop Health District.
Specific objectives
• To determine the difference in the incidence of morbidity and mortality due to malaria between the pre-CDI period and the CDI period among the under-five population.
• To assess the proportion of CHWs who attain their minimum monthly target of 50 home visits per month in the three consecutive preceding months.
• To assess the personal, professional, organizational and external work environmental factors which influence the service delivery of the CHWs in the Ndop Health District.
Methodology
Description of the study area
This study was carried out in the Ndop Health District which is one of the 19 health districts in the North West Region of Cameroon. The Ndop health district is a rural area and covers the entire Ngoketunjia division with a surface area of 1126 km2 (Cameroon National Institute of Statistics, 2015). The total population of the health district is estimated at 21508 people, and the under-five population at 38715 children (NW Annual malaria report, 2016). The Ngoketunjia division is further divided administratively into three subdivisions, namely Babessi, Balikumbat and Ndop-Central sub-divisions. These 3 subdivisions are made up of 13 villages including Baba-1, Babungo, Babessi, Bafanji, Balikumbat, Bamali, Bambalang, Bamessing, Bamunka, Bamunkumbit, Bangolan, Baligashu and Baligansin.
The Ndop health district is bounded to the North, South, East and West by the Bangoren, Tubah, Kumbo East, and Fundong and Oku health districts respectively. Its natural vegetation consists typically of savannah grassland, though some areas consist of the tropical equatorial forest vegetation due the presence of eucalyptus trees. It is a lowland area surrounded by hills with several streams that empty into the Bamenjim Dam.
The Ndop Health district has two annual seasons; rainy and dry seasons. The rainy season spans from late March to early October and is usually characterized by torrential rains, thunderstorm, lightening and hailstones. The dry season spans from November to early March and is characterized by cold, chilly harmattan winds.
The health district comprises 15 health areas. Among these, 14 are accessible by road, while one (Mbissa) is accessed by water across a dam (Bamendjim Dam). Within the 15 health areas are found 26 health facilities; 15 public, 7 confessionals and 4 private facilities. Under the CDI program, there are a total of 191 trained community health workers.
Media coverage in the health district consists of the National Radio Television Station (CRTV) and three community radio stations namely Ngoketunjia Radio (Stone FM), Balikumbat community radio, and Babungo Community radio.
Study population
The study population of this study included children below five years in the Ndop Health district. Other source population in this study included the community health workers (CHWs) in the Ndop Health district as well as the supervisors and coordinators of the CDI of malaria program in this health district.
Study duration
This study included retrospective malaria data from 2013 till 2017. This study was carried out during the months of April and May 2018.
Inclusion and exclusion criteria
Inclusion criterion for choosing annual malaria data for the study was the period falling within calendar years between 2013 and 2017 during which complete monthly morbidity and mortality data for malaria were recorded at the district office from January to December. Any year during which complete monthly data was not available was excluded. Based on the above inclusion and exclusion criteria, the years 2013, 2016 and 2017 were included in the study.
Inclusion criteria:
• CHWs working under the CDI program in the Ndop Health District.
• CHWs who were actively serving during the previous three months leading up to the data collection.
Exclusion criteria:
• CHW not working under the CDI program in the Ndop Health District.
• CHWs who were recently posted or transferred to the CDI program unit.
Sampling method
The pre-CDI period (up until 2015) was considered to be the period before the implementation of the CDI of malaria in the Ndop Health District. From 2013 till 2015, only the year 2013 had complete recorded annual data for all the variables on mortality and morbidity needed for the study. Therefore 2013 was selected as the pre-CDI period of the study.
The CDI-period was considered to be the period after the introduction of the CDI of malaria in the Ndop Health District. This included the period beginning from January 2016. Therefore, the years 2016 and 2017 were selected as the CDI period for the study. Purposeful non-probability sampling method was used to select the years included in the study.
CHWs included in the study were also recruited using the Purposeful non-probability sampling technique.
Sample size calculation
The sample size for the number of CHWs to involve in the study was calculated based on the presumption that 40% of the CHWs, given the working condition and factors affecting their service delivery, were able to attain the minimum monthly target of 50 home visits per month in the three previous months (February, March and April 2018). This choice of this proportion is based on results obtained by from a similar study carried out in Iran whereby 40.5% of the CHWs were satisfied with their productivity [20-22].
The sample size (n) was calculated according to the formula:
z=1.96 for a confidence level (α) of 95%.
p=Proportion (expressed as a decimal).
N= Population size; i.e., the number of CHWs in the Ndop Health District.
e=Margin of error.
For this study,
z=1.96, p=0.4, N=191, e=0.05.
n=368.7936/2.9309=125.831.
n ≈ 126.
The sample size (with finite population correction) is equal to 126.
Study tools, schedules and checklists
Data collection sheets were used to record morbidity and mortality data from malaria report database at the level of the Ndop Health District.
Self-administered semi-structured questionnaires were used to collect data from the CHWs including data of their monthly coverage and factors affecting service delivery. These questionnaires were adapted from Research Guide on the Improvement of Health Care Delivery in Urban Communities in Africa using Community Directed Intervention Approach.
Questionnaires were distributed to CHW to fill at their convenience and recollected after three days. Data collection from the health district office was carried out simultaneously with distribution and collection of questionnaires.
Data collection
Data collection sheets were used to collect data on the morbidity and mortality of under-fives due to malaria in the health district office database from 2013 to 2017. This included the number of reported treated cases of simple and severe malaria, number of hospitalizations due to severe malaria and the number of deaths due to malaria.
Report registers of the CBO and COCs were examined to obtain the annual activities carried out by the CHW during the years 2013, 2016 and 2017 including home visits, number of rapid diagnostic tests carried out by the CHWs, number of simple malaria cases diagnosed using RDTs and managed by the by CHWs, number of fever cases referred to health facility by the CHW and ITNs distributions.
Coded questionnaires were administered to CHWs were used to obtain data on the factors affecting the implementation of the CDI of malaria by the CHWs. The questionnaires will be coded with numbers to help in data entry. The questionnaires will include questions on personal factors (age, gender, education, family status), professional status (duration of experience as CHW, satisfaction with training received, duration of contract as CHW, any other occupation or source of income beside CHW, job satisfaction), organizational factors include supervision (frequency of supervision, number of supervisors, on-field supervision, refresher training, register examinations), infrastructure (availability of transportation means, medical kits supply and storage and data entry registers); external work environmental factors (community perception and appreciation) and job satisfaction.
Data analysis
Data entry and analysis was done using the Excel 2013 and SPSS Version 20.0 computer software packages.
Histograms were used to demonstrate differences in the incidence of and mortality due to simple and severe malaria among under-fives between the pre-CDI period and the CDI period.
Frequencies, means and rates were calculated, and results demonstrated on tables and figures and presented for easy analyses.
Analysis including factors (personal, professional, organizational, and external) as predictor variables and service coverage as outcome variable were carried out and statistical significance were set at p value <0.05 as well as correlation between job satisfaction and monthly output (number of home visits carried out each month). Results were presented on tables and graphics.
Ethical considerations
• Participants were informed using an information sheet on the topic, procedure, benefits and potential risks of the study as well as the liberty to withdraw participation at any time.
• To ensure autonomy, signed consent was obtained from CHWs willing to participate in the study.
• To ensure anonymity, survey questionnaire did not bear the names of the participants.
Limitations of study and potential bias
The non-probability sampling methods were used to make the study subject to inclusion bias.
More so, the other malaria intervention programs in the Ndop Health District may act as confounders to the changes seen in the morbidity and mortality rate of malaria in the under-five population such as the introduction of free treatment of malaria by the government in 2014.
Furthermore, porosity in malaria data obtained from records especially in the pre-CDI period posed a problem since calendar years 2014 and 2015 had to be excluded from the study.
Results
The years included in the study were those for which complete annual malaria data for the Ndop Health District was available for analysis. These included calendar years 2013, 2016 and 2017.
Of the 126 questionnaires administered, 113 Community health workers participated in the study, giving a response rate of 89.7%.
Comparison of the morbidity and mortality between the pre-CDI (before 2016) and CDI period (as from 2016)
Malaria-related under-five deaths: In 2013 (pre-CDI), malaria is found to have caused 35% of the under-five deaths in the Ndop Health District, while in 2016 and 2017 (CDI period), this proportion reduced to 9% and 7% respectively as shown on Figure 1. Under the CDI there was a 74.2% and 80% reduction in malaria-related under-five deaths by the end of 2016 and 2017 respectively.
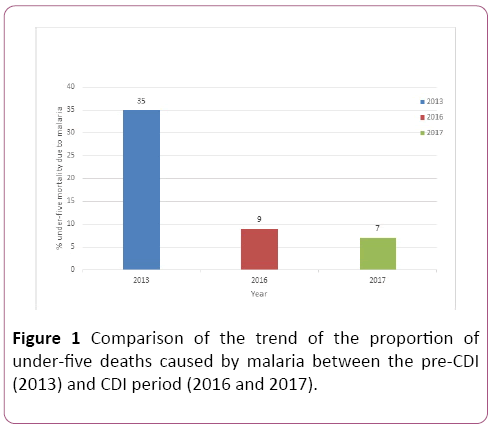
Figure 1: Comparison of the trend of the proportion of under-five deaths caused by malaria between the pre-CDI (2013) and CDI period (2016 and 2017).
Proportion of under-five hospital admissions due to severe malaria: In 2013, 40% of the under-fives hospital admissions in the Ndop Health District were due to severe malaria. In 2016, this proportion dropped to 28% and by the end of 2017, increased to 51% as shown on Figure 2.
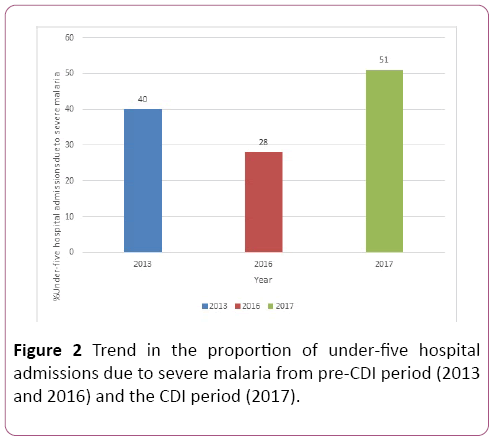
Figure 2: Trend in the proportion of under-five hospital admissions due to severe malaria from pre-CDI period (2013 and 2016) and the CDI period (2017).
Comparison of number of Rapid Diagnostic Tests (RDTs) carried out by Community Health Workers (CHW) between the pre-CDI (2013) and CDI period (2017)
Under the CDI of malaria program, there was a 24-fold increase in the number of RDTs carried out by the CHWs from 134 carried out in 2013 (pre-CDI) to 3271 carried out in 2017 (CDI) as demonstrated on Figure 3.
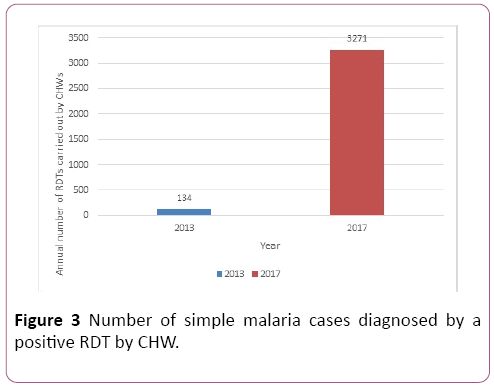
Figure 3: Number of simple malaria cases diagnosed by a positive RDT by CHW.
Comparison of the number of RDT-positive simple malaria cases diagnosed by the CHW
Under the CDI (2017), the number of under-five RDTpositive simple malaria cases diagnosed by the CHW (2657 children) had a 28-fold increase compared to the pre-CDI period of 2013 (95 children) as shown on Figure 4.
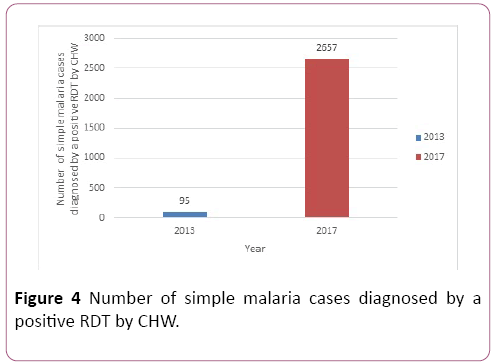
Figure 4: Number of simple malaria cases diagnosed by a positive RDT by CHW.
Proportion of CHW under CDI of malaria who carry out a minimum of fifty home visits monthly during the previous three consecutive months
Out of the 113 Community health workers involved in the study, 55%, 44.5% and 69.5% of them were able to carry out at least 50 home visits (HV) during the months of February, March and April respectively while 45%, 55.5% and 30.5% could not meet up with the minimum monthly target in the respective afore mentioned months (Figure 5).
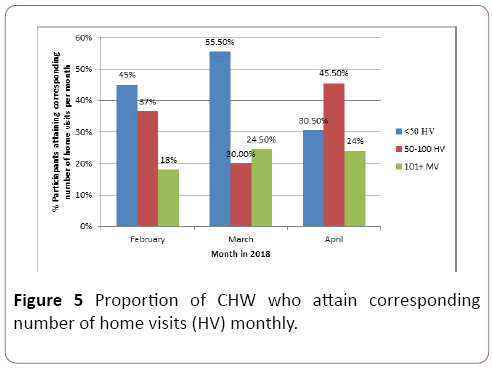
Figure 5: Proportion of CHW who attain corresponding number of home visits (HV) monthly.
Factors which influence the service delivery of CHW under the CDI of malaria in the Ndop health district
Demographic characteristics of study participants
Gender: A majority of the CHW sampled were males (53%) while females composed a minority of the sample population (47%) as demonstrated on Figure 6.
Figure 6: Distribution of CHW according to gender.
Age distribution of participants: Most participants had ages within the range 30 to 40 years (51.3%) while only one participant was more than 40-years-old (0.9%) as shown on Table 1.
| Variables |
Frequency |
Percentage |
Cumulative Percent |
| <25 years |
13 |
11.5 |
11.5 |
| 25-29 years |
41 |
36.3 |
47.8 |
| 30-40 years |
58 |
51.3 |
99.1 |
| >40 years |
1 |
0.9 |
100.0 |
| Total |
113 |
100.0 |
-- |
Table 1: Distribution of participants according to age.
Health area: As demonstrated on Figure 7, 16.5% of the Community health workers were sampled from Babessi health Centre, 10.16% from Babungo, 7.1% from Bamunkumbit, 21.2% from Baba, 31% from Bamunka, 6.2% from Bamali and 7.1% from Bafanji.
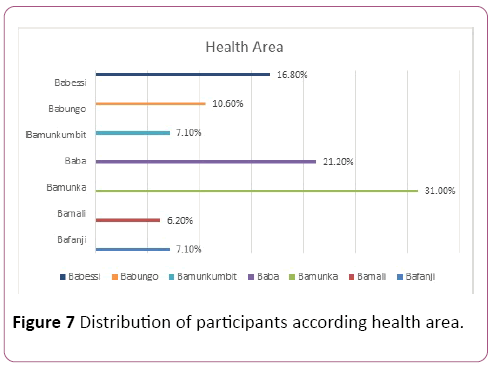
Figure 7: Distribution of participants according health area.
Assessment of personal factors
Academic qualification: A great proportion of the study participants had either primary level (45.5%) or secondary level (48.7%) as their highest level of education. Very few were either university graduates (3.5%) or had acquired vocational training of some sort (2.7%) as demonstrated in Table 2.
| Variables |
Frequency |
Percent |
Cumulative Percent |
| Primary |
51 |
45.1 |
45.1 |
| Secondary |
55 |
48.7 |
93.8 |
| University |
4 |
3.5 |
97.3 |
| Vocational |
3 |
2.7 |
100.0 |
| Total |
113 |
100.0 |
-- |
Table 2: Distribution of participants according educational qualification.
Family status: Among the CHW who participated in the study, an overwhelming majority (77.9%) were married while 12.4% were single as demonstrated on Figure 8.
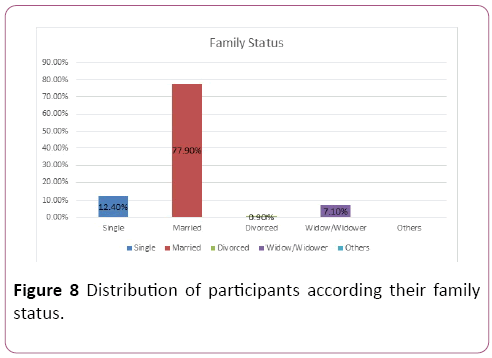
Figure 8: Distribution of participants according their family status.
Longevity of work experience as CHW: A huge majority (92.2%) of the participants had at least one-year experience of working as CHW under the CDI of malaria as well as prior working experience under other community health intervention programs (89.4%) as demonstrated on Table 3.
| Variables |
Item |
Positive responses
frequency |
% Positive response |
Negative response
frequency |
% Negative response |
| -- |
Working as a CHW under CDI of malaria for at least one year |
105 |
92.9% |
8 |
7.1% |
| Work experience as CHW |
Prior experience as a community health worker with any other health intervention program |
101 |
89.4% |
12 |
18.16 |
Table 3: Longevity work experience of study participants.
Assessment of professional factors
Incentive and supervision: Among the CHW involved in the study, 94.7% of them accepted to receive monetary incentive for their services as CHW. Up to 39.8% of them had no other source of income.
Furthermore, 74.3% of the participants reported that they have regularly monthly meetings with their supervisor while 25.6% of them had either irregularly-scheduled meetings or none (Table 4).
| Factor |
Item |
Positive responses
frequency |
% Positive response |
Negative response
frequency |
% Negative response |
| Incentives |
Motivation for working as a community health worker |
107 |
94.7% |
10 |
5.3% |
| -- |
Other source of income. |
68 |
60.2% |
45 |
39.8% |
| -- |
Joint meetings with your supervisors |
94 |
83.2% |
19 |
16.8% |
| -- |
Regularity of monthly scheduled supervisor |
84 |
74.3% |
29 |
25.6% |
| Monitoring and supervision |
Availability of field-based supervision by team leader or supervisor. |
103 |
91.2% |
10 |
8.8% |
| -- |
Availability of formal evaluation of performance within the last 12 months. |
108 |
95.6% |
5 |
4.4% |
Table 4: Provision of incentives and supervision.
Level of satisfaction with of training and refresher courses: While 76.1% of respondents accepted to have had at least one refresher course since working under the CDI of malaria program, 23.9% reported to have never had one (Table 5). Furthermore, when asked about their satisfaction with the level of training they have for their duties, most (73.5%) of the participants were satisfied while 11.5% were somewhat satisfied and 15.1% were not satisfied (Figure 9). Several suggestions were made with respect the need for refresher courses.
| Factor |
Item |
Positive responses
frequency |
% Positive response |
Negative response
frequency |
% Negative response |
| Refresher training courses |
Organization of refresher training course in community health service delivery under the CDI of malaria program. |
86 |
76.1% |
27 |
23.9% |
Table 5: Provision of refresher training courses.
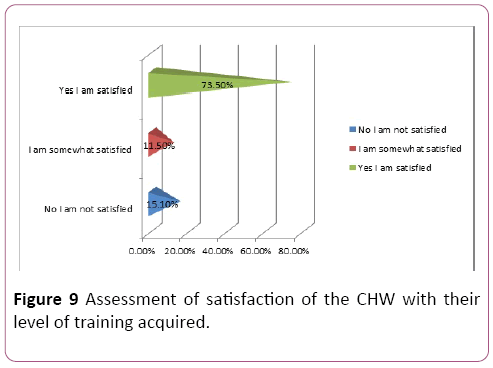
Figure 9: Assessment of satisfaction of the CHW with their level of training acquired.
Workload: While 43.3% of the respondents found their workload okay, 8.9% of them reported they were overworked. A majority (47.8%) of the respondents reported that they found their workload as community health workers manageable as shown on Figure 10.
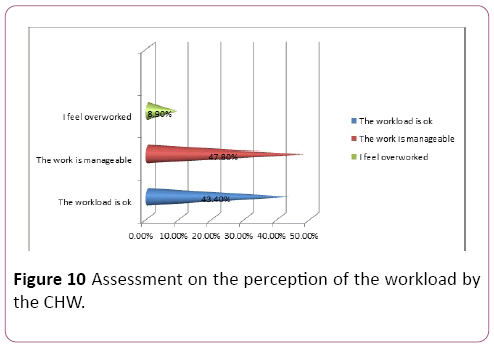
Figure 10: Assessment on the perception of the workload by the CHW.
Assessment of organizational factors
While majority of the respondents reported irregularity in the supply of both antimalarial drugs (64.6%) and RDT kits (73.5%), a majority of them said the supply of registers for records and the provision of transportation means were regular (71.7% and 69% respectively) as demonstrated on Figure 11.
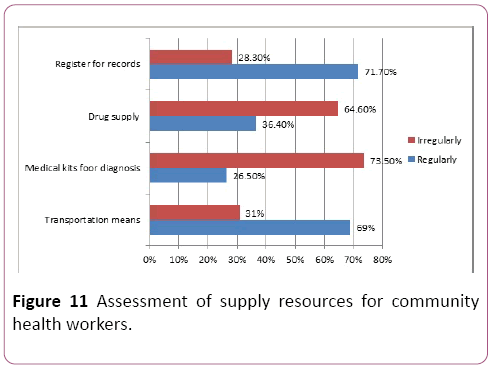
Figure 11: Assessment of supply resources for community health workers.
With regards to working material, several of the CHW suggested the need for certain materials in order to work effectively.
External work-environmental Factors
Acceptance and appreciation by community: Among the 113 CHW involved in the study, a majority (76.1%) of them felt accepted and appreciated all the time for their services by the community they serve while 1.8% of them felt almost always resisted as shown on Figure 12.
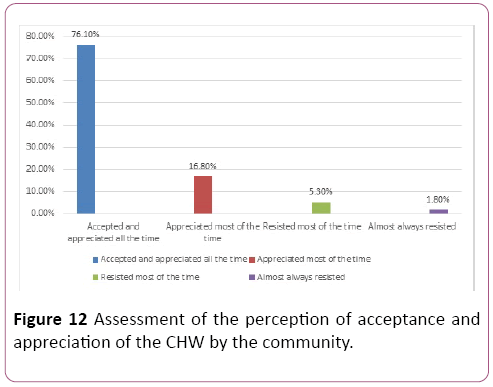
Figure 12: Assessment of the perception of acceptance and appreciation of the CHW by the community.
Job satisfaction: An overwhelming majority of the participants strongly agreed to the statement “In, general, I am satisfied with the job/work” while 1.6% somewhat agreed and 3.5% did not agree to this statement as demonstrated on Figure 13.
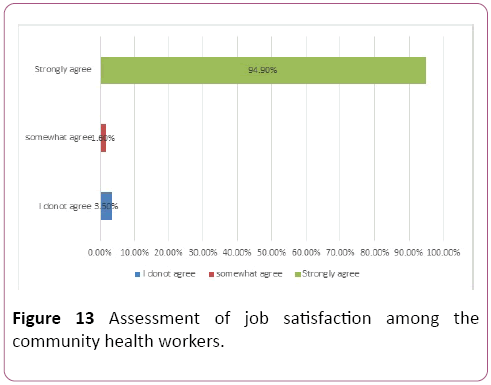
Figure 13: Assessment of job satisfaction among the community health workers.
Hypothesis
H1: There is a significant relationship between job satisfaction and monthly outcome (number of HV).
H0: There is no significant relationship between job satisfaction and monthly outcome.
Using Pearson Product Moment Correlation, there was a significant relationship between job satisfaction and monthly work output measured by number of hone visits (p= 0.01, r=0.18). The results obtained showed that the relationship is in a positive direction, meaning when job satisfaction increases, output of workers increase and vice versa as shown on Table 6.
| Variables |
Job satisfaction |
Monthly work output |
| Job satisfaction |
Pearson Correlation |
1 |
0.181 |
| Sig. (2-tailed) |
-- |
0.010 |
| N |
113 |
113 |
| Monthly outcome |
Pearson Correlation |
0.181 |
1 |
| Sig. (2-tailed) |
0.010 |
-- |
| N |
113 |
113 |
Table 6: Pearson product moment correlation between job satisfaction and outcome.
Discussion
In 2017 (CDI period), 45257 home visits were carried out by 191 CHW giving an average of approximately 20 monthly home visits per CHW. More than 40% of the CHWs involved in the study were able to meet their minimum monthly target of 50 home visits during the months of February, March and April 2018. This is similar to the results of a study carried out in Iran in which 40.5% of the CHW were satisfied with their monthly productivity [22]. This can be explained by the fact the organisation and implementation of CDI of malaria program in the Ndop Health District is adequate and well adapted for the Ndop context. This could also be due to the fact that the community member recruited under this program has a mastery of the community. Similarly, the age composition of the CHW in the Ndop Health District who participated in the study was predominantly below less than 40 years (99.1%). Therefore, they are energetic enough to meet up with the physical demands of the activities of a CHW, a finding similar to that obtained in Nigeria, Uganda and Burkina Faso whereby the performance of younger CHW was better than that of their older counterparts [20]. The month of December registered the lowest number of HV. This could be explained by the fact that in December; most of the CHW either travel for Christmas holidays or are preoccupied with the festivities of the season.
Most of the CHW involved in this study were married (77.9%) as well as a majority of them had previous experience working as a CHW under other intervention programs. However, considering the high monthly performance of the CHW, the findings are different from that obtained in the study carried out by Siribie et al., who demonstrated that single and new CHW had better performance when compared to their married and more experienced counterparts [20]. This difference could be explained by the fact that most CHW workers in our study were members of the community who, by working as CHW prior to the CDI, had gained a mastery of the terrain as well as were already known and identifies by members of the community for their services. While a majority of the participants found their current level of training satisfactory, there were several petitions made by the participants in the suggestion section of the questionnaire for refresher courses to enhance their performance (73.4%). The overwhelming interest in refresher training is similar to findings of Tilahun et al., in Ethiopia where by 88.5% of the CHW who participated in the study expressed interest in more frequent refresher training. Refresher training has been shown to enhance the accuracy in the performance of CHW especially in critical steps in carrying out RDTs of malaria as demonstrated by Counihan et al. [23]. With respect to workload (including visit schedules and travel distance), very few CHWs (8.9%) involved in this study expressed that they felt overworked. This is similar to findings obtained by Chin-Quee et al. in Rwanda whereby in an attempt to examine the CHWs’ perception of workload on the quality of service, performance and job satisfaction, results obtained demonstrated that 90% of the CHW found the workload either okay or manageable [24]. The lack of consistent provision of drugs and diagnostic kits as well as other materials needed for optimal work performance (lamps, rainboots, raincoats and umbrellas) were highlighted by participants as set-backs in the CDI program. This is similar to the problems identified by the CDI Study Group [19] during the pilot phase of program. This is also consistent with the finding of Druetz et al. in Burkina Faso where by frequent drug stock-out was one of the reasons of low utilization of the services of the CHWs by the community members [25]. Furthermore, a majority (76.1%) of the CHW involved in this study felt accepted and appreciated for their services. This is similar to the finding of Greenspan et al in Tanzania where by results of a qualitative study carried out to identify the sources of motivation for the CHW that resistance to the work of CHWs exhibited by families and community members was limited. However, this is different from the findings of Grant et al. in South Africa where by CHW where there was poor acceptability of the CHW by the community due to lack of trust and poor confidentiality [26].
Finally, an overwhelming majority of the study participants (94.9%) strongly agreed that they were generally satisfied with their job as community health workers. This is similar to findings obtained by Benpah in Ghana whereby 73% of CHWs expressed overall job satisfaction but much higher than the results obtained by Kabriaei and Moteghedi in Iran [22] whereby only 40.5% of participants were overall satisfied with their job. There was a positive correlation between job satisfaction and performance number of HV meaning that the performance of the CHW increased as their level of overall job satisfaction increased. This is similar to the findings of Kok et al. who demonstrated through a systematic review of several studies on factors influencing CHW performance that job satisfaction obtained through both intrinsic and extrinsic motivational factors, influence their performance positively [27].
Conclusion
The introduction and implementation of the communitydirected intervention of malaria in the Ndop Health District has benefited the population by decreasing the morbidity and mortality of children below five years in the community. Although there are several gaps in the implementation with respect to consistency in the supply of antimalarial drugs, RDT and other tools needed for optimal performance, the CHW are still able to meet up with their minimum monthly target and are generally satisfied with their job. CHWs are eager to enhance their competence as expressed by their desire for more refresher training courses.
While 43.3% of the respondents found their workload okay, 8.9% of them reported they were overworked. A majority (47.8%) of the respondents reported that they found their workload as Community Health Workers manageable. While majority of the respondents reported irregularity in the supply of both antimalarial drugs (64.6%) and RDT kits (73.5%), a majority of them said the supply of registers for records and the provision of transportation means were regular (71.7% and 69% respectively).
24036
References
- CDI Study Group (2010) Community-directed interventions for priority health problems in Africa: Results of a multicountry study. Bull World Health Organ 88(7): 509.
- Musoke D, Karani G, Ssempebwa JC, Musoke MB (2013) Integrated approach to malaria prevention at household level in rural communities in Uganda: Experiences from a pilot project. Malar J 12(1): 327.
- Austin-Evelyn K, Rabkin M, Macheka T, Mutiti A, Mwansa-Kambafwile J, et al. (2017) Community health worker perspectives on a new primary health care initiative in the Eastern Cape of South Africa. PLoS One 12(3): 0173863.
- Ndong IC, Van Reenen M, Boakye DA, Mbacham WF, Grobler AF (2014) Trends in malaria admissions at the Mbakong Health Centre of the North West Region of Cameroon: A retrospective study. Malar J 13(1): 328.
- Amoran OE (2013) Impact of health education intervention on malaria prevention practices among nursing mothers in rural communities. J Nigeria Med Assoc 54(2): 115.
- Edson DC, Massey LD (2010) Detection and identification of malaria parasite: A review of proficiency test results and laboratory practices. Lab Medicine 41(12): 719-723.
- Steketee RW, Campbell CC (2010) Impact of national malaria control scale-up programmes in Africa: Magnitude and attribution of effects. Malar J 9(1): 299.
- Salam RA, Das JK, Lassi ZS, Bhutta ZA (2014) Impact of community-based interventions for the prevention and control of malaria on intervention coverage and health outcomes for the prevention and control of malaria. Infect Dis Poverty 3(1): 25.
- Ruizendaal E, Dierickx S, Grietens KP, Schallig HD, Pagnoni F, et al. (2014) Success or failure of critical steps in community case management of malaria with rapid diagnostic tests: A systematic review. Malar J 13(1): 229.
- Counihan H, Harvey SA, Sekeseke-Chinyama M, Hamainza B, Banda R, et al. (2012) Community health workers use malaria rapid diagnostic tests (RDTs) safely and accurately: Results of a longitudinal study in Zambia. Am J Trop Med Hyg 87(1): 57-63.
- Mubi M, Janson A, Warsame M, Mårtensson A, Källander K, et al. (2011) Malaria rapid testing by community health workers is effective and safe for targeting malaria treatment: Randomised cross-over trial in Tanzania. PloS one 6(7): 19753.
- Lal S, Ndyomugenyi R, Magnussen P, Hansen KS, Alexander ND, et al. (2016) Referral patterns of community health workers diagnosing and treating malaria: Cluster-randomized trials in two areas of high-and low-malaria transmission in Southwestern Uganda. Am J Trop Med Hyg 95(6): 1398-1408.
- Sharma R, Webster P, Bhattacharyya S (2014) Factors affecting the performance of community health workers in India: A multi-stakeholder perspective. Glob Health Action 7(1): 25352.
- Wanduru P, Tetui M, Tuhebwe D, Ediau M, Okuga M, et al. (2016) The performance of community health workers in the management of multiple childhood infectious diseases in Lira, northern Uganda: A mixed methods cross-sectional study. Glob Health Action 9(1): 33194.
- Murray CK, Gasser RA, Magill AJ, Miller RS (2008) Update on rapid diagnostic testing for malaria. Clin Microbiol Rev 21(1): 97-110.
- Schumacher RF, Spinelli E (2012) Malaria in children. Mediterr J Hematol Infect Dis 4(1): 2012073.
- Sieleunou I, Kouontchou JC, Nguela AT, Yumo HA (2015) Removing the user fees for the under-fives' simple malaria treatment in Cameroon: Effect on the health services utilization. J Community Med Health Educ 5: 383.
- Siribie A, Moteghedi MS (2009) Job satisfaction among community health workers in Zehedan District, Islamic Republic of Iran. East Mediterr Health J 15(5): 1156-1163.
- Vitor-Silva S, Reyes-Lecca RC, Pinheiro TR, Lacerda MV (2009) Malaria is associated with poor school performance in an endemic area of the Brazilian Amazon. Malar J 8(1): 230.
- Kebriaei A, Moteghedi MS (2009) Job satisfaction among community health workers in Zahedan District, Islamic Republic of Iran. East Mediterr Health J 15(5): 1156-1163.
- Tilahun D, Fekadu A, Tekola B, Araya M, Roth I, et al. (2019) Ethiopian community health workers’ beliefs and attitudes towards children with autism: Impact of a brief training intervention. Autism 23(1): 39-49.
- Chin-Quee D, Mugeni C, Nkunda D, Uwizeye MR, Stockton LL, et al. (2015) Balancing workload, motivation and job satisfaction in Rwanda: Assessing the effect of adding family planning service provision to community health worker duties. Reprod Health 13(1): 2.
- Druetz T, Ridde V, Kouanda S, Ly A, Diabaté S, et al. (2015) Utilization of community health workers for malaria treatment: Results from a three-year panel study in the districts of Kaya and Zorgho, Burkina Faso. Malar J 14(1): 71.
- Grant T, Frost DR, Caldwell JP, Gagliardo RO, Haddad CF, et al. (2006) Phylogenetic systematics of dart-poison frogs and their relatives (Amphibia: Athesphatanura: Dendrobatidae). Bull Am Mus Nat Hist 15: 1-262.
- Kok G, Gottlieb NH, Peters GJ, Mullen PD, Parcel GS, et al. (2016) A taxonomy of behaviour change methods: An intervention mapping approach. Health Psychol Rev 10(3): 297-312.


