Hossain MM1*, Rahman MM2, Alam MS3 and Islam MM3
1Department of Surgery, Khulna Medical College, Khulna, Bangladesh
2National Institute of Cancer Research & Hospital (NICRH), Dhaka, Bangladesh
3Department of Surgical Oncology, National Institute of Cancer Research & Hospital (NICRH), Dhaka, Bangladesh
- Corresponding Author:
- Dr. Monoar Hossain
Associate Professor (Surgical Oncology)
Department of Surgery, Khulna Medical College
Khulna, Bangladesh
E-mail: dr.mdmonoar@gmail.com
Received Date: September 16, 2021; Accepted Date: October 04, 2021; Published Date: October 11, 2021
Citation: Hossain MM, Rahman MM, Alam MS, Islam MM (2021) Expression of HER2 in Gastric Carcinoma. Ann Clin Lab Res. Vol.9 No.10:375. doi: 10.36648/2386-5180.9.10.375
Copyright: © 2022 Hossain MM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction: Gastric cancer is the fourth commonest cancer worldwide. It is also recognized
as the second commonest cause of cancer related death in the global perspective. Although
the incidence of gastric cancer has gradually decreased over the last half of the century,
it varies among the different part of the world and different ethnic group. Mortality from
gastric cancer extremely high, and it is second only to lung cancer. Gastric cancer occurs
more frequently in men than in women.
Aim of the study: Aim of the study was to find out expression of HER2 in gastric carcinoma.
Material & Methods: This cross sectional study was conducted in the Department of
Surgical Oncology of National Institute of Cancer, Research and Hospital, Mohakhali, Dhaka.
The study period was from March, 2014 to April, 2015. A total of 80 patients were included
for the study. After receiving the gastrectomy specimen, it was fixed in 10% formaldehyde.
Data were compiled and necessary statistical analysis were carried out using computer
based software package for social science (SPSS 16.1). Ethical clearance was taken from the
ethical committee of NICRH.
Results: The highest patients were from 61-70 years age group and the lowest were from
71-80 years. The mean age of the patients was 59.71 (± 10.19) years. The female to male
ratio in this study was 1: 2.48. 66 (82.5%) patients were presented with anemia which was
followed by 39 (48.75%) cases with dehydration. Most of the tumors were located in the
distal part of the stomach (11.67%). Regarding staging 79(12.65%) patients were in the
advanced stage of the disease. The correlation between HER2 overexpression and TNM
staging has been tabulated below where it is shown that only Nodal (N) staging has the
significant correlation with the HER2 overexpression.
Conclusion: It is already mentioned that, in early history of immunohistochemistry, HER2
overexpression in case of carcinoma stomach was highly varied in different studies (from
9-92%). But recently, it was found around 9-32%, in several studies all over the world. It is
necessary to conduct further studies with larger samples and long term follow-up in order
to draw definite conclusions regarding the role of HER2/neu over expression.
Keywords
Gastric cancer; Expression; HER2; Epidermal; Prognosis
Introduction
Gastric cancer is the fourth commonest cancer worldwide. It is also recognized as the second commonest cause of cancer related death in the global perspective [1]. Although the incidence of gastric cancer has gradually decreased over the last half of the century, it varies among the different part of the world and different ethnic group [2]. Gastric cancer is one of the most common cancers worldwide, ranking fourth in overall frequency, and accounting for over 870,000 new cases and over 650,000 deaths annually [3]. Presently the mortality rates of gastric cancer are extremely high, placing second right after lung cancer. Generally, a higher male prevalence is observed among gastric cancer patients. An estimated 558,000 men and 317,000 women are affected by gastric cancer worldwide, accounting for about 5.5% of malignancies in men and 3.1% of malignancies in women, excluding skin cancer cases [4]. Although the incidence and mortality rates of gastric carcinoma have been steadily decreasing due to medical advancements, the increase in average lifespan of the populace has resulted in a situation where the total number yearly new cases are increasing [4]. The incidence of gastric carcinoma is extremely rare in those younger than 30 years, but it shows an extremely fast increase after that, with the oldest age groups being in the highest risks of gastric carcinoma. There are mainly two types of pathological variants in gastric cancer, intestinal type and diffuse type. The intestinal type is the outcome of an inflammatory procedure that initially advances from chronic gastritis to atrophic gastritis, and then from atrophic gastritis to intestinal metaplasia and dysplasia. This type of gastric carcinoma is more prevalent in the male population compared to the diffuse type, and the incidence rates increases sharply with age. On the other hand, the diffuse type carcinoma impacts the younger population more, and is prevalent in females. However, the incidence of the diffuse-type carcinoma may be increasing [5], which is worrying given that these types of tumors have a worse prognosis [6]. Recent studies showed that Human epidermal growth factor receptors are involved in the pathogenesis of gastric and gastroesophageal carcinoma and molecular target in advanced GC personalizing treatment [7,8]. The HER2 proteins are a type of growth factor receptors, coming from the family of Epidermal Growth Factor Receptors (EGFRs). An increase in HER2 has also been observed for cancers localized to the gastro-oesophageal junction, some probably originating from the distal oesophagus caused by gastro-oesophageal reflux [9]. In Bangladesh, almost all cases of gastric cancer are diagnosed in the advanced stage. Though much improvement has been achieved regarding survival of the patients of gastric cancer; still the prognosis is poor due to frequent metastasis [10]. Cancers of the cardia and gastroesophageal junction often exhibit a different pathogenesis to non-cardia carcinomas, and are showing a continuous increase in the incidence rate. With an increasing understanding of the molecular biology and the availability of genomics and proteomics analyses, HER2 has now been recognized to have an implication in other forms of cancer, especially gastric cancer.
Objectives
General objective
• To find out expression of HER2 in gastric carcinoma.
Specific objectives
• To find out expression of HER2 in gastric carcinoma regarding histological type.
• To find out expression of HER2 in gastric carcinoma according to tumor location.
• To find out expression of HER2 in gastric carcinoma according to the stage of the disease.
Methodology and Materials
This cross sectional study was conducted in the Department of Surgical Oncology of National Institute of Cancer, Research and Hospital, Mohakhali, Dhaka. The study period was from March, 2014 to April, 2015. A total of 80 patients were included for the study according to following inclusion and exclusion criteria. After receiving the gastrectomy specimen, it was fixed in 10% formaldehyde. After fixation a systemic gross examination was performed and adequate tissue sections were submitted and embedded in paraffin. Then histologic sections with 3-5 micron thickness were obtained from paraffin blocks and was initially stained with hematoxylin eosin for histological assessment. H & E stained slides were evaluated for histological examination (tumor classification, grading, and depth of tumor, nodal stage and lymphovascular invasion). Gastric cancer was classified histopathologically according to Lauren’s system (Intestinal, diffuse and mixed) and on the grading (well differentiated, moderately differentiated and poorly differentiated). Only the gastric adenocarcinomas, diagnosed in hematoxylin and eosin sections were selected for immunohistochemical examination. Endogenous peroxidase activity was removed by being kept in 3% hydrogen peroxide. Finally the sections were counterstained with Mayers hematoxylin. Data were compiled and necessary statistical analysis were carried out using computer based software package for social science (SPSS 16.1). Ethical clearance was taken from the ethical committee of NICRH.
Inclusion criteria
• Patients with any age, sex, stage having histopathologically confirmed carcinoma stomach
Exclusion criteria
• Previous history of gastric surgery
• Patients with history of radiotherapy
Results
The highest patients were from 61-70 years age group and the lowest were from 71-80 years. The mean age of the patients was 59.71 ( ± 10.19) years. The age followed almost gradual increase with increasing of age that was dropped suddenly in the last age group (Figure 1). Out of 80 patients of carcinoma stomach 57 were male (71.25%) and 23 were female (28.75%). The female to male ratio in this study was 1: 2.48 (Figure 2). Among the 80 respondents the maximum number of patients achieved primary education; 28(35%) which was followed by the number of patients with illiteracy; 24(30%). A considerable number of patients crossed SSC level; 15(18.75%) (Table 1). The income of majority of respondents were 10,000-20,000 BDT that means maximum patients came from middle class status. The housing status in majority of patients were semi-pacca. The sanitation status was acceptable in 69 (86.25%) patients (Table 2). More than half of the respondents were smokers. But among the above contributing parameters betel nut chewers were a little lower in number. The 52(65%) patients had the habit of taking additional salt intake that was a risk factor for developing carcinoma stomach (Figure 3). The leading number of patients presented with abdominal pain where the vague abdominal discomfort were also included. They were 75%. This clinical condition was followed by vomiting which coined 58.75% respondents (Table 3). Out of 80 patients 66 (82.5%) patients were presented with anemia which was followed by 39 (48.75%) cases with dehydration (Figure 4). There were 61.25% patients who possessed BMI 18-24.9 whereas 38.75% patients possessed BMI <18. There was no patient found with overweight and obese status (Table 4). Total 12.5% patients showed her2 positivity out of 80 respondents of carcinoma stomach (Table 5). Most of the tumors were located in the distal part of the stomach (11.67%). Regarding staging 79(12.65%) patients were in the advanced stage of the disease. More than half of cases were intestinal type (Table 6). The correlation between HER2 overexpression and TNM staging has been tabulated below where it is shown that only Nodal (N) staging has the significant correlation with the HER2 overexpression. Otherwise, tumor (T) and Metastasis (M) showed no significant relation with the HER2 overexpression. Here the p value was determined as<0.05 (Table 7). The correlation of HER2 overexpression with staging of carcinoma stomach has been depicted in the following table where it can be seen that the HER2 overexpression has no significant correlation with the staging of disease. Here the p value was determined as <0.05 (Table 8).
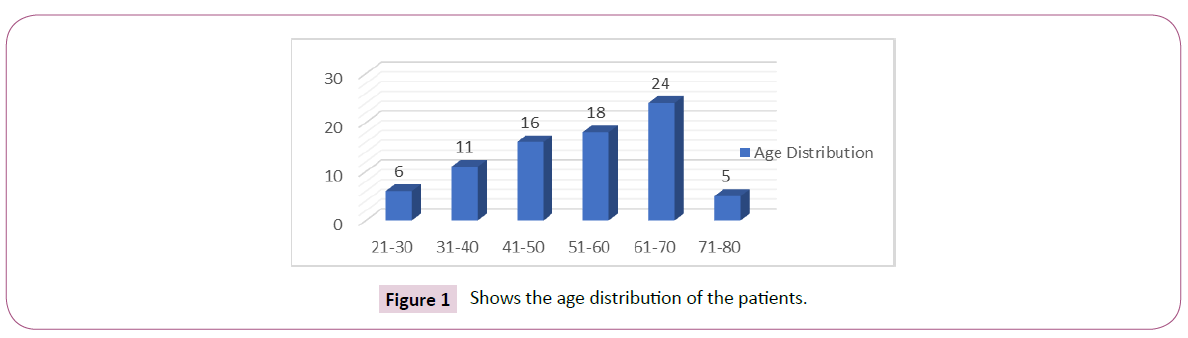
Figure 1: Shows the age distribution of the patients.
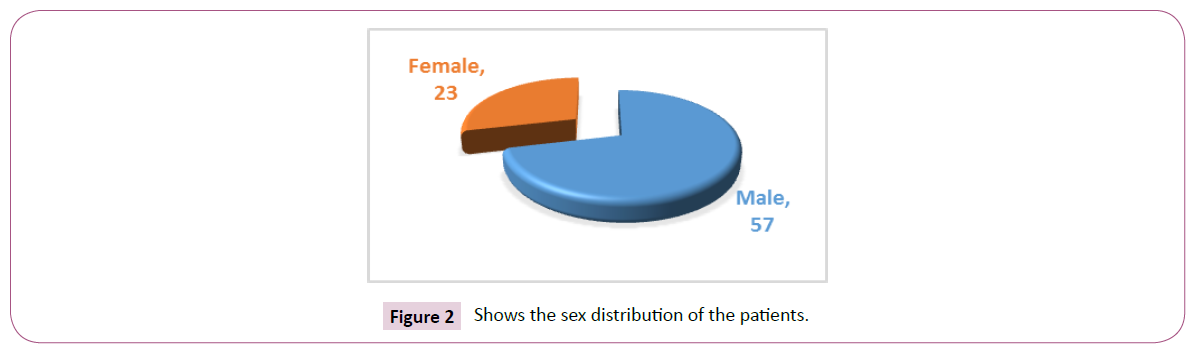
Figure 2: Shows the sex distribution of the patients.
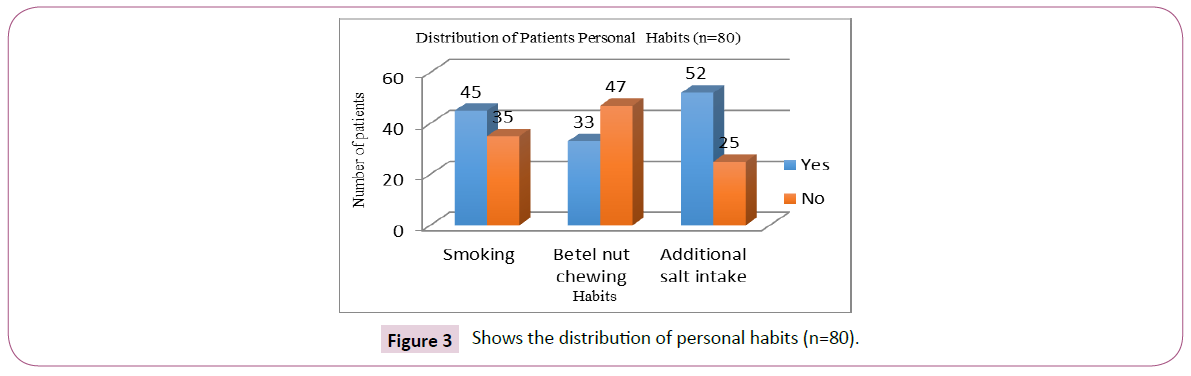
Figure 3: Shows the distribution of personal habits (n=80).
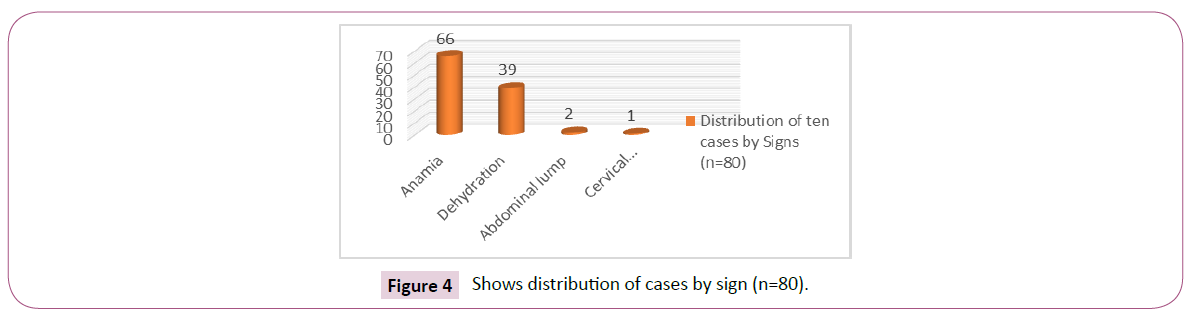
Figure 4: Shows distribution of cases by sign (n=80).
| S.L |
Level of Education |
No. of patients (%) |
| 1. |
Illiterate |
24(30%) |
| 2. |
Primary |
28 (35%) |
| 3. |
SSC |
15(18.75%) |
| 4. |
HSC |
8 (10%) |
| 5. |
Graduation & above |
5 (6.25%) |
| 6. |
Total |
80(100%) |
Table 1: Distribution of Educational Status of Patients (n=80).
| |
Frequency |
Percentage (%) |
| Income (Tk) |
| <10000 |
30 |
37.5% |
| 10000-20000 |
37 |
46.25% |
| >20000 |
13 |
16.25% |
| Housing |
| Kancha |
16 |
20% |
| Semi-Pacca (Tin shade) |
53 |
66.25% |
| Pacca |
11 |
13.75% |
| Sanitation |
| Poor |
11 |
13.75% |
| Acceptable |
69 |
86.25% |
Table 2: Comparisons of mean Parasitaemia of P. falciparum malaria-infected pregnant women by age group.
| Symptoms |
Frequencies (%) |
Percentage (%) |
| Weight loss |
19 |
(23.75%) |
| Anorexia |
34 |
(42.5%) |
| Abdominal pain |
60 |
(75%) |
| Weakness. |
29 |
(36.25%) |
| Vomiting |
47 |
(58.75%) |
| Dyspepsia |
13 |
(16.25%) |
| Dysphagia |
14 |
(17.5%) |
| Melaena |
9 |
(11.25) |
| Lump |
8 |
(10%) |
| Painless |
1 |
(0.8%) |
| Haematemesis |
2 |
(2.5%) |
Table 3: Distribution often causes by symptoms (n=80).
| Body Mass Index |
Number of patients |
Percentage (%) |
| <18 (underweight) |
31 |
(38.75%) |
| 18-24.9 (Normal) |
49 |
(61.25%) |
| 25-29 (Overweight) |
0 |
(0%) |
| = 30 (Obese) |
0 |
(0%) |
| Total |
80 |
(100%) |
Table 4: Distribution of patients according to BMI (n=80).
| Scoring |
No of patients |
Percentage (%) |
| 3+ |
9 |
11.25% |
| 2+ |
1 |
1.25% |
| 1+ |
10 |
12.50% |
| 0 |
60 |
75% |
| Total |
80 |
100% |
Table 5: Distribution of the cases by HER-2 positivity (n=80).
| Tumor morphology |
Frequency |
HER 2 Positive |
Percentage |
| Location |
| Proximal |
20 |
3 |
(15%) |
| Distal |
60 |
7 |
(11.67%) |
| Staging |
| Early |
1 |
0 |
(0%) |
| Advanced |
79 |
10 |
(12.65%) |
| Grading |
| Well to Moderately differentiated |
44 |
7 |
(15.91%) |
| Poorly differentiated |
36 |
3 |
(8.33%) |
| Laurence type |
| Intestinal |
45 |
8 |
(17.78%) |
| Diffuse |
35 |
2 |
(5.71%) |
Table 6: Distribution of correlation of patients with tumor morphology, frequency and HER2 positivity (n=80).
| T(Tumor) |
n |
Her2 |
X2 |
p-value |
| Positive |
Negative |
|
| T1 |
1(1.25%) |
0(0%) |
1(100%) |
0.5517 |
0.907NS |
| T2 |
29(36.25%) |
3(10.34%) |
26(89.66%) |
| T3 |
40(50%) |
6(15%) |
34(85%) |
| T4 |
10(12.5%) |
1(10%) |
9(90%) |
| N (Node) |
|
|
|
|
| N0 |
22(27.5%) |
0(0%) |
22(100%) |
9.6623. |
0.021S |
| N1 |
22(27.5%) |
3(13.64%) |
19(86.36%) |
| N2 |
24(30%) |
4(16.67%) |
20(83.33%) |
| N3 |
12(15%) |
3(25%) |
9(75%) |
| M (Metastasis) |
| M1 |
13(16.25%) |
8(61.54%) |
5(38.46%) |
1.1538 |
0.283NS |
| M2 |
2(2.5%) |
2(100%) |
0(0%) |
S: Significant.
NS: Not Significant.
P-value was calculated by chi-square test and Fisher’s Exact test. |
Table 7: Correlation of HER2 overexpression with TNM staging (n=80).
| T(Tumor) |
n |
Her2 |
X2 |
p-value |
| Positive |
Negative |
|
| Stage I |
14(17.5%) |
0(0%) |
14(100%) |
2.5725 |
0.4623NS |
| Stage II |
34(42.5%) |
5(14.71%) |
29(85.29%) |
| Stage III |
17(21.25%) |
3(17.65%) |
14(82.35%) |
| Stage IV |
15(18.75%) |
2(13.33%) |
13(86.67%) |
NS: Not Significant.
P-value was calculated by chi-square test. |
Table 8: Correlation of HER2 overexpression with Staging (n=80).
Discussion
Eighty patients were included in the study most them were from elderly age group, mean age 59.71, with male predominance (male: female=2.48:1). HER2/neu overexpression was present in 12.5% of gastric adenocarcinoma and was positively associated with only age and lymph node metastasis but not with other important clinicopathological variables. Park et al. [11] showed a 15.9% frequency of expression and through a univariate analysis found that protein expression, age ≥ 60 years old, tumor size ≥ 5 cm and advanced clinical stage are prognostic factors. Overexpression of HER2 protein in gastric cancer, using Immunohistochemistry (IHC), was first described in Sakai et al. [12]. Tanner et al. [13] observed HER2 amplification by Chromogenic Insitu Hybridization (CISH) in 12% of 131 gastric cancers, and in 24% of 100 GEJ tumors. The findings of our study are similar to the findings of the previously mentioned ones. We observed a statistically significant relationship between protein expression and age ( ≥ 60 years, p=0.0146) and lymph node metastasis. Our group reported a 12.5% of positive HER2 expression (IHC=3+ & 2+) in a series of 80 surgical specimen of gastric cancer patients. The difference of positive HER2 expression was observed in the present study, depending on the histology (intestinal type 17.78%. diffuse type 5.71%) and the primary localization of the tumor (15% proximal vs 11.67% distal). Following a modified HER2 scoring system Lordick et al. [14] are centrally testing tumor samples using both IHC and FISH to identify eligible patients for enrollment in the ToGA clinical trial. There are several studies that have analyzed the relationship between HER2/neu overexpression and clinicopathological characteristics in gastric cancer patients. Mizutani et al. [15] reported a frequency of gene expression of 14.2% and found a correlation with the depth of tumor invasion, histological subtype, growth pattern and liver metastasis. Yonemura et al. [16] found a positive correlation between the intensity of HER2/neu staining and tumor size, invasion to serosal layer and lymph node metastasis. All the studies mentioned above had a relatively low frequency of protein expression (9- 38%). According to Japanese series by Yenomura et al16, it was assumed that with immunohistochemical stain the rate of HER2 overexpression in gastric adenocarcinoma is 12% whereas in ToGA trial by Bang YJ et al. [17] it was reported 22.1%. But in our study, the HER2 overexpression was found only 12.5% which results match with that of Yenomura et al16 that is at the early age of the study in Japan. And hopefully, the experience in the field of immunohistochemistry for gastric carcinoma will play more vital role in future studies. However, we have found maximum cases according to T staging was in T3 stage (Locally advanced). But interestingly, there were some HER2 positive cases found from T2 and T4 group also. But we have found no statistically significant correlation with HER2 overexpression. On the contrary, the pathological Nodal stage showed statistically significant correlation with the HER2 overexpression. However, we have found maximum cases according to T staging was in T3 stage (Locally advanced). But interestingly, there were some HER2 positive cases found from T2 and T4 group also. But we have found no statistically significant correlation with HER2 overexpression. On the contrary, the pathological Nodal stage showed statistically significant correlation with the HER2 overexpression. The use of HER2/neu staining in surgical specimen biopsies limits the study only within the operated patients. The study done by Paola FB et al. [18] was depended on endoscopic biopsies that allows the test to be used in a greater number of patients, including patients who are not surgical candidates and would be referred for palliative chemotherapy and might benefit from combination chemo-immunological therapy.
Limitations of the Study
It is a cross- sectional single-centered study with small Sample size. Immunohistochemistry for gastric carcinoma is at its initial stage in our country also FISH procedure was not available.
Conclusion and Recommendations
We only found a relationship between protein expression with age and lymph node metastasis which were found statistically significant. Interestingly, there were multiple important variables that were correlated in this study with the HER2 overexpression. These variables were sex, tumor site, distant metastasis, Laurence histological classification. It is already mentioned that, in early history of immunohistochemistry, HER2 overexpression in case of carcinoma stomach was highly varied in different studies (from 9-92%). But recently, it was found around 9-32%, in several studies all over the world. It is necessary to conduct further studies with larger samples and long term follow-up in order to draw definite conclusions regarding the role of HER2/neu overexpression as an independent prognostic factor. Study should be multi-center basis. Multi-disciplinary approach should be mandatory to get a good outcome where the surgical oncologists, Thoracic surgeon, Gastroenterologists, Histopathologists, Geneticists are included. FISH procedures should be available for equivocal cases in every center. The experts involved in immunohistochemistry should go through continuous training.
Funding
No funding sources
Conflict of interest
None declared
Ethical approval
The study was approved by the Institutional Ethics Committee
40727
References
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, et al. (2011) Global cancer statistics. CA Cancer J Clin 61: 69-90.
- Montgomery E, Goldblum JR, Greenson JK, Haber MM, Lamps LW, et al. (2001) Dysplasia as a predictive marker for invasive carcinoma in Barrett’s esophagus. A follow-up study based on 138 cases from a diagnostic variability study. Hum Pathol 32: 379-388.
- Hamilton SR, Aalton L (eds.) (2000) Pathology and Genetics. Tumors of the Digestive System. IT’S Classification of Tumors 2. IARC Press: Lyon.
- Craanen ME, Dekker W, Blok P, Ferwerda J, Tytgat GN (1992b) Time trends in gastric carcinoma: changing patterns of type and location. Am J Gastroenterol 87: 572-579.
- Blok P, Craanen ME, Offerhaus GJ, Tytgat GN (1997) Gastric carcinoma: clinical, pathogenic, molecular aspects. QJM 90: 735-749.
- Bang Y, Chung H, Xu J, Lordick F, Sawaki A, et al. (2009) Pathological features of advanced gastric cancer (GC): Relationship to human epidermal growth factor receptor 2 (HER2) positivity in the global screening programme of the ToGA trial. J Clin Oncol 27: 45-56.
- Smith I, Procter M, Gelber RD, Guillaume S, Feyereislova A, et al. (2007) 2-year follow-up of trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer: a randomised controlled trial. Lancet 369: 29-36.
- Yamada Y, Kato Y (1989). Greater tendency for submucosal invasion in fundic area gastric carcinomas than those arising in the pyloric area. Cancer 63: 1757-1760.
- Wagner AD, Unverzagt S, Grothe W, Kleber G, Grothey A, et al. (2010) Chemotherapy for advanced gastric cancer Cochrane Database. Syst Rev 3: CD004064.
- Park WS, Oh RR, Park JY, Lee SH, Shin MS, et al. (1999) Frequent somatic mutations of the beta-catenin gene in intestinal-type gastric cancer. Cancer Res 59: 4257-4260.
- Sakai K, Mori S, Kawamoto T, Taniguchi S, Kobori O, et al. (1986) Expression of epidermal growth factor receptor on normal gastric epithelia and gastric carcinomas. J Natt Cancer inst 77: 1047-1052.
- Tanner M, Hollmen M, Junttila TT (2005) Amplification of HER-2 ingastric carcinoma: association with topoisomerase II alpha gene amplification, intestinal type, poor prognosis andsensitivity to trastuzumab. Ann Oncol 16: 273-278.
- Lordick F, Bang YJ, Kang YK, Otero Reyes D, Manikhas GM, et al. (2007) ‘HER-2 positive advanced gastric cancer; similar HER2- positivity levels to breast cancer. Eur J Cancer 5: 271.
- Mizutani T, Onda M, Tokunaga A (1993) Relationship of C-erbB-2 protein expression and gene amplification to invasion and metastasis in human gastric cancer. Cancer 72(7): 2083-2088.
- Yonemura Y, Ninomiya I, Yamaguchi A, Fushida S, Kimura H, et al. (1991) Evaluation of immunoreactivity for erbB-2 protein as a marker of poor short term prognosis in gastric cancer. Cancer Res 51: 1034-1038.
- Bang YJ, Van Custem E (2010) Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER-2positive advanced gastric or gastro esophageal junction cancer (TOGA): a phase 3, open-label, randomized controlled trial. Lancet 376: 687-697.
- Paola FB, Alejandra ZO, Quiñónez EU, Sergio SC, Angélica HG (2012) Clinical Significance of HER2/neu Overexpression in Advanced Gastric Cancer. Immuno-Gastroenterology 1:2, 136-142.


