Jien Sze Ho* and Wei Chieh Tan Jack
Department of Cardiology, National Heart Centre Singapore, Singapore
Corresponding Author:
Jien Sze Ho
Department of Cardiology, National Heart Centre Singapore
5 Hospital Dr, Singapore
Tel: 6567048000
E-mail: ho.jien.sze@singhealth.com.sg
Received date: April 15, 2017; Accepted date: April 22, 2017; Published date: April 28, 2017
Citation: Jien SH, Jack WCT. Extensive Dissection of the Left Internal Mammary Artery Graft and Emergency Bail Out. Arch Med. 2017, 9:2 doi: 10.21767/1989-5216.1000212
Copyright: © 2017 Jien Sze Ho. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Background: Left internal mammary artery (LIMA) bypass graft to the left anterior descending artery (LAD) have better long-term survival when compared with the use of a venous conduit to the LAD. It is a very important lifeline for coronary artery bypass patients and dissection of the LIMA is often disastrous.
This case illustrates an extensive dissection of the LIMA, involving the subclavian artery and aorta after bypass graft angiography. This was followed by an emergency bail out procedure.
Case Report: A 60-year-old gentleman presented with unstable angina underwent a routine diagnostic angiogram. Shortly after automated contrast injection of the left internal mammary artery (LIMA) graft, a column of contrast was found trapped in the subclavian artery. A review of the LIMA angiography revealed a spiral dissection extending distally from the ostial to distal LIMA, and also proximally from LIMA to subclavian artery down the aortic arch. Patient immediately deteriorated with hypotension and experienced chest pain. Emergency stenting of the left subclavian artery was performed. However, LIMA remained occluded. Cardiothoracic surgeons were consulted but acute redo coronary artery bypass was considered to be extremely high risk. In an attempt to bail-out the acutely occluded LIMA, we proceed with percutaneous coronary intervention of the native left anterior descending (LAD) artery chronic total occlusion. Fortunately, this was successful and stents were implanted from left main artery to distal LAD..
Keywords
LIMA dissection; Emergency coronary intervention; Chronic total occlusion
Introduction
Coronary artery bypass surgery with the use of at least one arterial graft was superior to percutaneous coronary intervention (PCI) in patients with left main or severe triple vessel disease. Left internal mammary artery (LIMA) bypass graft to the left anterior descending artery (LAD) have better longterm survival when compared with the use of a venous conduit to the LAD [1,2]. It is a very important lifeline for coronary artery bypass patients and dissection of the LIMA is often disastrous. This case illustrates an extensive dissection of the LIMA, involving the subclavian artery and aorta after bypass graft angiography. This was followed by an emergency bail out procedure. To our knowledge, this is the first reported case of a dissection of such massive extent with successful bail out PCI of the LAD chronic total occlusion.
Case Report
A 60-year-old gentleman presented with increasing frequency of exertional chest pain over few days. He has cardiovascular risk factors of hypertension, hyperlipidemia and a history of myocardial infarction with a coronary artery bypass graft surgery (CABG) done 10 years ago.
His electrocardiogram showed ST segment depression in the anterolateral leads. His physical examination revealed a normal blood pressure, heart rate and cardiovascular examination. His serial troponin levels were in the normal range and 2D echocardiogram showed an ejection fraction of 40%. He was diagnosed with unstable angina and underwent a routine diagnostic angiogram.
His coronary angiogram showed severe triple vessel with left main disease (Figures 1 and 2). Bypass graft angiography showed a patent LIMA graft, occluded vein graft to obtuse marginal artery, 90% stenosis in the vein graft to diagonal artery, 50% stenosis in vein graft to right posterior descending artery.
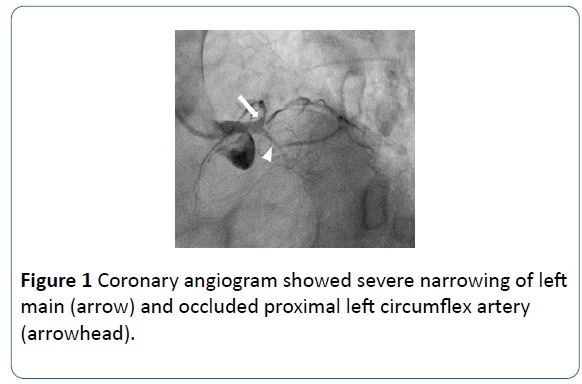
Figure 1 Coronary angiogram showed severe narrowing of left main (arrow) and occluded proximal left circumflex artery (arrowhead).
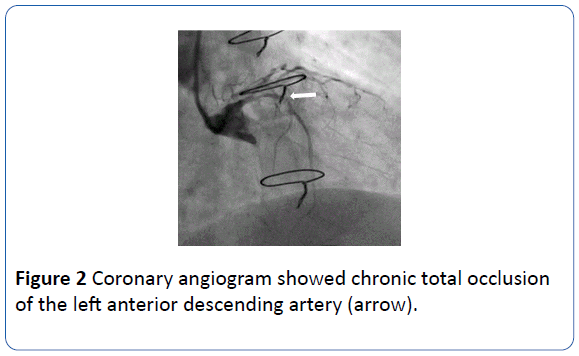
Figure 2 Coronary angiogram showed chronic total occlusion of the left anterior descending artery (arrow).
A Judkins Right coronary catheter was used to cannulate the LIMA. Shortly after automated contrast injection of the LIMA graft, a column of contrast was found trapped in the subclavian artery (Figure 3). A review of the LIMA angiography revealed a spiral dissection extending distally from the ostial to distal LIMA (Figure 4), and also proximally from LIMA to subclavian artery down the aortic arch (Figure 5). Patient immediately deteriorated with hypotension and experienced chest pain.
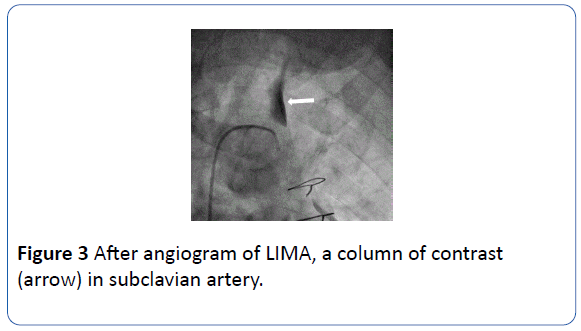
Figure 3 After angiogram of LIMA, a column of contrast (arrow) in subclavian artery.
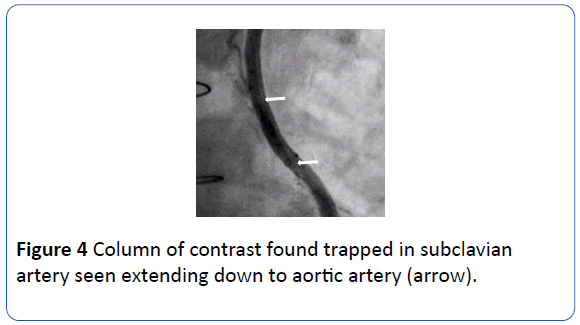
Figure 4 Column of contrast found trapped in subclavian artery seen extending down to aortic artery (arrow).
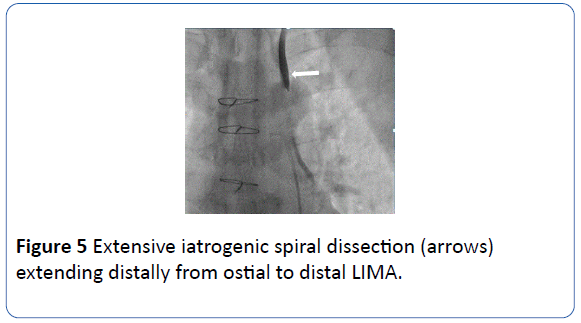
Figure 5 Extensive iatrogenic spiral dissection (arrows) extending distally from ostial to distal LIMA.
Emergency stenting of the left subclavian artery was performed (Figure 6) to seal the dissection flap and prevent further extension of the dissection. Multiple efforts to locate the ostium of the LIMA were attempted (Figure 7). However, LIMA remained occluded. Cardiothoracic surgeons were consulted but acute redo coronary artery bypass was considered to be extremely high risk.
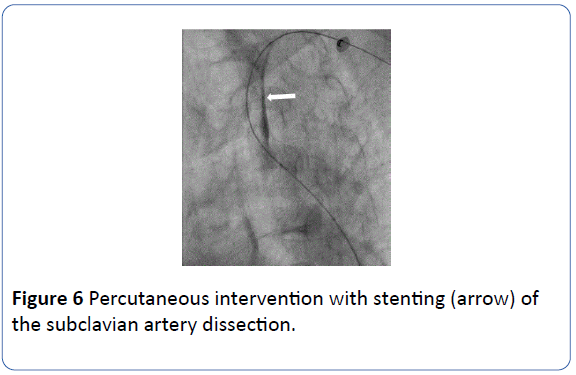
Figure 6 Percutaneous intervention with stenting (arrow) of the subclavian artery dissection.
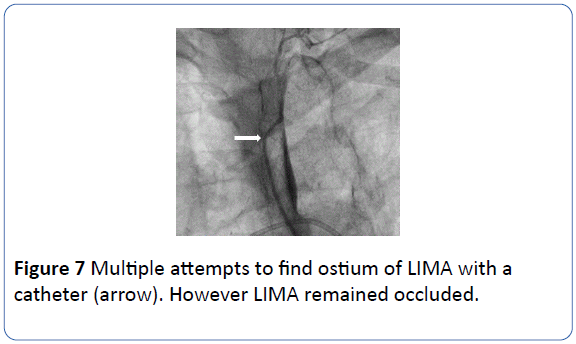
Figure 7 Multiple attempts to find ostium of LIMA with a catheter (arrow). However LIMA remained occluded.
In an attempt to bail-out the acutely occluded LIMA, we proceed with percutaneous coronary intervention of the native LAD chronic total occlusion (CTO) (Figure 8). Fortunately, this was successful and stents were implanted from left main artery to distal LAD (Figure 9).
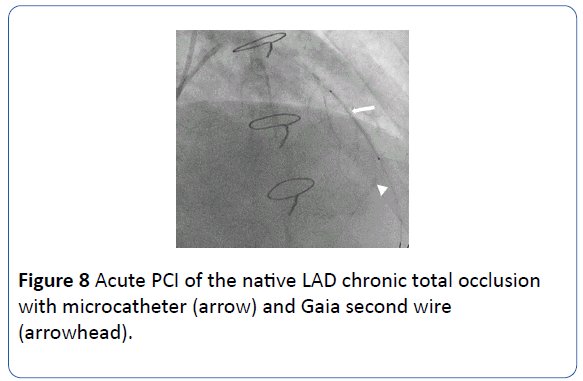
Figure 8 Acute PCI of the native LAD chronic total occlusion with microcatheter (arrow) and Gaia second wire (arrowhead).
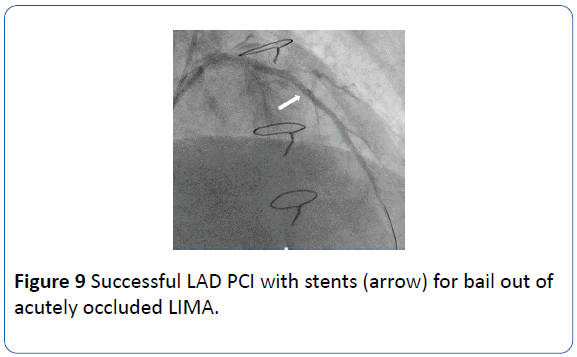
Figure 9 Successful LAD PCI with stents (arrow) for bail out of acutely occluded LIMA.
Discussion
This case illustrates an extensive iatrogenic catheter-induced dissection of the LIMA, involving the subclavian artery and aorta. The catheter was non coaxial to the LIMA and coupled with vigorous contrast injection have led to the dissection [3].
The LIMA can be a challenging vessel to catheterize due to its acute angle of origin from the let subclavian artery. For grat engagement, an IMA catheter is preferred over Judkins Right as it is more co-axial and catheter manipulation should be done very carefully to avoid complications [4]. Another risk factor of LIMA dissection could be the catheter size. Nonselective angiography of the LIMA via injection of the proximal subclavian artery as a scout arteriogram before selective cannulation of the LIMA graft can guide operator to an easier and safer selective engagement [5].
In this case, the extensive LIMA and subclavian dissection have compromised the flow of the LIMA leading to rapid deterioration of the patient. Despite multiple attempts, operator has failed to locate the ostium of the LIMA to perform bail out LIMA stenting. Cardiothoracic surgeons urgently consulted have deemed redo CABG as extremely high risk. At the crucial moment, the ability of the operator to perform a CTO PCI quickly and skilfully had led to the survival of the patient.
Catheter induced LIMA dissection carries the potential for catastrophic consequences [5]. When treating a LIMA dissection, emergency bailout stenting of the LIMA could be the only key to obtaining a rapid coronary reperfusion and hopefully possible success [4]. Other alternative was emergency bail out CABG [6] following failed angioplasty.
Conclusion
Engagement of the left internal mammary artery graft during routine bypass graft angiography should be done with utmost care to avoid complications. We advocate operators to develop procedural skills for treating chronic total occlusion as it may come in handy especially during similar emergency situations.
18987
References
- Cohn L (2001) Use of the internal mammary artery graft and in-hospital mortality and other adverse outcomes associated with coronary artery bypass surgery. Circulation 103: 483-484.
- Jones RH, Ryan TJ, Bennett E, Culliford AT, Isom OW, et al. (2005) Long-term outcomes of coronary-artery bypass grafting versus stent implantation. N Engl J Med 352: 2174-2183.
- Bapat VN, Venn GE (2003) A rare case of aortocoronary dissection following percutaneous transluminal coronary angioplasty: Successful treatment using off-pump coronary artery bypass grafting. Eur J Cardiothorac Surg 24: 312-314.
- Vatrano M, Ceravolo R, Dattilo G, Ciconte VA, Imbalzano E (2014) Left internal mammary artery dissection during percutaneous coronary intervention in hypertensive patients. J Clin Exp Cardiol 5: 5-6.
- Khan Z, Latif F, Dasari T (2014) Internal mammary artery graft dissection: a case-based retrospective study and brief review. Texas Hear Inst J 41: 653-656.
- Rasmussen C, Thiis JJ, Clemmensen P, Efsen F, Arendrup HC, et al. (1997) Significance and management of early graft failure after coronary artery bypass grafting: Feasibility and results of acute angiography and re-re-vascularization. Eur J Cardio-Thoracic Surg 12: 847-852.


