Aaron Hayson*, Justin Lee and Alexander RamirezValderama
General Surgery Residency at Florida State University College of Medicine and Tallahassee Memorial Healthcare
*Corresponding Author:
Aaron Hayson
General Surgery Residency at Florida State University
College of Medicine and Tallahassee Memorial Healthcare
Tel: +850-431-5567
E-mail: awh2830@gmail.com
Received date: May 13, 2017; Accepted date: May 23, 2017; Published date: May 30, 2017
Citation: Hayson A, Lee J, RamirezValderama A. Gallbladder Volvulus: A Case Study and Review of Literature. J Univer Surg. 2017, 5:3. doi: 10.21767/2254-6758.100080
Keywords
Gallbladder volvulus; Gallbladder torsion; Acute cholecystitis; Floating gallbladder; Chronic cholecystitis; Biliary peritonitis; Laparoscopic cholecystectomy
Introduction
Definitive preoperative diagnosis is difficult as it is often confused for acute cholecystitis. Gallbladder volvulus can lead to obstruction of biliary drainage and arterial flow leading to ischemia, necrosis, perforation and biliary peritonitis. However, with timely diagnosis and surgical intervention of these complications can be prevented. Currently the disease mortality is quite low at roughly 5%
Case Presentation
A 76 year old white female presented with severe right upper quadrant pain, nausea and emesis. The pain was described as achy and radiated to the right mid back. The patient’s past medical history included hypertension, hyperlipidemia, gerd and irritable bowel syndrome. Her surgical history included a hysterectomy with bilateral salpingo ophrectomy and repair of an enterocele. On examination, the patient was tender in the right upper quadrant without guarding or rebound. Laboratory values and vital signs showed the following:
A significant WBC of 18.8 was noted however the patient was afebrile. An Ultrasound was performed which showed no evidence of cholelithiasis (Figure 1) [1]. Biliary “sludge” was noted without cholecystic fluid or gallbladder wall thickening. Ultrasound impression was no acute process. A CT of the abdomen and pelvis was obtained. This showed a moderately distended gallbladder with pericholecystic fluid consistent with inflammation (Figures 2 and 3).
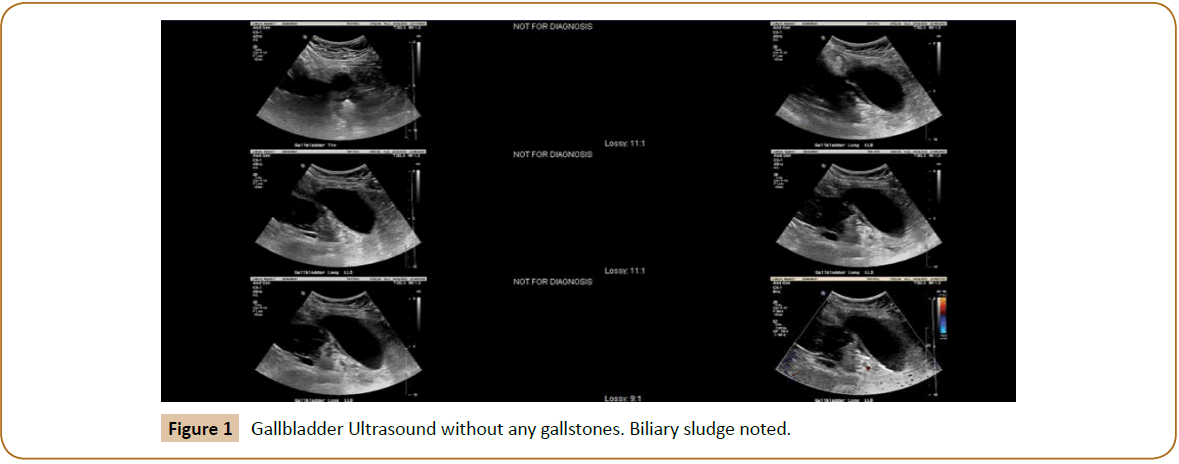
Figure 1: HPLC chromatogram of the nine reference compounds in 50% aqueous methanol, measured at 370nm. Retention times for rutin, sutherlandin A, sutherlandin B, kaempferol-3-O-rutinoside, sutherlandin C, sutherlandin D, quercitrin, quercetin and kaempferol were 11.9, 12.7, 13.8, 15.3, 16.2, 17.0, 18.0, 26.2 and 28.1 minutes, respectively.
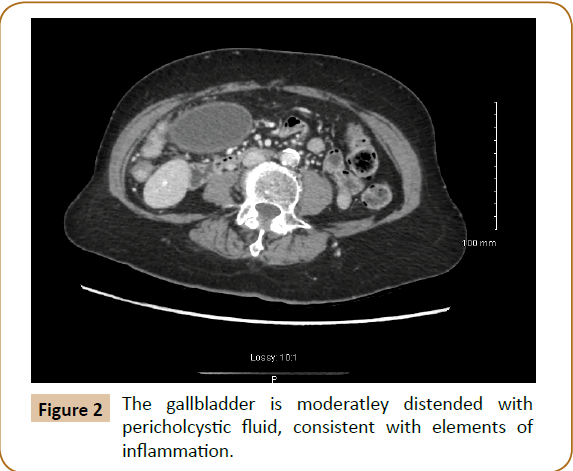
Figure 2: The gallbladder is moderatley distended with pericholcystic fluid, consistent with elements of inflammation.
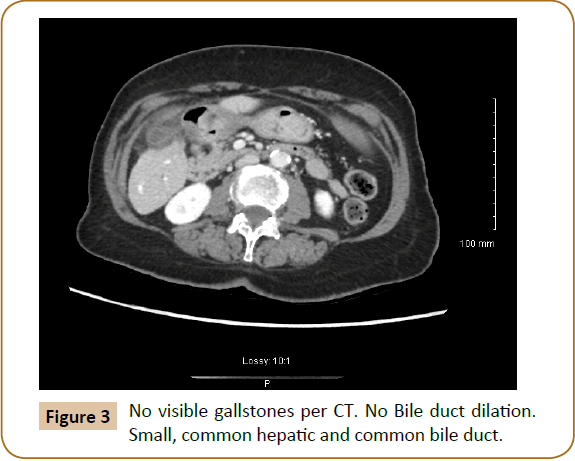
Figure 3: No visible gallstones per CT. No Bile duct dilation. Small, common hepatic and common bile duct.
The patient was consented for a laparoscopic cholecystectomy with intraoperative cholangiogram; possible open cholecystectomy. Intraoperatively, a floppy/floating gallbladder was noted without attachment to the liver with the exception of the cystic artery and cystic duct. The gallbladder was rotated about its longitudinal axis in a counter clockwise fashion. The gallbladder appeared necrotic (Figures 4 and 5).
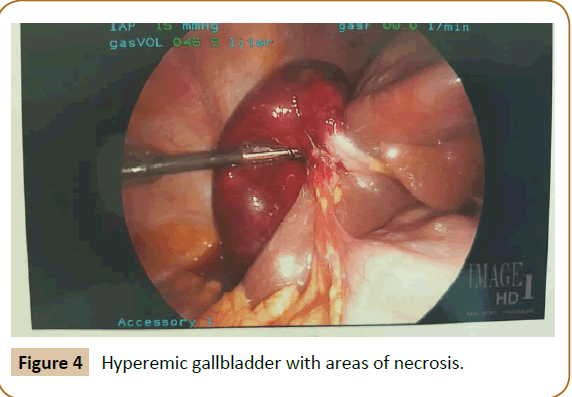
Figure 4: Hyperemic gallbladder with areas of necrosis.

Figure 5: Gallbladder torsed about its longitudinal axis, upper right is the infundibulum and neck of the gallbladder.
A cholecystectomy was performed in the routine fashion. Histological examination revealed a red-purple trabeculated mucosa. The serosa was hyperemic. The wall of the gallbladder measured to 0.5 cm thick. There were no stones within in the specimen. The gallbladder wall had extensive hemorrhage and necrosis consistent with torsion. The patient did well post operatively and was discharged to home the following day
Discussion
Gallbladder volvulus is a rare condition that is more prominent in older, Caucasian females and the incidence appears to increase with age [2]. Our patient fit this description.
The etiology of gallbladder volvulus is unknown but some underlying factors seem to be present. First the gallbladder is usually “floating” that is where the entire organ is in contact with the peritoneum and it is connected to the porta hepatis only by the cystic pedicle. A congenital anomaly may be present where an abnormally long mesentery can suspend the gallbladder away from the liver bed, thus increasing the chance for torsion. Likewise relaxation and atrophy of previously normal mesentery can cause visceroptosis [3].
But for the torsion to occur a triggering event has to occur. Liver atrophy, loss of visceral fat and elasticity, weight loss, atherosclerosis of the cystic artery and spinal deformities have all been theorized as possible triggering factors [4-7]. Interesting to note that our patient was very thin weighing just under 90 pounds, BMI 19.
Gallstones are unlikely to be the cause of torsion as they have been reported in only 20-33% of patients. One large study of 245 patients found stones in only 24.4%8 Preoperative diagnosis is difficult with fewer than a dozen cases found in the literature. Most diagnosis are made intraoperatively [8-11].
Conclusion
Gallbladder volvulus is a rare occurrence should be suspected in all patients presenting with signs and symptoms of acute cholecystitis, especially if they are elderly white woman. Delay in treatment can lead to necrosis, perforation and biliary peritonitis
19885
References
- Wendel AV (1898) A case of floatinggall-bladder and kidneycomplicated by cholelithiasis, with perforation of the gall-bladder. Ann Surg 27:199–202.
- Chung JC, Song OP, Kim HC (2010) Gallbladder torsion diagnosed by MDCT and MRCP. Abdom Imaging 35: 462–464.
- Aibe H, Honda H, Kuroiwa T, Yoshimitsu K, Irie H, et al. (2002) Gallbladder torsion: Case report. Abdom Imaging.27:51–53.
- Janakan G, Ayantunde AA, Hoque H (2008) Acute gallbladder torsion: An unexpectedintraoperativefinding. World J EmergSurg 3: 9.
- Pottorf BJ, Alfaro L, Hollis HW (2013) A clinician’s guide to the diagnosis and management of gallbladder volvulus. Perm J 17: 80–83.
- Tarhan OR, Barut I, Dinelek H (2006) Gallbladder volvulus: Review of the literature and report of a case. Turk J Gastroenterol17: 209–211.
- Ijaz S, Sritharan K, Russell N, Dar M, Bhatti T, et al.(2008) Torsion of the gallbladder: A case report. J Med Case Rep 2: 237.
- Chou CT, Chen RC, Yang AD, Wu HK (2007) Gallbladder torsion: Preoperativediagnosis by MDCT. Abdom Imaging32: 657–659.
- Reddy PK, Muralidharan M, Venkatasubramanian R, Yuvaraja S (2005) Laparoscopicderotation and cholecystectomy for torsion gallbladder. JSLS 9: 238–240.
- Gupta V, Singh V, Sewkani A, Purohit D, Varshney R, et al. (2009)Torsion of gallbladder, a rare entity: A case report and review article. Cases J 2:193.
- Garciavilla PC, Alvarez JF, Uzqueda GV (2010)Diagnosis and laparoscopicapproach to gallbladder torsion and cholelithiasis. JSLS 14:147–151.
- Koyanagi T, Sato K (2012) Complete gallbladder torsion diagnosedwithsequentialcomputedtomography scans: A case report. J Med Case Rep.6:289.

