Key words
Midnapore, West Bengal, Dengue Virus
Introduction
Dengue viruses are the members of the genus Flavivirus of the family Flaviviridae, consists four antigenically distinct Sero types, which do not offer cross protection. Dengue is an important mosquito borne disease in the world in terms of morbidity, mortality and economic cost [1], especially in the tropics, with more than 2/5th of the world population living in areas at risk for dengue [2-4]. Infection with any one of the four types leads to a mild, self limiting febrile illness (dengue fever, DF) A more severe form of the disease, dengue haemorrhagic fever (DHF)/ dengue shock syndrome (DSS), is responsible for high mortality rate, especially in children [5]. Dengue has now become a regular occurrence worldwide including America, Africa, Asia and the South Pacific, where the vector of the disease is wide spread. The incidence of DF is on the increase and spreading to geographic regions not previously affected. Movement of Dengue between different geographic areas and also from urban to rural is an important element in the epidemiology of the disease. From being a sporadic illness, epidemics of dengue have now become a regular occurrence all over the world. In India Dengue was first isolated in 1946 and many epidemics have since been reported [6-9].
The clinical features of dengue virus infection range from nonapparent infection through dengue fever (DF) and the more severe dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS) [10-12]. DHF/DSS, although common in South East Asia, has also been reported in India during Dengue epidemics. DHF was first reported in Calcutta, West Bengal, in 1963 [13] again in 1964 [14] and subsequently in different states of India [15-22].
Laboratory diagnosis of a recent dengue virus infection may be done by detection of the virus in patient’s blood, either by virus isolation in susceptible cell cultures [3] or by detection of the viral RNA by reverse transcriptase-polymerase (RT-PCR) chain reaction based techniques [23-24]. These processes are very specific and should be performed within 48 hrs following the onset of illness in a well equipped laboratory, as the virus disappears after that period. However, detection of IgM antibodies by ELISA method and detection of rise of antibody titres with the convalescent samples by Haemagglutination inhibition test are well accepted serological methods for the diagnosis of dengue infection.
This paper reports the detailed investigation of repeated outbreak of unknown fever in the year 2002, 2004 and 2007; in the district West Midnapore and establishes dengue activity in rural areas on the basis of laboratory investigations.
Methods
Location and Meteorological information
Midnapore was the biggest district in the state of West Bengal, having a sea port from the ancient time, with historical back grounds. Presently the district has been divided into East and West Midnapore. The district West Midnapore, our study area, is situated at an altitude of 23 meters above sea level on the bank of Bay of Bengal with an average rain fall of 1656 mm, mostly between the months of May and September. In the summer the temperature ranges from 42ºC to 50ºC with high humidity.
Sample collections and investigations
Investigation in the year 2002
Cases started occurring initially in the Guiadaha village of Gorbeta block followed by Salboni block. These two villages were worst affected and are situated 30-40 km from the district head quarter, surrounded by paddy fields and agricultural lands. Source of drinking water was tube wells. Village Guiadaha has a total population of 1541.It was a typical rural village with kachha houses and kachha road. The village has reported 311 cases since its onset, at the local primary health centre. During investigation, it was revealed that several people suffered from two episodes of fever, headache, nausea, abdominal pain and retro orbital pain at an interval of 4 days to 6 days. In most of the houses visited, stagnant and stored water were observed for regular uses, which facilitated the breeding of the mosquitoes. Mosquitoes were abundant at the village and day biting mosquitoes were also present. From 1st to 17th July, the numbers of daily attendants of fever cases in the OPD of the hospital were collected. During this visit a total of 288 blood samples were collected from the acute cases from two villages. Of which we could collect 63 blood samples from the OPD and from the indoor patients of the hospitals and rest of the 110 blood samples were collected by the local health workers and the medical technicians of the health centre on door to door visit.
The Salboni village has a total population of 5819. It is semi urban in settings. This village has reported 540 cases up to 14th July, 2002. In both the villages there were many cases, who suffered but did not report to any health facility. Only 115 blood samples could be collected from acute cases from the affected village.
After a fort night, Local health workers could collect only 74 paired blood samples at the convalescent stage from the two affected villages. These samples were sent to the ICMR virus unit, maintaining the cold chain.
Clinical manifestation
All the patients had the clinical features of continued fever, headache, pain all over the body, anorexia, epigastric pain, nausea and/or vomiting, extreme weakness, bleeding manifestations like, epistaxis, haematemesis, haematuria etc. only in one case, paetichial rash was observed.
Regarding seven death cases, one case died of paralytic illeus, three cases died of haematemesis, two cases died of haematuria and one case was brought dead to the hospital with a history of rapid up rise of fever followed by sudden collapse.
Investigation in the year 2004
This year, village Kesia, and Laxmanpur, of Garbeta block were affected. These two villages are about 90 km from the District Headquarter and adjacent to Salboni of West Midnapore. During investigation, it was revealed that the total populations of these two villages are 4059. Date of first case report was 16th May 2004, total number of fever cases up to 3rd June were 792. All the age groups were more or less affected. During this visit in the year 2004,139 and 115 samples were collected from Kesia and Laxmanpur respectively, in the manner adopted in the year 2002. The two patients who died in these villages had suffered from high fever with headache and cough associated with severe respiratory distress. During the time of investigation the outbreak was in declining state. There was no evidence of sex differentiation among cases. The distribution of clinical presentation among the cases and the age wise distribution of fever cases were collected from the health centre.
Clinical manifestations
All the cases had continued high fever, rashes all over the body with cough and mild respiratory symptoms. Majority of them had headache, nausea / vomiting, malaise and drowsiness with duration of 3 days to 5 days. Joint pain and backache were the common features in all the cases.
A total of 63 convalescent paired sera were collected after 15 days by the local health authority with the help of medical Technicians and health workers.
Sample collection in the year 2007
This year, again an outbreak of unknown fever took place in a mild form in all over the district. The clinical manifestation was almost same with the previous years. No death was recorded in this year. The health authority of the district West Midnapore took the initiative for collection of blood samples. A total of 239 blood samples from all over the district were collected by the doctors of Sadar Hospitals, block hospitals and the primary health centers. These samples were sent to us for necessary diagnosis.
A total of 58 convalescent paired sera were collected by the local health authority with the help of medical Technicians and the health workers. All the sera collected during different years, were transported on wet ice to the ICMR virus unit, Calcutta, where they were stored at -800C until tested. The possibilities of bacterial and prokaryotic etiology in the collected sample were excluded through investigations at the local hospitals. All the sera were tested within 1 month to 2 months from the date of collection.
Laboratory investigation
Virus isolation
Attempts were made to isolate the virus from the acute samples, if any, by using C6/36 cell lines. Two hundred micro liters of selected samples (2 days fever cases with dengue like symptoms) were spread over the monolayer of C6/36 cell line and allowed to adsorb for 120 minutes in an incubator at 28°C under 5% CO2 concentration. After adsorption, the excess sample materials were discarded and minimum essential media (MEM; GIBCO BRL, US) supplemented with 2% fetal bovine serum (FBS; GIBCO BRL, US) and Penicillin Streptomycin antibiotics (PenStrep; Gibco) were added in 24 well tissue culture plate (Tarsons) and were incubated again in the same condition as before. It was observed regularly for the appearance of cytopathic effect (CPE) up to 7-8 days.
Serology
The acute samples were tested for the presence of Dengue IgM antibody by IgM capture ELISA (MAC-ELISA) method, using a kit (Prepared by National Institute of virology, Pune, India), following the prescribed protocol. O.D was measured at 450 nm using an ELISA reader (Titertek Multiskan Plus, Lab systems Finland, Type- 314).
Haemagglutination inhibition test
A total of 195 convalescent samples could be collected from the affected areas and were tested along with the respective acute sera for any rise of HAI antibody in the convalescent state. The HAI test was carried out according to the method of Clarke and Casals [19]. For confirmation of the etiologic agent, the convalescent sera along with the acute samples were subjected to HAI test against Dengue and JE antigen. Samples were considered positive, if they had a fourfold rise of titer in the convalescent paired sera in comparison with the corresponding acute samples.
Results
Sample collections and investigations
The total number of fever cases attended the OPD of Guiadaha hospital from 1st July to 17th July has been presented (Figure 1).
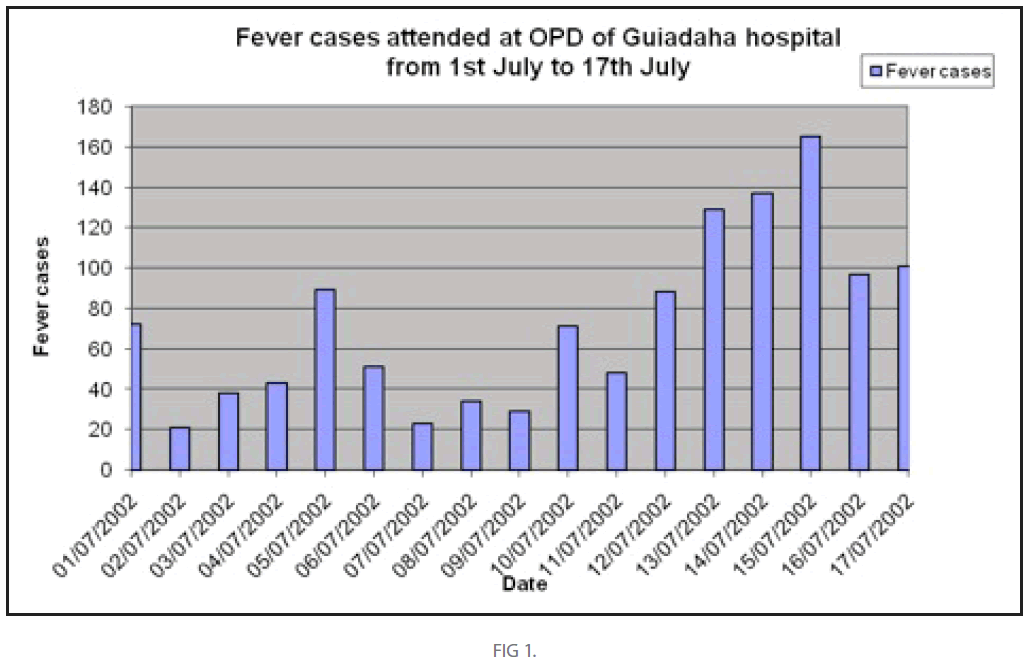
Figure 1
There was a steady increase in number of patients. On 15th July, 2002; highest no. of Patients attended the OPD.
Virus isolation
CPE was not developed and No virus could be isolated from any of the acute sera collected from fever cases.
Serology
Out of 781 acute blood samples, collected during these three years, Dengue Virus specific IgM antibodies were observed only in 446 (57.10%) samples. Year wise collection of acute samples and detection of Dengue IgM antibody in them, are presented (table 1).
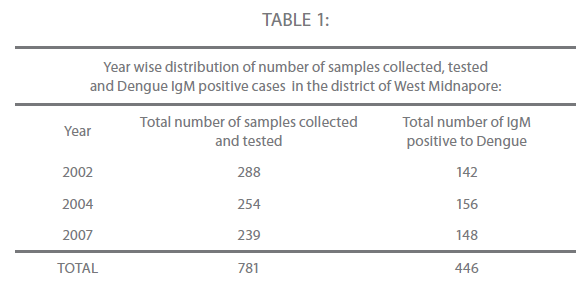
Table 1
Among the 781 patients’ samples tested, 453 were male and 328 were female. Out of 453 male, 217 (47.90%) were positive. On the other hand, 185 (56.40%) of the 328 samples collected from the female cases, were positive to Dengue IgM antibody. The sex wise distribution of suspected cases of Dengue and Dengue IgM positive cases have been presented (table 2).
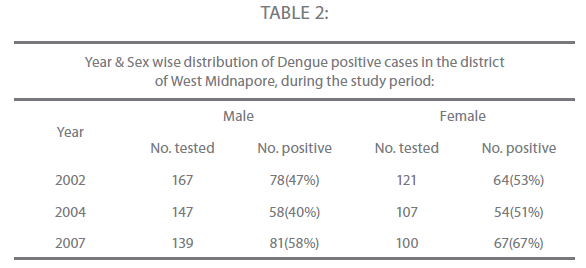
Table 2
There was a decrease in the number of the samples collected, during the three outbreaks, as compared to the year 2002. The age wise distribution of Dengue suspected cases and Dengue IgM positive cases have been presented (table 3).
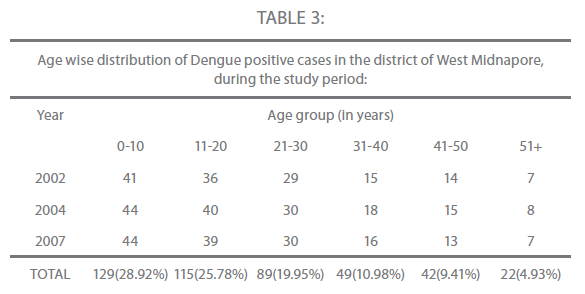
Table 3
In all the three years, the maximum IgM positive cases were observed in the age group of 0-10 (28.69%), as compared to the other age groups (Figure 2).
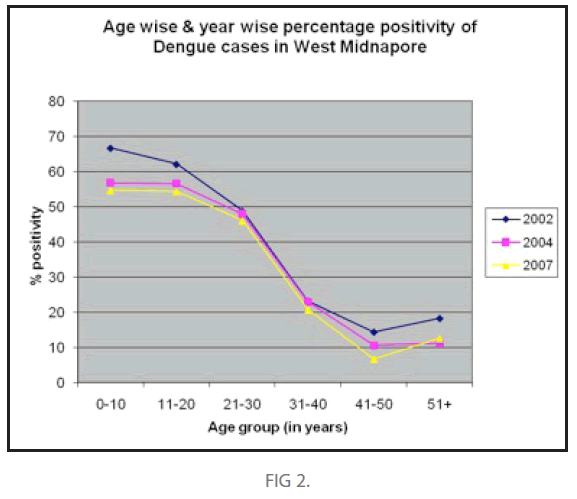
Figure 2
A total of 77 samples out of 195 convalescent sera revealed fourfold rise of antibody titre, in comparison with the acute sera, against Dengue antigen. Apart from that, only 27 sera had very low antibody titre against JE, both in acute and the convalescent stage. Rest of the convalescent samples did not produce any reaction either against dengue or against JE antigen. The results of the HAI test against Dengue and JE antigen have been given (table 4).
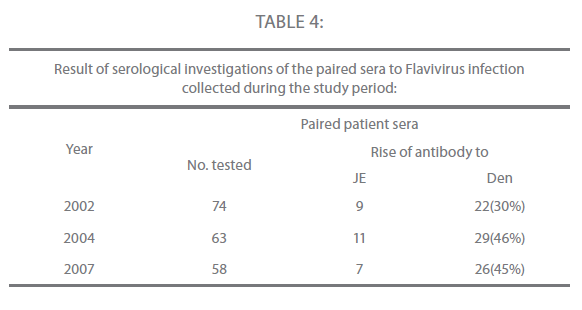
Table 4
Discussion
The epidemiology of Dengue is of continuing health importance, as the incidence of DF and DHS/DSS is increasing worldwide and is appearing in areas where it was previously unreported. In India, Den-1 and Den-4 was first reported in 1964 [25-26] and Den-3 in 1968 [27]. DHF was first reported in Calcutta, West Bengal in 1963 and in 1964 [13-14] Ever since, several reports of DF and DHF outbreaks have come from different cities in India and these include reports from Ludhiana [28], Lucknow [29], Chennai [30], Mangalore [31], Assam/ Nagaland [32] and Vellore [33]. In Delhi, although frequent outbreaks of DF have been occurring since 1967, major outbreaks of DHF and DSS have been reported in the year 1999 and 2001 [34-35]. All these outbreaks of DF and DHF/DSS have been recorded from the cities and the urban areas. No such outbreak has yet been recorded from the rural area like the district of West Midnapore, West Bengal. In the year 2002, all most one fifth of the total populations of the two villages were affected. Out of seven deaths, five cases had the symptoms of dengue haemorrhagic fever and one had the history of shock syndrome. More over the history of two episodes of fever at an interval of 4 days to 6 days in the same locality indicates the possible circulations of two types of Dengue viruses. This has in turn facilitated the haemorrhagic manifestations. The detection of IgM antibody to dengue virus by ELISA test, in 446 samples out of 781 cases, amply proves that the febrile illness was due to the dengue virus infection in the recent past (Table-1).
According to the sex wise distribution of the suspected cases (Table-2), there was a significant higher incidence of dengue IgM Sero positivity in females and not in males. This may be explained by the fact that the female individuals usually resides at home at the day time and get exposure to the mosquitoes (Aedes aegypti), as it is a domestic and peridomestic in nature.
A significant higher incidence of dengue IgM Sero positivity were observed in the age group of 0-10 years followed by 11-20 years(Table 3),(Figure 2), which is similar to the observations made by many workers at different times and from different parts of India. The results obtained in the convalescent sera by HAI test, revealed 4 fold rise of antibody titre in 77 samples, as compared with the acute sera. Only 27 convalescent sera produced group B flavivirus reaction and had a very low titre of antibody to JE in them, indicate their exposure to JE elsewhere in the remote past (Table 4). The activity of JE in this district has already been established [36]. So on the basis of the house hold condition, epidemiological information, detection of IgM antibody to Dengue virus in the acute sera and rise of dengue antibody titre in the convalescent sera confirms the etiologic agent of the febrile illness was dengue virus. It is worthy to mention that the selected acute sere/samples did not produce CPE in the tissue culture system and no virus could be isolated due to the fact that, the initiation of antibody (IgM) response mounted the activity of the virus during the course of infection at the late stage. On the other hand, samples might have lost the viability of the Dengue virus during transport and repeated freeze thawing conditions, as this may led to lose of viral titre or RNA, making it difficult to isolate the virus from the selected samples.
This scenario on the outbreak of dengue in three years at intervals, in the district of West Midnapore, happens to be the same as it has taken places in different cities in India. More over many of the ecological conditions in this area do not differ substantially from those where the disease has been prevalent. However, Dengue infections have been recorded mainly from the urban areas of the countries, all over the world. Due to the rapid and increased urbanization, Dengue has spread all over the world only in the urban area. But the reports of DF and DHF from the rural area either absent or scanty. This is an important observation that DF and DHF have first emerged in the rural area as the major public health problem in the district of West Midnapore, West Bengal, India; that needs to be taken notice of. Hence, it constitutes a new report from a rural and costal district like West Midnapore, West Bengal; which needs continuous surveillance and molecular studies on the circulating serotypes and their genotypes for addressing the probabilities of DSS/DHF incidence in future.
Acknowledgements
The author expresses his sincere gratitude to all the staff members of ICMR Virus Unit, for their constant help and assistance to carry out the laboratory investigations and compilation of data. I also gratefully acknowledge the help I received from N.I.V, Pune for providing me the Elisa kit and antigen to carry out the work smoothly. The enthusiastic repeated help obtained from the staff members of the office of Chief Medical Officer of Health, Medical Officers and Medical Technologists of the District Hospital, Sub divisional hospital and the primary health center at different places in the District West Midnapore during the investigations, is gratefully acknowledged.
Fundings
We received all sorts of financial help from the Indian Council of Medical Research, New Delhi, India to carry out the work in the ICMR VIRUS UNIT, KOLKATA, INDIA.
Competing interests
The first two authors are Research Fellows at the ICMR Virus Unit and the communicating author is an Assistant Research Officer of ICMR Virus Unit. The authors have no financial and competing interests that are affected by the material in the manuscript.
269
References
- MonathTP (1994) Dengue: The risk to developed and developing countries. Proc. Natl, Acad. Sci. USA 91: 2395-2400.
- MacBride WJ, Bielefeldt-Ohmann H (2000) Dengue viral infections, pathogenesis and epidemiology. Microbes Infection 2: 1041-1050.
- HenchelEA, Putnak JR (1990) The Dengue viruses. Clin.Microbiol.Rev. 3: 376-96.
- Solomon T, Mallewa M (2001) Dengue and other emerging flaviviruses. J.Infection 42: 104-115.
- World Health Organization (1996) Dengue and Dengue Haemorrhagic Fever Fact sheet. 117. Available:https://www.who.int/csr/resources/publications/dengue/ Denguepublication/en/
- Balaya S, et al (1969) Investigation of an outbreak of dengue in Delhi in 1967. Indian J Med Res 57: 767-774.
- Rodrigues FM, PatankarMR, Banerjee K (1972) Etiology of the 1965 epidemic of febrile illness in Nagpur city, Maharashtra State, India. Bull WHO 46: 173-179.
- PadbidriVS, DandawateCN, Goverdhan MK (1973) An investigation of the etiology of the 1971 outbreak of febrile illness in Jaipur city, India. Indian J Med Res 61: 1737-1743.
- Karamchandani PV (1973) Study of 100 cases of dengue fever in Madras penitentiary. Indian Med Gazette 72: 532-534.
- Gregson A, Edelman R (2003) Dengue virus infection. Paediatr. Infect. Dis.J22 :179- 181.
- WHO (1997) Dengue hemorrhagic fever: Diagnosis, treatment and control 2nd edn. Geneva. Available:https://www.who.int/csr/resources/publications/dengue/itoviii.pdf
- Nimmannitya S (2003) Dengue and dengue hemorrhagic fever. In: Cook GC, Zumla AL, editors. Manson’s Tropical Diseases, 21st ed. Philadelphia, USA: Saunders. pp. 765-772.
- AikatBK, Konar NR, Banerjee G (1964) Hemorrhagic fever in the Calcutta area. Indian J. Med. Res 152: 660-675.
- SarkarJK, Chakraborty SK, SarkarRK (1972) Sporadic cases of hemorrhagic and/ or shock during dengue epidemics. Trans. Royal Soc. Trop. Med. Hyg. 66: 875-877.
- GhoshSN, Pavri KM, Singh KRP (1974) Investigation on the outbreak of dengue fever in Ajmer city, Rajasthan state in 1969. Part-I.Epidemiological, clinical and virological study of the epidemic. Indian J. Med. Res. 62:511-522.
- ChauhanGS (1985) Clinical and virological study of dengue fever outbreak in Jalore city, Rajasthan. Ind J. Med .Res. 91:414-418.
- Seth P, Broor S, Dar L. Dengue outbreak in Delhi. In: Sharma PL., Sood OP, editors. Laboratory diagnosis.Ranbaxy Science Foundation, India. pp. 28-30.
- Carry DE, Myers RM, Pavri KM (1996) JE studies in Vellore, South India. Part—II.Antibody response to patients. Indian J. Med. Res. 56:1319-1329.
- Clark DH, Casals J (1958) Technique for Hemagglutination and Hemagglutination inhibition with arthropod borne viruses. Am. J. Trop. Med. Hyg. 7: 561-577.
- Broor S, et al (1997). Recent Dengue epidemic in Delhi, India. In: SaluzzoJF, Dodet B, eds. Factors in the emergence of arbovirus diseases. Amsterdam: Elsevier. pp. 123-127.
- PadbidiVS, MahadevPVM, Thakare JP (1996) Virological& entomological investigation of an outbreak of dengue fever in Dhuk district, Maharashtra. Indian J. Med Microbiol. 14: 25-32.
- Ram S, Khurana S, Kausshal V (1998) Incidence of dengue fever in relation to climatic factors in Ludhiana, Punjab. Indian J. Med. Res. 108: 128-133.
- Lanciotti RS, et al (1992) Rapid detection and typing of dengue viruses from clinical samples by using reverse transcriptase polymerase chain reaction. J. clin.Microbiol 30: 545-551.
- HenchelEA, et al (1991) Sensitivity and specificity of a universal primer set for the rapid diagnosis of dengue virus infections by polymerase chain reaction and nucleic acid hybridization. Am J Trop Med Hyg 45: 418-428.
- Carey DE, Myers RM, Reuben R (1964) Dengue types 1 and 4 viruses in wild- caught mosquitoes in south India. Science 143:131-132.
- Myers RM, et al (1964) The isolation of type 4 virus from human sera in south India. Indian J Med. Res 52 : 559-565.
- Myers RM, et al (1970) Dengue outbreak in Vellore, southern India, in 1968, with isolation of four dengue types from man and mosquitoes. Indian J Med. R 58: 24-30.
- Kaur H, et al (1997) Dengue Haemorrhagic fever outbreak in October-November 1996 in Ludhiana, Punjab, India. Indian J Med. R 106:1-3.
- Agarwal R, et al (1999) A clinical study of the patients with dengue Haemorrhagic fever during the epidemic of 1996 at Lucknow, India. South East Asian J. Trop. Med. Public Health 30: 735-740.
- Kabilan L, et al (2003) Dengue disease spectrum among infants in the 2001 dengue epidemic in Chennai, Tamil Nadu, India. J. Clin. Microbiol41: 3919-3921.
- PadbidriVS, et al (1995) The 1993 epidemic of dengue fever in Mangalore, Karnataka state, India. South east Asian J. Trop. Med. Public Health 26: 699-704.
- Barua HC, Mahanta J (1996) Serological evidence of DEN-2 activity in Assam and Nagaland. J.Comm. Dis. 28: 56-58.
- Cherian T, et al (1994) An epidemic of dengue haemorrhagic fever & dengue shock syndrome in and around Vellore. Indian J Med Res 100: 51-56.
- Dar L, et al (1999) The first major outbreak of dengue haemorrhagic fever in Delhi, India. 40: 418-427.
- Kurukumbi M, et al (2001) Sero epidemiological and active surveillance of dengue fever/ dengue haemorrhagic fever in Delhi. Indian J Med Sci 55: 149-156.
- Chatterjee S, et al (2004) Sero surveillance for Japanese encephalitis in children in several districts of West Bengal, India. ActaPaediatr 93: 390-393.

