Dkhissi Y1, Bourakkadi Idrissi M1, Benabddallah SI2, El-Bouhaddouti H1, Benjelloun E1, Ousadden A1, Ait Taleb K1 and Mouqit O1
1Department of Visceral Surgery A, Hassan II University Hospital, Fez, Morocco
2Department of Radiology, Hassan II University Hospital, Fez, Morocco
- Corresponding Author:
- Dkhissi Yassine
Department of Visceral Surgery A
Hassan II University Hospital, Fez, Morocco
Tel: 2120619513432
E-mail: yassine.dkhissi@usmba.ac.ma
Received Date: April 23, 2021; Accepted Date: May 25, 2021; Published Date: June 02, 2021
Citation: Dkhissi Y, Bourakkadi Idrissi M, Benabddallah SI, El-Bouhaddouti H, Benjelloun E, et al. (2021) Jejunal Diverticulosis Perforation: A Rare Cause of Acute Abdomen. J Univer Surg Vol. 9 No. 5: 26
Copyright: © 2021 Dkhissi Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Introduction: Small bowel diverticulosis is a rare pathology; in contrast to
colonic diverticular disease. It usually remains asymptomatic and undiscovered,
until severe complications such as diverticulitis or even perforation occurs. We
present a rare cause of acute abdominal pain with a case of jejunal diverticulitis
complicated with perforation.
Case report: We report the case of an 84-year-old woman, who was admitted
to the emergency department for the management of jejunal diverticulitis with
perforation, who underwent immediate surgery after confirmation on abdominal
CT-scan.
Conclusion: Jejunal diverticulitisis a rare entity that may lead to chronic non-specific
abdominal symptoms. However, it can also present as an acute complication, one
of its form being intestinal perforation, which may require immediate surgical
intervention.
Keywords
Jejunal diverticulitis; Perforation; Intestinal resection
Introduction
Jejunal diverticula represent 1% of digestive diverticular disease, and the jejunum is the least frequent location. Jejunal diverticulitisis usually not suspected clinically as symptoms are often vague and nonspecific (chronic abdominal pain and/ or malabsorption) [1], and can present complications such as bleeding, perforation and intestinal obstruction, which require urgent surgical treatment.
Case Report
We report the case of an 84-year-old woman, admitted on 15/03/2020, who complains from a painful abdominal mass in the left flank, and constipation, she had noticed in the previous week. The patient had a significant medical history as she was treated for type 2 diabetes and ischemic heart failure. No known history of colonic diverticulosis or any previous surgery. On physical examination the patient was febrile, and the abdominal examination revealed a round, tender, elastic mass in the left flank, measuring approximately 10 × 5 cm, with associated tenderness, but without rebound tenderness or other signs of peritonitis. CT scan of the abdomen and pelvis 15/03/2020 revealed a thinwalled, cavitated lesion with an air-fluid level in the left flank, limited by thickened small bowel loops and apparently with luminal continuity with at least one segment. There was no evidence of intraperitoneal free air or fluid (Figure 1).
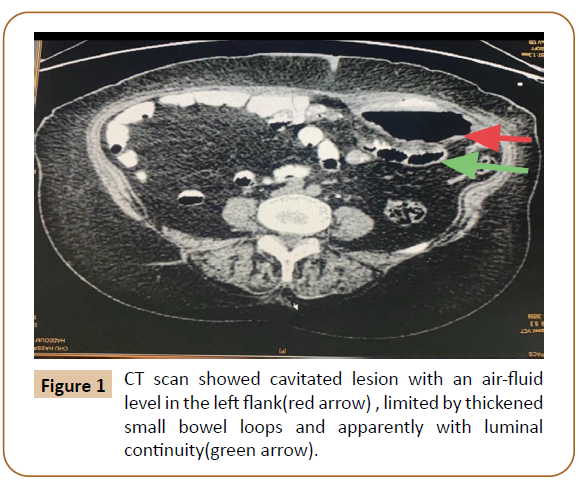
Figure 1: CT scan showed cavitated lesion with an air-fluid level in the left flank(red arrow) , limited by thickened small bowel loops and apparently with luminal continuity(green arrow).
The patient underwent a laparotomy which macroscopically revealed the diagnosis of perforated Jejunal diverticula. Multiple Jejunal diverticula were revealed, of which at least one was perforated. A segmental (20 cm) resection of the affected jejunum was carried out with evacuation of the parietal abscess, followed by a side-to-side hand-sewn primary anastomosis (Figure 2). The post-operative period was simple, and the patient was discharged on 23/03/2020.
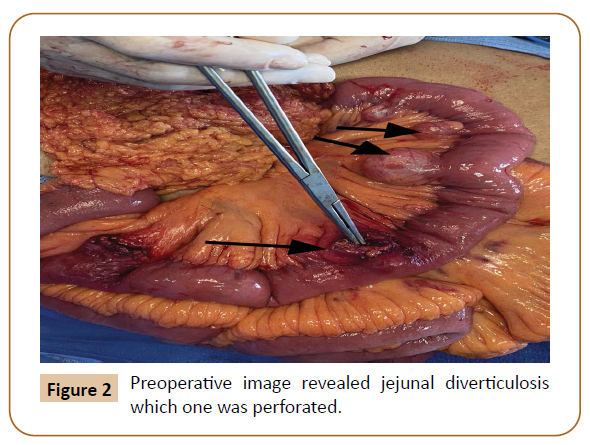
Figure 2: Preoperative image revealed jejunal diverticulosis which one was perforated.
Discussion
Jejunal diverticula are pseudo diverticula resulting from a mucosal and submucosal herniation through the muscular layer where blood vessel penetrates bowel’s wall. Small bowel diverticulosis was first described by Baillie and von Soemmerring in 1794 and Cooper first described jejunal diverticulosis in 1807 [2]. The hypothesis of jejunal diverticula is unknown; this condition is believed to develop from a combination of intestinal motility disorders, focal weakness of the muscularis and high segmental intra-luminal pressures, with diverticulum arising atthe site where mesenteric vessels enter into the muscular layer of the small intestine [3,4]. The diagnosis of a perforated diverticulum is rarely made preoperatively. Typical symptoms are sudden onset of abdominal pain, nausea, and vomiting. Typical physical findings are localized tenderness and rebound tenderness. The most frequent complications reported are malabsorption, obstruction, abscess formation, and rarely, diverticular perforation or hemorrhage (Acute complications occur in 10% - 20% of patients). However, the perforation of Jejunal Diverticula remains rare (2.1 to 7% of diverticulitis) [5].
In the emergency, abdominal CT is the better modality to diagnose this pathology and its complications, with findings that include thickening or inflammation of the jejunum and mesentery, localized abscess formation, air-fluid collection in contiguity with Small Bowel loops, free peritoneal air, and occasionally visualization of the diverticulum [6,7].
The presence of an acute complication may require immediate surgical intervention. Surgery is mandatory for intestinal resection (taking away perforated diverticulum) in 2 situations: failure or infeasibility of percutaneous drainage and generalized peritonitis. Immediate anastomosis should be performed whenever allowed by abdominal and general condition of the patient [8] like in our case. Otherwise, jejunostomy seems reasonable in shocked or high-risk patient.
Conclusion
Perforated jejunal diverticulitis is a rare clinical entity in which clinical presentation is variable; therefore, diagnosis is not necessarily easy. Surgical treatment is required for the management of complications; surgical resection followed by primary anastomosis is the treatment of choice.
37542
References
- Palder SB, Frey CB (1988) Jejunal diverticulosis. Arch Surg 123: 889-894.
- Kwak JY, Park EH, Park CS, Kim JH, Han MS, et al. (2016) Uncomplicated jejunal diverticulosis with pneumoperitoneum. Ann Surg Treat Res. 90: 346.
- Kassir R, Boueil-Bourlier A, Baccot S, Abboud K, Dubois J, et al. (2015) Jejuno–ileal diverticulitis: Etiopathogenicity, diagnosis and management. Int J Surg Case Rep 10: 151-153.
- Kongara KR, Soffer EE (2000) Intestinal motility in small bowel diverticulosis: a case report and review of the literature. J Clin Gastroenterol 30: 84-86.
- Benya EC, Ghahremani GG, Brosnan JJ (1991) Diverticulitis of the jejunum: Clinical and radiological features. Gastrointest radiol 16: 24-28.
- Mansoori B, Delaney CP, Willis JE, Paspulati RM, Ros PR, et al. (2016) Magnetic resonance enterography/enteroclysis in acquired small bowel diverticulitis and small bowel diverticulosis. Eur Radiol 26:n2881-2891.
- De Peuter B, Box I, Vanheste R, Dymarkowski S (2009) Smallbowel diverticulosis: imaging findings and review of three cases. Gastroenterol Res Pract.
- Kassahun WT, Fangmann J, Harms J, Bartels M, Hauss J (2007) Complicated small-bowel diverticulosis: a case report and review of the literature. World J Gastroenterol 13: 2240.

