Keywords
Fracture; Pelvic Bones; Injuries
Introduction
The trauma, a world public health problem, has been a major cause of morbidity and mortality, as it affects more than 50 million people today, an aggravated circumstance in urban centers, mainly due to the growing number of vehicles and the aggressiveness in traffic Which cause accidents with high energy and leading to an increase in the number of deaths and injuries [1].
Among the orthopedic traumas, pelvic injuries are considered the third cause of death due to auto accidents; represent 20% to 25% of fractures in polytraumatized patients, their incidence ranges from 3% to 8% of all skeletal fractures [2]. It is observed that up to 60% of the deaths occur in the area of the accident itself and about 90% of the cases, there are concomitant lesions, which represents a negative prognostic factor in relation to morbidity and mortality [3].
It is believed that retroperitoneal hemorrhage associated with pelvic fracture is responsible for 7% to 33% of deaths. When there is an association of complex fractures and serious injuries in other body segments, such as the skull and abdomen, the lethality can reach 50% [4].
Pelvic fractures, marked by mechanical instability, hemodynamics and presence of injuries in other body segments, are most often the result of strong impact traumas, especially in young people, such as falls from high altitude and auto accidents [2], requiring a frontal collision at least 50 km/h or lateral at 40 km/h to damage the pelvic ring. In about 72% of cases, injuries occur in compact vehicles, which are increasingly common in urban centers [5].
Differently from what occurs in the elderly, where this type of injury in general is caused by low energy trauma, more commonly falling from the height itself, mainly due to bone porosity [2].
Patients with pelvic fracture have several associated severe lesions, especially involving the extremities, brain, urogenital and abdominal regions. These have higher mortality and the survivors have a high chance of living with some permanent sequel. For this reason, the simple presence of a pelvic fracture indicates a severe trauma, with a greater chance of developing complications and death [5].
Fractures of the pelvic ring are part of the routine of traumatology. The accompanying traumatic lesions commonly require neurosurgeries, abdominal surgeries, colostomies, cystostomies, drains and prolonged hospitalization that impair orthopedic treatment. When assessing a patient with pelvic trauma, one should keep in mind the momentary conditions related to the general condition of the patient and their clinical conditions, since vessels, nerves and organs are in close contact with the bone structure and are prone to suffering associated lesions [6].
Advances in pre-hospital care, accompanied by the improvement of the multidisciplinary approach to those traumatized with pelvic fractures, are responsible for the reduction of morbidity and mortality observed in recent years. Rapid intervention in the control of retroperitoneal hemorrhage through early external fixation and angiography with embolization, associated with the development of transfusion protocols and damage control are some of the most important aspects in the care of these patients [7].
With this, it is observed that deaths caused by retroperitoneal hemorrhage alone have become less common and that many deaths are caused by concomitant lesions, especially craniophalic trauma. This is true especially in patients with stable pelvic fractures [7].
To understand the changes in the behavior of the population in the last decades, regarding pelvic fracture, have been widely discussed by hospital and educational institutions, governments and the population in general to the morbidity and mortality resulting from this trauma. In this way, this study proposes to review in the scientific literature the main lesions associated with pelvic fractures.
Methods
It is an integrative review of the literature, a specific method that summarizes empirical or theoretical literatures to provide a more comprehensive understanding of a particular phenomenon with the potential to present the state of science, contribute to the development of theory, and have direct applicability to practice and policy [8].
The methodological process carefully followed the following steps: selection of the hypotheses or questions for the review; establishment of sample selection criteria; categorization of studies and synthesis of knowledge produced; analysis of data and results; and interpretation of the results, which provided a critical examination of the findings [9].
Considering the criteria proposed by an integrative review, the study intends to answer the question: What are the injuries associated with pelvic fractures found in scientific literature?
The inclusion criteria adopted for the search and selection of publications were: articles published in national and international scientific journals that approached the theme: morbidity of lesions associated with pelvic fracture; disclosed in portuguese, english or spanish; in the period from 2006 to 2016; indexed in databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Literatura Latino-Americana e do Caribe em Ciências da Saúde (LILACS), Scientific Electronic Library Online (SCIELO) e Índice Bibliográfico Espanhol de Ciências da Saúde (IBECS); Made available in full, either directly from the base website or through the Capes Portal; via the combination of the following descriptors registered in the Portal de Descritores das Ciências da Saúde (DeCS) ou no Medical Subject Headings (MeSH): “fraturas”, “ossos da pelve” e “lesões”, These descriptors were combined with the boolean operator and in order to refine the studies according to the theme addressed.
The search was carried out in an orderly manner, with a classification in the first analysis of articles in the categories: outside the period considered, does not provide the full text, published in more than one database, duplicates, and then were selected for second analysis. Subsequently, a careful reading of the title and summary of each publication was carried out in order to verify the consonance with the guiding question of the investigation. In the presence of doubt as to the criteria of inclusion or exclusion, it was read in its entirety, in order to reduce the risk of loss of publications. Thus, those who did not approach the theme in full were discarded in the second analysis.
Data collection took place in January and February of 2017 and was supported by an instrument written by the authors with the help of Microsoft Office Excel 2010 software, and included the following variables: article title, authors, periodical, year of publication, Country of study, study type/approach. The search initially found 748 articles, after the first analysis was 164 and at the end, the sample was composed of 19 articles (Figure 1).
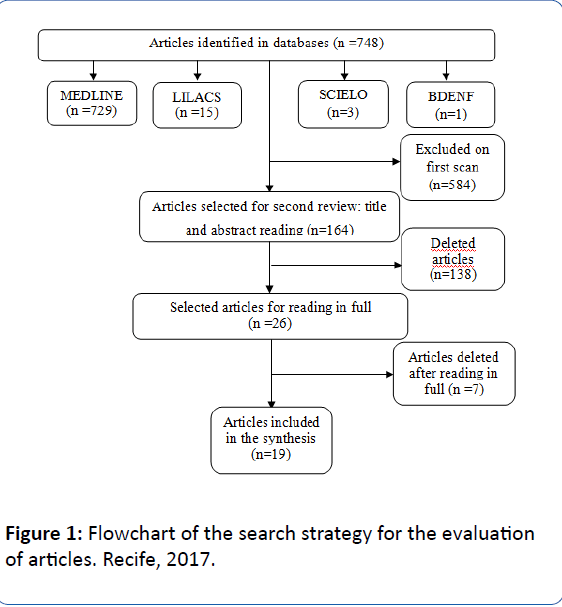
Figure 1: Flowchart of the search strategy for the evaluation of articles. Recife, 2017.
Results and Discussion
In the present study, 19 articles were analyzed in their entirety. After analyzing the selected articles, according to Table 1, productions of six continents were raised: Europe (7/19) [9-15], North America (6/19) [16-21], Africa (3/19) [22-24], Asia (1/19) [25], Oceania (1/19) [26], and South America (1/19) [27], with predominance in the following countries: United States (5/19) [16-21], Egypt (3/19) [22-24] and United Kingdom (3/19) [12-14]. In Brazil, the Southeast Region was the only one that presented a publication being represented by the State of São Paulo. It is noteworthy that no studies were found in Central America that dealt with the subject matter.
| Ref |
Article title |
Authors |
Journal |
Country/Year |
Type of research |
| [9] |
One-year outcome of geriatric Hip-fracture patients following prolonged ICU treatment |
Eschbach D, Bliemel C, Oberkircher L, Aigner R, Hack J, Bockmann B, Ruchholtz S, Buecking B. |
BioMed Research International |
Germany/2016 |
Prospective observational study |
| [10] |
Analysis of the cause, classification, treatment, outcome and associated injuries of pediatric pelvic ring fractures |
Saglam Y, Dikmen G, Bademler S, Aksoy M, Dikici F. |
Ulus Travma Acil Cerrahi Derg |
Turkey/
2015 |
Retrospective study |
| [11] |
Which pelvic ring fractures are potentially lethal? |
Ruatti S, Guillot S, Brun J, Thony F, Bouzat P, Payen JF, Tonetti J. |
Injury Int J Care Injured |
France/
2015 |
Retrospective study |
| [12] |
Admission for osteoporotic pelvic fractures and predictors of length of hospital stay, mortality and loss of independence |
Marrinan S, Pearce MS, Jiang XY, Waters S, Shanshal Y. |
Age and ageing |
United Kingdom/
2014 |
Prospective study |
| [13] |
High rates of sexual and urinary dysfunction after surgically treated displaced pelvic ring injuries |
Odutola AA, Sabri O, Halliday R, Chesser TJS, Ward AJ. |
Clin Orthop Relat Res |
United Kingdom/
2012 |
Prospective study |
| [14] |
Paediatric pelvic ring fractures and associated injuries |
Leonard M, Ibrahim M, Mckenna P, Boran S, McCormack D. |
Injury Int J CareInjured |
United Kingdom/011 |
Retrospective study |
| [15] |
Fracturas de pelvis graves, lesiones associadas e inestabilidad hemodinámica: incidencia, manejo y pronóstico em nuestro medio |
Tocino JMS, Fuentes FT, Díaz DP, Sánchez MS, Oliver JL, Ortúzar JO, Baena DM. |
Cir Esp |
Spain/
2007 |
Retrospective study |
| [17] |
Can we ever stop worrying about venous thromboembolism after trauma? |
Godat LN, Leslie K, Chang, David CC, Coimbra R. |
Journal of Trauma and Acute Care Surgery–2015 |
United States/
2015 |
Retrospective study |
| [18] |
The effect of pelvic factures on future stress incontinence and pelvic organ prolapse surgery |
Welk B, Hothi HA, Winick NJ,
Chou Q, MacMillan B, Lawendy AR. |
Int Uro gynecol |
Canada/
2015 |
Retrospective study |
| [19] |
Obesity increases early complications after high-energy pelvic and acetabular fractures |
Morris BJ, Richards JE, Guillamondegui OS, Sweeney KR, Mir HR, Obremskey WT, Kregor PJ. |
Journal of Orthopaedic Trauma |
United States/
2015 |
Retrospective study |
| [20] |
Pelvic ring injury is associated with sexual dysfunction in women |
Vallier HÁ, Cureton BA, Schubeck D. |
Journal of Orthopaedic Trauma |
United States/
2012 |
Prospective study |
| [21] |
Genitourinary injuries in pelvic fracture morbidity and mortality using the National Trauma Data bank |
Bjurlin MA, Fantus RJ, Mellett MM, Goble SM. |
Journal of Trauma Injury Infection & Critical Care |
United States/
2009 |
Retrospective study |
| [23] |
Predicting risk of erectile dysfunction after pelvic fracture urethral injury in children |
Koraitim MM. |
The Journal of Urology |
Egypt/
2014 |
Prospective study |
| [24] |
Predictors of erectile dysfunction post pelvic fracture urethral injuries: A multivariate analysis |
Koraitim MM. |
Urology |
Egypt/
2013 |
Prospective study |
| [25] |
Epidemiology of hospitalized traumatic pelvic fractures and their combined injuries in Taiwan: 2000-2011 National Health Insurance Data Surveillance |
Yang NP, Chan CL, Chu D, Lin YZ, Lin KB, Yu CS, Yu IL, Chang NT, Lee YH. |
Bio Med Research International |
Taiwan/
2014 |
Retrospective study |
| [26] |
Functional and return to work outcomes following major trauma involving severe pelvic ring fracture |
Gabbe BJ, Hofstee DJ, Esser M, Bucknill A, Russ MK, Cameron PA, Handleyand C, Steiger RN. |
ANZ journal of surger |
Australia/
2014 |
Observational study with prospective and retrospective data |
| [27] |
Fratura de pelve: um marcador de gravidade em trauma |
Filho RMC, Parreira JG, Perlingeiro JAG, Soldá SC, Campos T, Assef C. |
Rev Col Bras Cir |
Brazil/
2011 |
Retrospective study |
Table 1: Characteristics of the articles included in the integrative review, according to reference, title, authors, published periodicals, country, year and type of research. Recife, PE, Brazil, 2017.
Classifying the articles according to the year of publication, there was predominance in the year 2015 (6/19) [11-16], followed by 2014 (4/19) [17-20]. As for the methodological design of the researches, 12 articles were about retrospective studies [10-16,18,24-27], carried out from past records, and it is followed from that moment to the present [28].
High velocity pelvic ring fractures are life-threatening lesions and various lesions are described associated with pelvic fractures. For purposes of analysis, the results were grouped into categories, namely: abdominal lesions, thoracic lesions, lesions of long and cranial and hematological bones. Table 2 presents the synthesis of the main results of the selected studies, addressing the main lesions associated with pelvic fractures.
| Ref* |
Major injuries associated with pelvic trauma |
| [09] |
Respiratory and renal insufficiency and urinary tract infection |
| [10] |
Cranial and long bone lesions, maxillary-facial fracture, rib fractures, pulmonary contusions, pneumothorax, lesions in solid abdominal organs, genitourinary lesions, perineal lacerations and intramuscular hematomas |
| [11] |
Massive bleeding |
| [12] |
Urinary tract and respiratory tract infections |
| [13] |
Erectile and urinary dysfunction |
| [14] |
Cranial and rib fractures, splenic and hepatic lacerations, soft tissue and parenchymal brain injury, extensive facial hemorrhage, pneumothorax, hemothorax, rupture of the diaphragm, bladder and urethral ruptures, perineal, pelvic and intramuscular hematoma and large abdominal contusions |
| [15] |
Rib fractures, pneumothorax, long bones, lesions in the liver, spleen and bladder, cranial and spinal ruptures |
| [16] |
Lesion of the sacral, urinary and bladder |
| [17] |
Venous thromboembolism |
| [18] |
Urinary dysfunction and pelvic organ prolapse |
| [19] |
Deep venous thrombosis, pulmonary embolism, pneumonia, and respiratory failure |
| [20] |
Dyspareunia and less interest in sexual intercourse |
| [21] |
Cranial injuries, genitourinary injury, lower extremity, thoracic and abdominal |
| [22] |
Traumatic urethral stenosis and erectile dysfunction |
| [23] |
Erectile dysfunction |
| [24] |
Erectile dysfunction |
| [25] |
Fractures of upper and lower limbs, spine and skull, internal injury of the abdomen, pelvis and thorax |
| [26] |
Thoracic, abdominal, upper and cranial, urological, neurological, urinary tract and vascular complications |
| [27] |
Traumatic subdural hemorrhage, spinal trauma, hemothorax, pneumothorax, rib fractures, pulmonary contusion, spleen, liver, renal and bladder injuries |
Table 2: Synthesis of the main results of the articles of the present integrative review, Recife, PE, Brazil, 2017.
Several complications were observed in the abdominal region, among them: urinary dysfunction [10,12-14,16,18,21,26], bladder injuries [10,14,15,27], erectile dysfunction [22-24,13], unilateral infection [9,12,26], uterine stenosis [22], dyspareunia [22], perineal hematoma [14], renal failure [9], lesions in parent organs [19].
The rupture of the high energy pelvic ring can have a significant impact on the genitourinary system, with some patients having a direct lesion concomitant with the urethra or bladder. Although direct damage to these organs is often identified at the time of injury, long-term sequelae of substantial rupture to the internal pelvic floor support systems may not present for years [24].
These predictive fractures of the genitourinary lesions are mainly those associated with anterior pubic arch rupture, including pubic symphysis diastasis, dislocated lower pubic branch fracture, bilateral pubic branch fractures, combined pubic and sacroiliac fractures, or rupture of the sacroiliac joint [23].
The underlying causes of sexual dysfunction following pelvic trauma are related to damage to autonomic nervous, vascular or erectile tissues. Delays in the evaluation and treatment of erectile dysfunction may result in irreversible morphological and functional changes in the erectile tissue and veno-occlusive mechanism with less satisfactory results [23].
Sexual dysfunction was analyzed in a prospective study [14], the results pointed to erectile dysfunction after pelvic fracture had a vasculogenic etiology in 84% of the patients, could be sub classified as arteriogenic in 76% and arteriovenogenic in 8%. Two other studies [16,23] verified the causes of erectile dysfunction in children after pelvic fracture urethral injuries, two factors, length of urethral clearance and lateral displacement of the prostate, stand out as independent predictors for the development of erectile dysfunction at puberty.
In another study [24] it was observed that the most common complaints were reduced excitement or less sexual desire, with erectile dysfunction reported in 20% of men and pain in 3% of women. There is a correlation between the subjective severity reported by the patient of sexual and urinary dysfunction, sustaining the view that psychological and emotional issues may also be important.
Regarding the chest region, thoracic complications related to pelvis fracture, verified in nine articles were: rib fracture [1,11,18,22], pulmonary contusion [1,5,18,22], pneumothorax [1,5,18,22], spinal cord injuries [7,11,22], rupture of the diaphragm [5], hemothorax [13,25]. As in other studies [29] and [30], thoracic trauma resulting from pelvic fracture is common and, among them, rib fractures accompanied by pneumothorax and pulmonary contusion are often associated with abdominal injuries, with the liver often the spleen.
In a retrospective study carried out in Brazil [27], the organs most affected were the thoracic/abdominal/pelvic organs, among them the bladder, spleen, liver, urethra and kidneys. Data corroborated with the results of another study carried out in Germany [31], which analyzed 386 trauma victims with pelvic fractures, found the following changes: retroperitoneal hematoma, bladder, urethral, bilateral or bilateral sacral plexus vessels pelvic, intestine and perineum.
Bone lesions, including upper and lower limb fractures [17,15,26,28], cranial fractures [17,23,21,28] and lesion of the sacral spine [10] were verified in seven of the analyzed articles. In a retrospective study conducted in Turkey [10], all patients had end-injury, cranial and long-bone lesions (forearm, femur and tibia) were reported in nine cases.
Distal femoral fractures are more common in cases of injuries associated with pelvic trauma, particularly in elderly individuals. These fractures are the result of a single or multiple overloads, with a magnitude exceeding the limit supported by the bone. Treatment should be done so that the reduction is anatomical or at most with the distal segment slightly in the cranial position [31].
The main complication of these fractures is joint stiffness, which can be quite disabling for many activities of the lower and upper limbs. In addition, there may be severe damage to soft tissues, which can affect muscles, blood vessels and nerves [32].
The facial skin and the facial bones, due to their anterior projection corporal, can be exposed to these aggressions. The skin has thin and elastic thickness, the subcutaneous tissue is thin, the musculature is superficial and vascularization and innervation are extensive. Soft tissues, when compressed between bones and external aggression forces, can have numerous lesions (cuts, lacerations, hemorrhages, hematomas, etc.), potentializing the deleterious effects of bone fractures [33].
The cranial fracture can be closed or exposed, and may have the potential to damage veins involving the brain and the bleeding caused, when very intense, causes brain lesions that may be irreversible. Another complication of cranial fractures are infections, since bacteria can invade the brain, causing infections and severe brain injuries [34].
Concerning hematologic complications associated with femoral fracture, thromboembolism [17], deep vein thrombosis [19] and hemorrhage [11,14] are prominent.
The rates of deep venous thrombosis (VTE) among the general population are low, ranging from 0.1% to 0.2% per year. In contrast, trauma patients are at high risk for developing VTE, with rates ranging from 58% to 67% when chemical prophylaxis is not used [35].
Patients such as vertebral and pelvic fractures are among those with a higher known risk of developing thrombosis. A retrospective study in the California State Hospital database [17] found that the period of highest risk for VTE occurred in the first three months and that VTE risk returned consistently to that of the general population of 12 months to 15 months after injury.
Intra-pelvic, venous or arterial hemorrhage, associated with other thoracic, abdominal and cranial lesions, explains the high mortality rates in polytraumatized patients with pelvic ring fractures. The recent development of endovascular techniques for the control of intra-pelvic arterial bleeding allows us to quantify and map vascular lesions and effectively treat hemorrhage [36,37].
In the case of anterior pelvic ring lesions, the middle artery is often damaged, especially with pubic symphysis dysfunction. Moreover, in most cases, a >3 cm gap is associated with a complete posterior lesion, which is exposed to bleeding from the posterior part of the pelvic ring, requiring most of the time the patients are embolized. Lesions of the anterior pelvic ring may lead to retroperitoneal hematoma, which may explain the need for embolization in many cases [11].
A retrospective study of the files of patients from a University Hospital in France [11] identified as potentially lethal pelvic fractures: iliac wing fractures and sacral fractures. Patients with complete posterior injury and dysfunction of the pubic symphysis are unstable and associated with hemodynamic collapse because bleeding cannot be contained due to complete disruption of the pelvic ring.
The primary identification should allow to anticipate massive hemorrhages and transport these patients directly to a Trauma Center with interventional radiology and possibility of embolization [11]. Since retroperitoneal hemorrhage associated with pelvic fracture accounts for 7% to 33% of deaths [4].
When assessing a patient with pelvic trauma, one should keep in mind the momentary conditions related to the general condition of the patient and their clinical conditions, since vessels, nerves and organs are in close contact with the bone structure and are prone to suffering associated lesions [6].
The presence of a pelvic fracture can be considered as a marker of severity in trauma. It’s simple diagnosis impels to investigate, actively, associated lesions, presumed the presence of retroperitoneal bleeding and, before hemodynamic instability, to take immediate measures for the transfusion of hemoderivatives, identification of hemorrhagic focus and its control [27].
Conclusion
Many are the lesions associated with the fractures of the pelvic ring, especially the abdominal and thoracic regions, the long bones, the skull and the hematological ones. The organs most affected were the bladder, spleen, liver, rib, urethra and kidneys. This study made it possible to size and analyzes the production of the injuries associated with pelvic fractures. In this context, we emphasize the need for studies that also emphasize the care of these patients through humanized care, in order to minimize the physical discomforts and social, psychic and emotional problems that can be generated by these injuries.
It is hoped that this study may contribute to professionals and other research, as it provides knowledge of the major injuries associated with pelvic trauma. This study, coupled with an action plan, contributes as a tool to build a care plan to be implemented from admission to preparation for discharge, including guidelines for home care.
19454
References
- Gaudêncio TG, Leão GML (2013) The epidemiology of traumatic brain injury: A bibliographical survey in Brazil. Rev Neurocienc. 21: 427-434.
- Pizanis A, Pohlemann T, Burkhardt M, Aghayev E, Holstein JH (2013) Emergency stabilization of the pelvic ring: Clinical comparison between three different techniques. Injury 44: 1760-1764.
- Holstein JH, Culemann U, Pohlemann T (2012) What are predictors of mortality in patients with pelvic fractures? Clin Orthop Relat Res 470: 2090-2097.
- Parreira JG, Kanamori LR, Valinoto GC, Perlingeiro JAG, Soldá SC, et al. (2014) Comparative analysis between identified injuries of victims of fall from height and other mechanisms of closed trauma. Rev Col Bras Cir 41: 285-291.
- Sarraf EM (2013) Clinical and epidemiological profile of patients with hip fracture in a traumatological reference hospital in the city of Salvador, Bahia. Revista Baiana de Saúde Pública 36: 1053.
- Guimarães RP, Ribeiro AG, Ulson O, Ávila RB, Ono NK, et al. (2016) Treatment of unstable pelvic ring lesions with supra-acetabular fixator and sacroiliac screws: Preliminary results in 20 patients. Rev Bras ortop 51: 132-137.
- Cordts Filho RM, Parreira JG, Perlingeiro JAG, Soldá SC, Campos T, et al. (2011) Pelvis fracture: A marker of severity in trauma. Rev Col Bras Cir 38: 310-316.
- Soares CB, Hoga LAK, Peduzz M, Sangaleti C, Yonekura T, et al. (2014) Integrative review: Concepts and methods used in nursing. Rev Esc Enferm USP 48: 335-345.
- Eschbach D, Bliemel C, Oberkircher L, Aigner R, Hack J, et al. (2016) One-year outcome of geriatric hip-fracture patients following prolonged ICU treatment. BioMed Res Int 1: 1-6.
- Saglam Y, Dikmen G, Bademler S, Aksoy M, Dikici F (2015) Analysis of the cause, classification, treatment, outcome and associated injuries of pediatric pelvic ring fractures. Ulus Travma Acil Cerrahi Derg 21: 392-396.
- Ruatti S, Guillot S, Brun J, Thony F, Bouzat P, et al. (2015) Which pelvic ring fractures are potentially lethal? Int J Care Injured 46: 1059-1063.
- Marrinan S, Pearce MS, Jiang XY, Waters S, Shanshal Y (2015) Admission for osteoporotic pelvic fractures and predictors of length of hospital stay, mortality and loss of independence. Age Ageing 44: 258-261.
- Odutola AA, Sabri O, Halliday R, Chesser TJS, Ward AJ (2012) High rates of sexual and urinary dysfunction after surgically treated displaced pelvic ring injuries. Clin Orthop Relat Res 470: 2173-2184.
- Leonard M, Ibrahim M, Mckenna P, Boran S, McCormack D (2011) Paediatric pelvic ring fractures and associated injuries. Injury Int J Care Injured 42: 1027-1030.
- Tocino JMS, Fuentes FT, Díaz DP, Sánchez MS, Oliver JL, et al. (2007) Severe pelvic fractures, associated injuries and hemodynamic instability: Incidence, management and prognosis in our environment. Cir Esp 81: 316-323.
- Delaney KM, Reddy SH, Dayama A, Stone MEJ, Meltzer JA (2016) Risk factors associated with bladder and urethral injuries in female children with pelvic fractures: An analysisof the National Trauma Data Bank. J Trauma Acute Care Surg 80: 472-476.
- Godat LN, Leslie K, Chang, David CC, Coimbra R (2015) Can we ever stop worrying about venous thromboembolism after trauma? Trauma Acute Care Surg 78: 475-481.
- Welk B, Hothi HA, Winick NJ, Chou Q, MacMillan B, et al. (2015) The effect of pelvic fractures on future stress incontinence and pelvic organ prolapse surgery. Int Uro gynecol 26: 805-811.
- Morris BJ, Richards JE, Guillamondegui OS, Sweeney KR, Mir HR, et al. (2015) Obesity increases early complications after high-energy pelvic and acetabular fractures. J Orthop Trauma 38: 881-887.
- Vallier HÁ, Cureton BA, Schubeck D (2012) Pelvic ring injury is associated with sexual dysfunction in women. J Orthop Trauma 26: 308-313.
- Bjurlin MA, Fantus RJ, Mellett MM, Goble SM (2009) Genitourinary injuries in pelvic fracture morbidity and mortality using the national trauma data bank. J Trauma 67: 1033-1039.
- Assmy AE, Harraz AM, Benhassan M, Fouda M, Gaber H, et al. (2015) Erectile dysfunction post‑perineal anastomotic urethroplasty for traumatic urethral injuries: Analysis of incidence and possibility of recovery. Int Urol Nephrol 47: 797-802.
- Koraitim MM (2014) Predicting risk of erectile dysfunction after pelvic fracture urethral injury in children. J Urol 192: 519-523.
- Koraitim MM (2013) Predictors of erectile dysfunction post pelvic fracture urethral injuries: A multivariate analysis. Urology 81: 1081-1085.
- Yang NP, Chan CL, Chu D, Lin YZ, Lin KB, et al. (2014) Epidemiology of hospitalized traumatic pelvic fractures and their combined injuries in Taiwan: 2000-2011 National Health Insurance Data Surveillance. BioMed Res Int 1: 1-9.
- Gabbe BJ, Hofstee DJ, Esser M, Bucknill A, Russ MK, et al. (2015) Functional and return to work outcomes following major trauma involving severe pelvic ring fracture. ANZ J Surg. 85: 749-754.
- Filho RMC, Parreira JG, Perlingeiro JAG, Soldá SC, Campos T, et al. (2011) Pelvis fracture: A marker of severity in trauma. Rev Col Bras Cir 38: 310-316.
- Hochman B, Nahas FX, Oliveira Filho RS, Ferreira LM (2005) Research Drawings. Acta Cir Bras 20: 2-9.
- Gurevitz S, Bender B, Tytiun Y, Velkes S, Salai M, et al. (2005) The role of pelvic fractures in the course of treatment and outcome of trauma patients. Isr Med Assoc J 7: 623-626.
- Dyer GS, Vrahas MS (2006) Review of the pathophysiology and acute management of haemorrhage in pelvic fracture. Injury 37: 602-613.
- Mourão AL, Vasconcellos HA (2001) Geometry of the proximal femur in Brazilian bones. Acta Fisiátrica 8: 113-119.
- Fernandes MGA, Fonseca EMM, Barbosa MP, Natal RM (2015) Biomechanical analysis of femoral diaphyseal fractures (type b) using an intramedullary nail. Revista Iberoamericana de Ingeniería Mecánica 19: 41-48.
- Maia BG, Paula FRP, Cotta GD, Costa MAL, Públio PG, et al. (2013) Clinical-epidemiological profile of trauma occurrences brain. Rev Neurocienc 21: 43-52.
- Jerônimo AS, Creôncio SCE, Cavalcanti D, Moura JC, Ramos RA, et al. (2014) Factors related to the prognosis of traumatic brain injury victims: a bibliographic review. Arq Bras Neurocir 33: 165-169.
- Centers for Disease Control and Prevention (2012) Deep vein thrombosis/pulmonary embolism blood clot forming in a vein: Data and statistics.
- Martinelli T, Thony F, Decle´ ty P, Sengel C, Broux C, et al. (2010) Intra-aortic balloon occlusion to salvage patients with life-threatening hemorrhagic shocks from pelvic fractures. J Trauma 68: 942-948.
- Sánchez-Tocino SJM, Turégano-Fuentes F, Pérez-Díaz D, Sanz-Sánchez M, Lago-Oliver J, et al. (2007) Severe pelvic fractures, associated injuries and hemodynamic instability: Incidence, management and prognosis in our medium. Cir Esp 81: 316-323.


