Introduction
Low back pain has clinical, social and economical importance since it is a public health problem that affects the population indiscriminately. The available literature is heterogeneous and contradictory.
It is unknown exactly what the proportion of affected people around the world is. Globally, it is estimated that 4-33% of the population exhibits it [1]. While in the United States (USA), Spain and Africa this ranges from 8% to 56% [2-4]. Recent data indicate that its incidence and prevalence have remained stable over the last 15 years [5]. However, the prevalence in the general population is rarely under study, compared with the prevalence in specific groups, like schoolchildren, adolescents, medical students, construction workers, nurses, farmers and indigenous people, to mention a few [6-14].
Most of the research has been developed in the field of occupational medicine, even over orthopedics, since industrialized societies are presenting an disability epidemic due to low back pain, with a tremendous socioeconomic and labor impact, that tend to increase [15]. In Mexico, Noriega-Elió et al. [16] stated that 10-15% of the disability reports in the Mexican Institute of Social Security (IMSS), are issued for low back pain.
Given the frequency of low back pain, attempts have been made to identify its etiology, and so far, approximately 57 causes have been pointed out [17]. However, there is no linear correlation between clinical and anatomic alterations, so an etiological diagnosis is only possible in 10-20% of the cases, i.e., 80-90% of low back pains were “non-specific” [18,19]. Therefore, approximately 90% are cared for and controlled by primary care [3].
Risk factors are numerous, varied and heterogeneous, amongst them are: prolonged static posture, heredity, old age, heavy labor, smoking, obesity, stress, low psychological well being, female gender, operating heavy machinery, exposure to intense vibrations, emotional and behavioral problems, abdominal pain, tiredness, odynophagia, rapid growth rate, tendon and quadriceps stiffness, study and work, previous episode of low back pain 12 months before current, age >25 years old,
Tall stature (≥1.80 m), overweight, construction work, nursing and office work, repetitive and monotonous, frequent twisted postures, driving vehicles daily, lifting and carrying heavy loads, work dissatisfaction, unemployment, and work in the field [2-32]. On the other hand, it has not always been able to corroborate the significant association of these factors with low back pain, so it is recommended to check in different populations.
In the IMSS in Tabasco, low back pain is one of the main reasons to request medical attention. In the Family Medicine Unit (UMF) No. 11 of the IMSS, Comalcalco, Tabasco, it’s one of the top 20 reasons for consultation in adults over 20 years old, and one of the 20 most common reasons for temporal disability [33-35].
Therefore, an investigation was conducted aimed at determining the prevalence of low back pain and its association with some known risk factors, in beneficiaries in the UMF No. 11 of the IMSS, Comalcalco,Tabasco, Mexico.
Materials and Methods
An analytic cross-sectional investigation was conducted, in which the universe of the study were beneficiaries of the UMF 11 of the IMSS, in Comalcalco, Tabasco, México, a finite and undetermined number, from which a multistage sample was taken: 1) Sub-universe of medical centers (6 units), random sample with maximum error acceptable 5%, estimated percentage of sample 10%, and p=0.05 obtaining 1 medical center, randomly selected by raffle method, “Medical Center No. 6”. 2) Sub-universe of 420 beneficiaries appointed to the selected medical center, probability sampling with maximum error acceptable 5%, estimated percentage of the sample 25%,and p=0.05, obtaining 100 beneficiaries, selected by nonprobability sampling by convenience. Selecting people >15 years old, of either sex, who went to receive medical and/or preventive attention in the selected location during September-December 2007; excluding: pregnant women, carriers of cognitive diseases, locomotive disabilities and/or musculoskeletal malformations, users of wheelchairs or crutches, and people with a history of spinal surgery.
Accepted after external review
Given the frequency of low back pain, attempts have been made to identify its etiology, and so far, approximately 57 causes have been pointed out [17]. However, there is no linear correlation between clinical and anatomic alterations, so an etiological diagnosis is only possible in 10-20% of the cases, i.e., 80-90% of low back pains were “non-specific” [18,19]. Therefore, approximately 90% are cared for and controlled by primary care [3].
Risk factors are numerous, varied and heterogeneous, amongst them are: prolonged static posture, heredity, old age, heavy labor, smoking, obesity, stress, low psychological well being, female gender, operating heavy machinery, exposure to intense vibrations, emotional and behavioral problems, abdominal pain, tiredness, odynophagia, rapid growth rate, tendon and quadriceps stiffness, study and work, previous episode of low back pain 12 months before current, age >25 years old,
Sociodemographic and anthropometric variables on lifestyles and unhealthy habits, chronic degenerative diseases and low back pain were studied. The information was gathered in an interpretive survey, filled in by direct examination (subject to signature of informed consent [of the parents / guardians in the case of minors under 18 years old]) and clinical record review.
The data were analyzed using the software Epi Info® v3.3.2 (freeware distributed by the USA Center of Disease Control and Prevention) in two phases: 1) Descriptive statistics to identify characteristics of the sample, and 2) Odds ratio (OR) with 95% confidence (p≤0.05) to identify factors associated with Low Back Pain. The research was conducted with prior approval of the Local Committee of Inquiry 2701 of the IMSS.
Results
Description of the population
100 beneficiaries, 57% male and 43% female were studied. The mean age was 32.5±12.49 years, mode 28, minimum 17, and maximum 76 years. The sociodemographic, lifestyle and health conditions of the population are shown in Table I, while the anthropometric characteristics are shown in Table II.
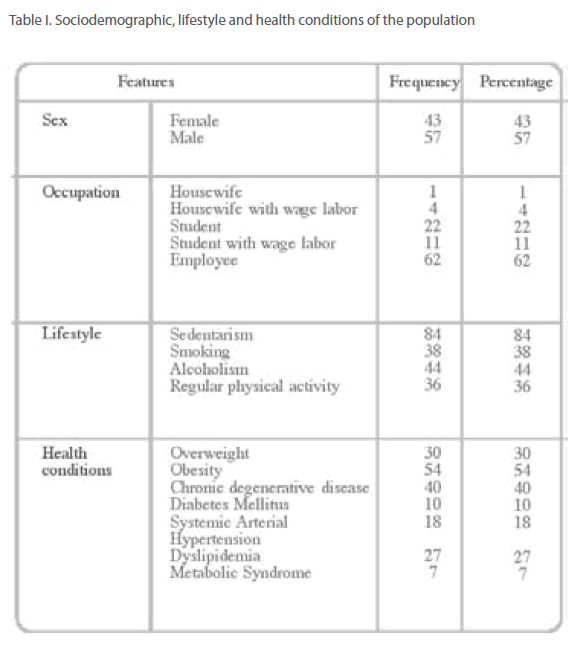
Table I: Sociodemographic, lifestyle and health conditions of the population
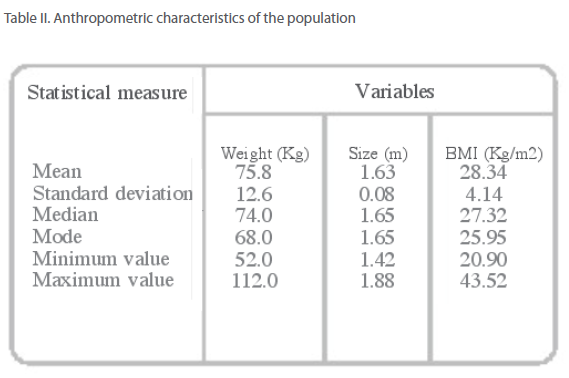
Table II: Anthropometric characteristics of the population
Prevalence of Low Back Pain
The prevalence of Low Back Pain was 63% of beneficiaries.
Factors associated with Low Back Pain
When looking for factors associated with Low Back Pain, it was found an association statistically significant with: student occupation, age >25 years, male gender, wage earning worker, obesity, sedentarism, smoking, alcoholism, chronic degenerative disease, Diabetes Mellitus, Systemic Arterial Hypertension, and Metabolic Syndrome (Table III). Table III. Odds Ratio: Independent Variables / Low back pain
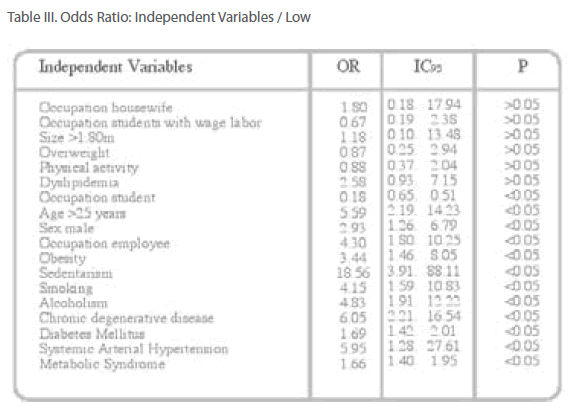
Table III: Odds Ratio: Independent Variables / Low
Discussion
The prevalence of low back pain in this series (63%) was higher than that reported worldwide (4-33%) [1], in USA (8-56%) [2], and Africa (10- 14%) [4]. This high prevalence may be related to the high BMI of the people (which denotes a population with overweight and obesity), and the large proportion of sedentary people. Given these findings, it is necessary to investigate on this matter in order to identify causes and associated factors.
Regarding associated factors, the data was able to corroborate the association of some risk factors described in the literature. Smoking is consistent with what Manchikanti [2], Feldman et al. [7], Deyo [30], Croft [31], and Brage [32] reported. The significant risk with obesity agrees with that informed by Manchikanti [1], Latza et al. [9], Deyo [30], Croft [31], and Brage [32]. Likewise, it also coincided with the risk of sedentarism, noted by Juul-Kristensen et al. [22] and by Ozgu-ler and his group [23]. It also agreed with the results published by Latza et al. [9] which pointed out that the group people >25 years old, were at risk. In addition, the data was able to corroborate that the workers represent a risk group, which agrees with that reported by several authors [2,10,12,22,23,28,29]. On the other hand, there were no references that mention as risk factors: male gender, alcoholism and chronic degenerative diseases; and protective association with the student occupation so it is believed that they are factors associated particularly with the research population. Finally, there was no significant association with female gender, students workers, tall stature and overweight, contrary to the findings reported by Manchikanti [2], Feldman et al.[7], Latza et al. [9], Ozguler et al. [23], and Acouffe et al. [27].
Conclusions
The prevalence of low back pain in beneficiaries of the IMSS, in Comalcalco, Tabasco, Mexico, is greater than that reported in the international literature.
The significant association of low back pain with some risk factors identified in developed countries was not corroborated in the Comalcaco inhabitants, therefore the epidemiological findings reported in several areas should not be adopted by the health care providers without having ratified or rejected such association within its user population. This conclusion and recommendation is applicable to other Latin American populations. To provide better conclusions, larger studies with larger samples, a narrower selection criteria and the inclusion of other variables are required.
Acknowledgments
We thank the authorities of the UMF 11 of the IMSS, Tabasco Delegation, for the facilities granted to carry out this study.
369
References
- Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):215-22.
- Manchikanti L. Epidemiology of Low Back Pain. Pain Physician. 2000;3(2);167-92.
- Peña-Sagredo Jl, Brieva-Beltrán P, Peña-Martín C, Humbría-Mendiola A. Unidades de espalda: un modelo multidisciplinario. Rev Esp Reumatol. 2002;29:499-502.
- Low Q, Morris L, Grimmer-Somers K. The prevalence of low back pain in Africa: a systematic review. BMC Musculoeskeletal Disorders. 2007;8:105-19.
- Barbadillo-Mateos C, Rodríguez-Cardoso A, Herrero-Pardo-de-Donlebún M. Lumbalgias. Jano. 2001;61:101-5.
- Watson KD, Papageorgiou AC, Jones GT, Taylor S, Symmons DPM, Silman AJ, Macfarlane GJ. Low back pain in schoolchildren: the role of mechanical and psychosocial factors. Archs Dis Child. 2003;88:12-7.
- Feldman DE, Shrier I, Rossingnol M, Abenhaim L. Risk factors for development of low back pain in adolescence. Am J Epidemiol. 2001;154(1):30-6.
- Smith DR, Wei N, Ishitake T, Wang RS. Musculoeskeletal disorders among chinesse medical students. Kurume Medical Journal. 2005;52:139-46.
- Latza U, Karmaus W, Stürmer T, Steiner M, Neth A, Rehder U. Cohort study of occupational risk factors of low back pain in construction workers. Occup Environ Med. 2000;57:28-34.
- Kaneda K, Shirai Y, Miyamoto M. An epidemiological study on occupational low back pain among people who work in construction. J Nipón Med Sch. 2001;68(4):310-7.
- Smedley J, Egger P, Cooper C, Coggon D. Prospective cohort study of predictors of incident low back pain in nurses. BMJ. 1997;314:1225-33.
- Ando S, Ono Y, Shimaoka M, Hiruta S, Hattori Y, Hori F, Takeuchi Y. Associations of self estimated workloads with musculoeskeletal symptoms among hospital nurses. Occup Environ Med. 2000;57:211-6.
- Holmberg S, Thelin A, Stiernström EL, Svärdsudd K. Low back pain comorbidity among male farmers and rural referents: a population-based study. Ann Agric Environ Med. 2005;12:261-8.
- Vindigni D, Walter BF, Jamison JR, Da-Costa C, Parkinson L, Blunden S. Low back pain risk factors in a large rural Australian Aboriginal community. An opportunity for massaging co-morbitities? Chiropractic & Osteopathy. 2005;13:21- 33.
- Sauné-Castillo M, Arias-Anglada R, Lleget-Maymo I, Ruiz-Bassols A, Escriba- Jordana JM, Gil M. Estudio epidemiológico de la lumbalgia. Análisis de factores predictivos de incapacidad. Rehabilitación. 2003;37:3-10.
- Noriega-Elió M, Barrón-Soto A, Sierra-Martínez O, Méndez-Ramírez I, Pulido- Navarro M, Cruz-Flores C. La polémica sobre las lumbalgias y su relación con el trabajo: estudio retrospectivo en trabajadores con invalidez. Cad Saúde Pública. 2005;21(3):150-66.
- Champín-Michelena D. Lumbalgia. Rev Soc Per Med Inter. 2004;17(2):50-6.
- Moyá-Ferrer F. Lumbalgia. En: Andreu JL, Barceló P, Figueroa M, Herrero-Beaumont G, Martín-Mola E, Olivé A, et. al., editores. Manual de enfermedades reumáticas de la Sociedad Española de Reumatología. Mosby/Doyma; Madrid. 1996.
- Manek NJ, McGregor AJ. Epidemiology of back disorders: prevalence, risk factors and prognosis. Curr Opin Rheumatol. 2005;17:134-40.
- Peña-Sagredo JL, Peña C, Brieva P, Pérez-Núñez M, Humbría-Mendiola A. Fisiopatología de la lumbalgia. Rev Esp Reumatol. 2002;29:483-8.
- Feyer AM, Herbison P, Williamson AM, De-Silva I, Mandryk J, Hendiré L, Hely MCG. The role of pysical and psychosocial factors in occupational low back pain: a prospective cohort study. Occup Environ Med. 2005;57:116-20.
- Juul-Kristensen B, Jensen C. Self-reported workplace related ergonomic conditions as prognostic factor for musculoeskeletal symptons: the “BIT” follow up study on office workers. Occup Environ Med. 2005;62:188-94.
- Ozguler A, Leclerc A, Landre MF, Pietri-Taleb F, Niedhammer I. Individual and occupational determinants of low back pain according to various definitions of low back pain. J Epidemiol Community Health. 2000;54:215-20.
- Papageorgiou AC, Croft PR, Thomas E, Silman AJ, Macfarlane GJ. Psychosocial risk for low back pain: are these related work? Ann Rheum Dis. 1998;57:500-2.
- Harkness EF, Macfarlane GJ, Nahit ES, Silman AJ, McBeth J. Risk factors for new-onset low back pain amongst cohorts of newly employed workers. Rheumatology. 2003;42:959-68.
- Jones GT, Watson KD, Silman AJ, Symmons DPM, Macfarlane GJ. Predictors of low back pain in british schoolchildren: a poppulation-based prospective cohort study. Pediatrics. 2003;111(4):822-8.
- Acouffe J, Manillier P, Brehier M, Fabin C, Faupin F. Analysis by sex of low back pain among workers from small companies in the Paris area: severity and occupational consequences. Occup Environ Med. 1999;56:696-701.
- Walter-Bone K, Palmer KT. Musculoeskeletal disorders in farmers and farm workers. Occup Med. 2002;52(8):441-50.
- Palmer KT, Griffin MJ, Syddall HE, Pannett B, Cooper C, Coggon D. The relative importance of whole body vibration and occupational lifting as risk factor for low back pain. Occup Environ Med. 2003;60:715-21.
- Deyo RA, Bass JE. Lifestyle and low back pain: the influence of smoking and obesity. Spine. 1989;14:501–6.
- Croft PR, Rigby AS. Socioeconomic influences on back problems in the community in Britain. J Epidemiol Community Health. 1994;48:166–70.
- Brage S, Bjerkedal T. Musculoskeletal pain and smoking in Norway. J Epidemiol Community Health. 1996;50:166–9.
- Instituto Mexicano del Seguro Social. Primer reporte semestral 2007 del Sistema de Información Médica Ordinaria. Diagnósticos más frecuentes en la consulta externa. IMSS; Villahermosa, México. 2007:95-105.
- Instituto Mexicano del Seguro Social. Reporte anual 2006 del Sistema de Información Médica Ordinaria. Diagnósticos más frecuentes en la consulta externa. Unidad de Medicina Familiar No. 11, Tabasco. IMSS; Villahermosa, México. 2007:95-105.
- Instituto Mexicano del Seguro Social. Reporte anual 2006 del Sistema de Información Médica Ordinaria. Incapacidades temporales y permanentes. Unidad de Medicina Familiar No. 11, Tabasco. IMSS; Villahermosa, México. 2007:125-35.


