Nick Youssefi*, Brian Remillard and Dartmouth-Hitchcock
Division of Nephrology, Dartmouth- Hitchcock Medical Center, Dartmouth University, Concord, NH 03303, USA
*Corresponding Author:
Nick Youssefi
Division of Nephrology, Dartmouth- Hitchcock Medical Center
Dartmouth University, Concord, NH 03303
USA
Tel: 1-858-232-3330
E-mail: nicholas.d.youssefi@hitchcock.org
Received date: January 21, 2016; Accepted date: February 18, 2016, Published date: February 22, 2016
Citation: Youssefi N, Remillard B, Hitchcock D. Massive Autosomal Dominant Polycystic Kidneys: Case Report of 18 kg Polycystic Kidneys. Ann Clin Lab Res. 2016, 4:1.
Autosomal dominant polycystic kidney disease (ADPKD) is an inherited, progressive, systemic disorder with renal and extra renal involvement. The incidence is 1 in 500 to 1000, with 50% of cases progressing to end-stage renal disease by the age of 60. Renal manifestations include multiple cysts, pain, hypertension, hemorrhage, infection, and renal failure. Extra renal involvement includes liver cysts, intracranial aneurysms, mitral valve prolapse, and colonic diverticulosis [1]. We report a case of massive polycystic kidney disease requiring bilateral nephrectomy and hemodialysis.
Introduction
Autosomal dominant polycystic kidney disease (ADPKD) is an inherited, progressive, systemic disorder with renal and extra renal involvement. The incidence is 1 in 500 to 1000, with 50% of cases progressing to end-stage renal disease by the age of 60. Renal manifestations include multiple cysts, pain, hypertension, hemorrhage, infection, and renal failure. Extra renal involvement includes liver cysts, intracranial aneurysms, mitral valve prolapse, and colonic diverticulosis [1]. We report a case of massive polycystic kidney disease requiring bilateral nephrectomy and hemodialysis.
Case History
A 44-year-old gentleman with a history of autosomal dominant polycystic kidney disease, hypertension, atrial fibrillation who was being followed by the nephrology service. Patient was diagnosed with ADPKD at the age of 27 when he had an episode of flank pain prompting computed tomography scan of the abdomen/ pelvis which revealed multiple bilateral renal cysts. Family history of ADPKD including 3 brothers and one daughter, CKD Stage 3a-b, creatinine stable 1.3 - 2.3 mg/dL for nearly 16 years. However, over the course of the next few months the patient developed progressive shortness of breath, poor appetite, and ruptured cysts. Computed tomography scan abdomen/pelvis revealed multiple renal cysts, largest 14 × 11 × 10 cm displacing the abdominal viscera. Serum creatinine increased to 4.3 mg/dL. On exam, his blood pressure was 141/81 mmHg and abdominal exam revealed moderately distended and diffusely tender abdomen, while bowel sounds was loud. No organs or masses could be identified by palpation. Given progression of his symptoms and worsening renal function, the patient had an open left nephrectomy with the specimen weighing 20 pounds (9 kg). Patient tolerated surgery well and was discharged home with a serum creatinine 5.3 mg/ dL without need for dialysis. The patient’s creatinine continued to rise slowly each month for the next six months thereafter, however the patient was asymptomatic and did not require any further hospitalizations during this time. Six months later the patient developed abdominal pain, poor appetite and was found to have hemorrhagic cysts on subsequent MRI abdomen. He had worsening renal function with serum creatinine increasing from 5 mg/dL to 8.8 mg/dL. Patient was started on hemodialysis. Patient was evaluated by surgery and given retractable pain, poor appetite, nausea, and hemorrhagic cysts, the patient had a right nephrectomy with the specimen weighing 20 pounds (9 kg). The patient tolerated surgery well and was discharged home thereafter. Patient is currently on hemodialysis with improvement in pain and appetite after bilateral nephrectomy (Figure 1).
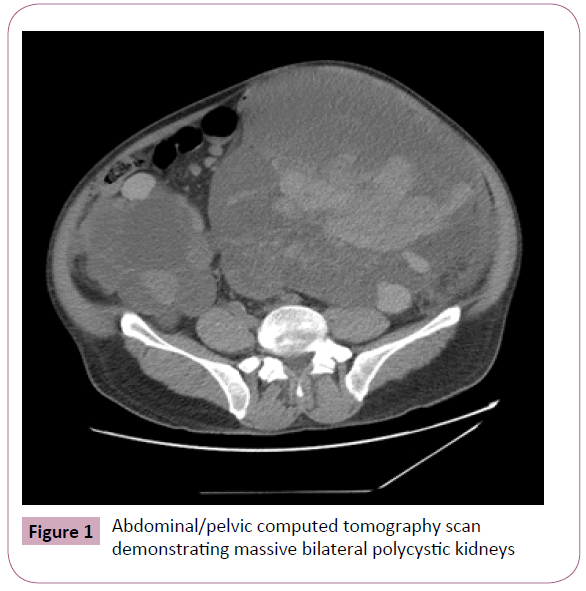
Figure 1: Abdominal/pelvic computed tomography scan demonstrating massive bilateral polycystic kidneys
Discussion
Therapeutic nephrectomy is indicated for symptomatic and malignant ADPKD. Symptoms include pain, nausea, early satiety, constipation, hypertension, recurrent pyelonephritis, and gross hematuria which can all markedly affect quality of life. Additionally, surgery may also be indicated to facilitate placement of a renal allograft if concerned about lack of space due to massive cystic disease. Significant research is ongoing on ADPKD, including compensatory hypertrophy of the remaining solitary kidney post unilateral nephrectomy. Nephrogenesis is complete before birth, and thus compensatory growth of the remaining adult kidney is known to be caused by hypertrophy and hyperfiltration of nephrons [2]. One study suggested nearly 44% of patients developed compensatory renal hypertrophy as a result of unilateral functioning kidney [3,4]. This finding has also been noted in other studies and may reflect the ability to maintain relative normal renal function [5]. Our case highlights one of the most massive polycystic kidneys reported in the literature (40 pounds/18 kg total weight).
8691
References
- Rahul B(2014) Laparoscopic nephrectomy for massive polycystic kidney disease: Updated technique and outcomes. Can Urol Assoc J 8:341-345.
- VanVuuren (2012) Compensatory enlargement of a solitary functioning kidney during fetal development. UltrasoundObstet Gynecol 40:665-668.
- Wisenbaugh E (2000) Massive renal size is not a contraindication to a laparoscopic approach for bilateral nativenephrectomies in a autosomal dominant polycystic kidney disease. BJU International 2015; 115: 796-801.
- Fetal H(2000) Compensatory Renal Hypertrophy with a Unilateral Functioning Kidney. Ultrasound ObstetGynecol 15: 191-193.
- Heymans C (1998) Multicystic kidney dysplasia: a prospective study on the natural history of the affected and contralateral kidney. Eur J Pediatric 157: 673-675.


