Karina Lie Akinaga, Fabiano Reis, Maria Augusta Montenegro*
1Department of Neurology, State University of Campinas, Brazil
*Corresponding Author:
Maria Augusta Montenegro
Department of Neurology, FCM Unicamp, Rua Tessália Vieira de Camargo, 126, CEP: 13083-887; Campinas, SP, Brazil
Tel: 55 19 35217372
E-mail: guga.32@hotmail.com
Received Date: June 14, 2015; Accepted Date: June 17, 2015; Published Date: June 20, 2015
Citation: Akinaga KL, Reis F, Montenegro MA. Neuroimaging of Congenital Cytomegalovyrus. J Neurol Neurosci. 2016, 6:1. DOI: 10.21767/2171-6625.100016
We present three patients with developmental delay, hearing impairment and microcephaly. Although all three patients have congenital ciytomegalovyrus (CMV) infection and all three have similar clinical presentation, the neuroimaging findings are completely different in each patient.
CMV is a type of herpesviruses. It affects the fetus transplacentally, and is one of the most common causes of congenital infection. Most congenitally infected children do not have symptoms. However, some patients can present the classical symptoms of intrauterine growth retardation, prematurity, petechiae, hepatosplenomegaly, jaundice, microcephaly, hearing impairment, chorioretinitis and brain abnormalities [1].
The diagnosis is established by polymerase chain reaction of urine or saliva samples [2]. The isolation of the virus through viral culture canhearing impairment also be performed. The virus should be detected within 2-3 weeks of life.
The most common neuroimaging findings include intracranial calcification (Figure 1A), polymicrogyria (Figure 1B), and white matter disease (Figure 1C). Differential diagnosis should include congenital toxoplasmosis, isolated polymicrogyria and leukodystrophy.
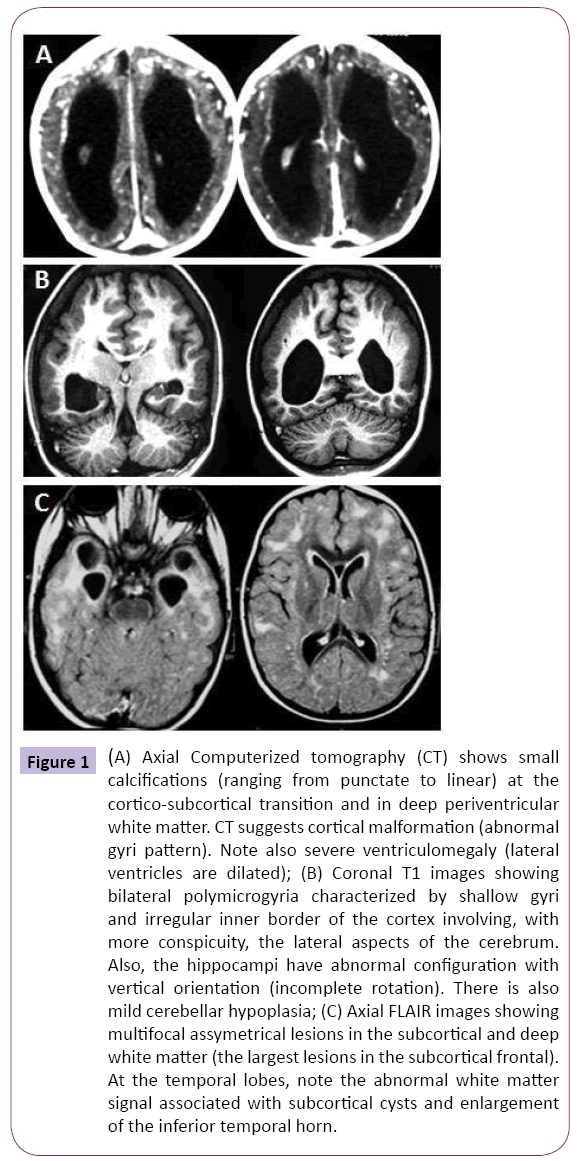
Figure 1: (A) Axial Computerized tomography (CT) shows small calcifications (ranging from punctate to linear) at the cortico-subcortical transition and in deep periventricular white matter. CT suggests cortical malformation (abnormal gyri pattern). Note also severe ventriculomegaly (lateral ventricles are dilated); (B) Coronal T1 images showing bilateral polymicrogyria characterized by shallow gyri and irregular inner border of the cortex involving, with more conspicuity, the lateral aspects of the cerebrum. Also, the hippocampi have abnormal configuration with vertical orientation (incomplete rotation). There is also mild cerebellar hypoplasia; (C) Axial FLAIR images showing multifocal assymetrical lesions in the subcortical and deep white matter (the largest lesions in the subcortical frontal). At the temporal lobes, note the abnormal white matter signal associated with subcortical cysts and enlargement of the inferior temporal horn.
Congenital CMV treatment and prevention remains a challenge. Recent evidence showed that treatment with hyperimmune globulin did not significantly modify the course of primary CMV infection during pregnancy [3].
6754
References
- Trincado DE, Rawlinson WD (2001) Congenital and perinatal infections with cytomegalovirus. J Paediatr Child Health37:187-192.
- Gunkel J, Wolfs TF, Nijman J (2014) Urine is superior to saliva when screening for postnatal CMV infections in preterm infants. J ClinVirol61:61-64.
- Revello MG, Lazzarotto T, Guerra B (2014) A randomized trial of hyperimmune globulin to prevent congenital cytomegalovirus. NEngl J Med 370:1316-1326.

