Jesús Porta-Etessam MD1*, Rocío Garcia-Cobos MD1 Raul Barbosa MD2, Alvaro Martín-Ruiz MD2, Ignacio Casanova MD1, Teresa Lapeña MD1, Carmen Blasco Fanlo MD2
1Headache and neuroophthalmology Unit. Neurology Department. Hospital Clínico Universitario San Carlos. Madrid.
2Emergency Department. Hospital Clínico Universitario San Carlos. Madrid.
*Corresponding Author:
Dr Jesús Porta-Etessam
C/ Andrés Torrejón, 15, 7º 28014 Madrid. Spain
Phone: +34667062490
Fax: +34 91552719
E-mail:jporta@yahoo.com., mporta@caminos.recol.es
Keywords
Ocular Flutter, Pathophysiology, amphetamine
Introduction
Ocular flutter (OF) is one of the two types of eye movement abnormalities lack the intersaccadic interval [1]. Typically presents burst of horizontal movements that use to have quite small amplitude and very high frequency. In the other hand opsoclonus (OC) presents multidirectional eye movements [1,2]. These types of eye movements have been described with different situations as paraneoplastic, postinfection, hyperosmolar coma, toxic chemicals and drugs intoxication [1-4]. We present the first case of ocular flutter related with amphetamine intoxication and discuss the physiopathology of this interesting syndrome and the biochemical differences between OF and OC.
Clinical case
A-15-years-old Caucasian male with not previous medical history experienced a rapid onset of dizziness and blurred vision while he was playing soccer. There were no other complaints such as weakness, headache or jumping vision. There were not familiar or personal past medical history of migraine epilepsy or other neurological diseases. On neurological admission the patient was nervous, there were no cognitive deficit. Clinical eye movements examination revealed frequent horizontal and symmetric involuntary conjugated burst of large to-and fro. There was a bilateral pupil mydriasis but no motor or sensory deficit, no tremor and no limb ataxia and deep tendon reflexes were all presents. Blood pressure was 145/90 mm Hg and pulse 105 beats/min. An electrocardiogram revealed a supraventricular tachycardia. Blood count and routine biochemistry were normal. CT performed on admission was normal. CSF contained 0 lymphocytes/mm3, 45 mg/dl and normal glucose levels. Urine drugs analysis was positive for amphetamine. All symptoms progressively resolved within 6 hours. An MRI performed 48 hours after admission was normal. On follow up the patient remained asymptomatic six months later.
Discussion
The horizontal to-and-fro saccadic oscillations observed in this patient correspond to the definition of ocular flutter. In our opinion the most interesting aspects of this case are: 1) that amphetamine could induce OF and 2) that the relationship between OF and amphetamine should have biochemical and pathophysiological implications.
OF is a burst of involuntary saccadic horizontal oscillations without an intersaccadic interval [1,2]. According to physiological models (fig 1) excitatory premotor burst neurons (EPBN) are inhibit by omnipause (OPN) neurons secreting in the synaptic cleft glycine; on the other hand, EPBN stimulated the inhibitory premotor burst neurons (IPBN) using glutamate and finaly this neurons inhibit OPN [5]. Amphetamine produces a delayed and sustained increase in glutamate levels [6,7]. The amphetamine increase will induce an stimulation in common oculomotor integrator and in IPBN, and secondary to the IPBN and OP cells inhibition. The result of these neurotransmitters changes is a burst of involuntary saccadic movement.
On the other hand ¿why are these burst movement in horizontal directions? This interesting question could be explained because horizontal IPBN neuron seems to be gycergic and vertical-IPBN neurons gabaergic [8, 9]. This neurotransmitter difference could explain the question.
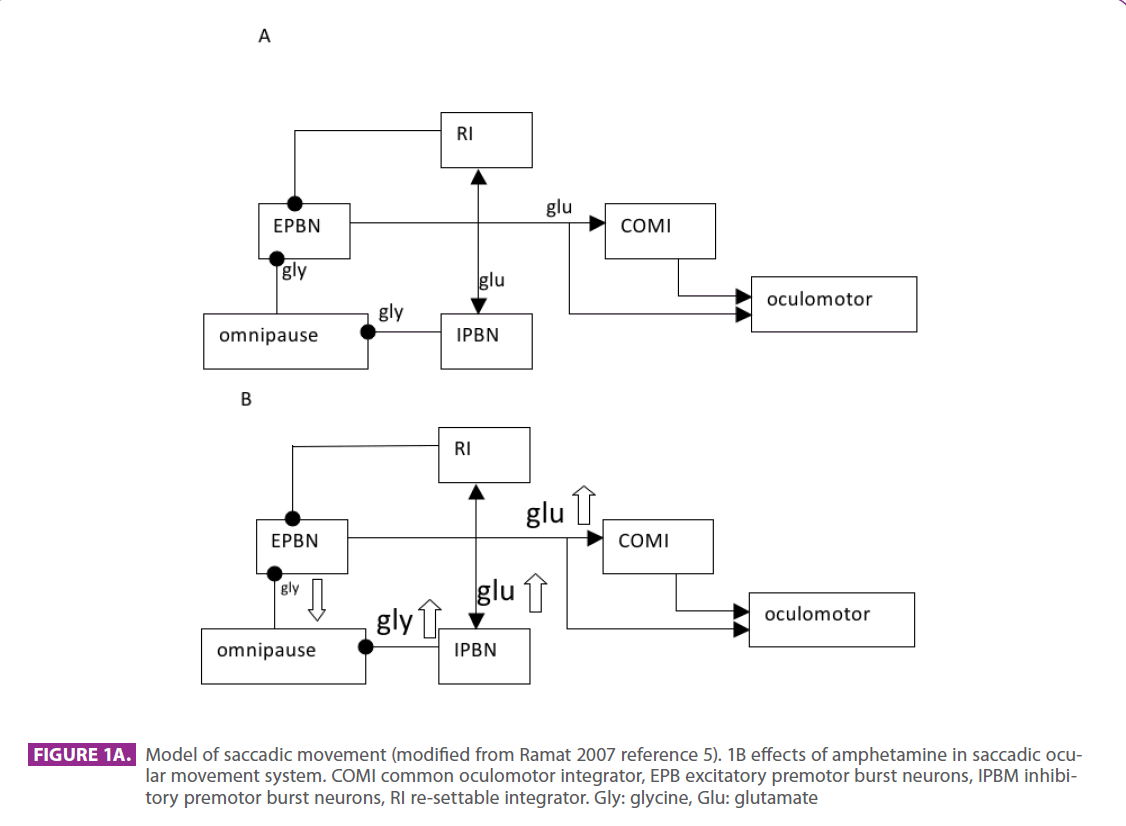
Figure 1A. Model of saccadic movement (modified from Ramat 2007 reference 5). 1B effects of amphetamine in saccadic ocular movement system. COMI common oculomotor integrator, EPB excitatory premotor burst neurons, IPBM inhibitory premotor burst neurons, RI re-settable integrator. Gly: glycine, Glu: glutamate
Although al lesion of OPN could produce OF, a dysfunction in other neuron of the saccadic system could explain this syndrome. The horizontal predominance of burst movement could be explained because a neurotransmitters differences in horizontal and vertical IPBN neurons. Amphetamine intoxication should be consider in the differential diagnosis of OF.
2213
References
- Leigh RJ, Zee DS. The neurology of eye movements (Book/DVD). Fourth edition. New York: Oxford University Press; 2006.
- Liu GT, Volpe NJ, Galetta SL. Neuro-ophthalmology. Diagnosis and management. First Edition. Philadephia: Saunders Company; 2001.
- Verhaeghe S, Diallo R, Nyffeler T, Rivaud-Péchoux S, Gaymard B. Unidirectional ocular flutter. J Neurol Neurosurg Psychiatry. 2007;78:764-6.
- Zaro-Weber O, Galldiks N, Dohmen C, Fink GR, Nowak DA. Ocular flutter, generalized myoclonus, and trunk ataxia associated with anti-GQ1b antibodies. Arch Neurol. 2008;65:659-61.
- Ramat S, Leigh RJ, Zee DS, Optican LM. What clinical disorders tell us about the neural control of saccadic eye movements. Brain. 2007;130:10-35.
- Wolf ME, Xue CJ, Li Y, Wavak D. Amphetamine increases glutamate efflux in the rat ventral tegmental area by a mechanism involving glutamate transporters and reactive oxygen species. J Neurochem. 2000 Oct;75(4):1634-44.
- Paladini CA, Fiorillo CD, Morikawa H, Williams JT. Amphetamine selectively blocks inhibitory glutamate transmission in dopamine neurons. Nat Neurosci. 2001;4:275-81.
- Spencer RF, Wang SF. Immunohistochemical localization of neurotransmitters utilized by neurons in the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF) that project to the oculomotor and trochlear nuclei in the cat. J Comp Neurol. 1996;366:134-48.
- Miura K, Optican LM. Membrane channel properties of premotor excitatory burst neurons may underlie saccade slowing after lesions of omnipause neurons. J Comput Neurosci. 2006;20:25- 41.

