Sunny Modi1* and Matthew Pavicic2
1Redcliffe Hospital, Queensland, Australia
2Greenslopes Private Hospital, Newdegate Street, Brisbane, Queensland- 4120, Australia
*Corresponding Author:
Sunny Modi, Redcliffe Hospital
Sunny Modi, Redcliffe Hospital
13, Tarragon Parade, Griffin
Queensland 4503, Australia
Tel: +61423000576
E-mail: sunny_modi003@hotmail.com
Received date: May 26, 2016; Accepted date: June 01, 2016; Published date: June 10, 2016
Citation: Modi S, Pavicic M. Omental Infarction from a Blunt Trauma in a Child-Should we Panic?. Trends Green Chem. 2016, 4:2.
Omental Infarction (OI) is a rare cause of acute abdomen in children and often misdiagnosed as acute appendicitis due to itssimilar clinical presentation.Omental infarction is caused by rotation of the greater omentum on its long axis which may lead to tissue ischemia/infarction and necrosis. Of the 400 reported cases of OI, only 50 involved paediatric patients, with the majority presenting as right lower quadrant abdominal pain.
Case Presentation
A five year old boy presented to his General Practitioner with a one day history of right lower abdominal pain after a fall at school. The boy was unable to give a history of the mechanism of the fall. He denied any history of fever, nausea or vomiting. An USS and a CT abdomen were arranged by the child’s GP which revealed an omental infarction (Figure 1). He was transferred to the hospital for further management. The patients’ blood test showed white cell count of 9.2 x 109 per liter and C-reactive protein of 24 units. The patient was managed conservatively and discharged home next day.
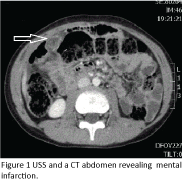
Figure 1: USS and a CT abdomen revealing Omental infarction.
Discussion
Omental infarction is a rare cause of an acute abdomen in children, with more than 85% of reported cases occurring in adults [1-3]. It is often not initially considered as a differential diagnosis of an acute abdomen in children. The right-sided omental torsion is much more common than a left-sided one, because the right part of the omentum is longer and has anatomically altered vasculature, which is less tolerant of spontaneous venous stasis and is prone to thrombosis secondary to stretching of omental vein [4], however there are case reported with left sided and epigastric abdominal pain [5].
Omental torsion can be primary or secondary due to; acute pancreatitis, cholecystitis, tumors, appendix epiploica, diverticulitis, adnexitis, or post-surgical adhesions [6]. Other etiologies are; obesity, blunt trauma, strong sudden increase in intra-abdominal pressure brought on by coughing or violent exercise, accelerated peristalsis, or some acute process in an intracavitary organ that causes the migration of a segment of the omentum to the affected site [7].
Early identification of omental infarction by abdominal USS or CT scan appears to prevent unjustified surgical procedures and reduce the length of hospital stay [8]. Rimon et al. reported the largest case series of paediatric patients showing success from a conservative approach in 14 of 19 pediatric patients treated with IV antibiotics, analgesia and hydration. Symptoms resolved without any complications. Surgical exploration in 5 patients was performed due to a clinical suspicion of appendicitis [8]. In another case series of 4 patients by Park TU et al diagnosed omental infarction by CT scan in which 1 patient underwent laparoscopy because his abdominal pain persisted despite conservative treatment and recommended conservative care because this disease runs a self-limited course [9].
Conclusion
We report one of the rarest cases of omental infarction in a paediatric patient caused due to blunttrauma injury. The patient was managed successfully with conservative management. Omental infarction should be included in the differential diagnosis list of acute abdominal pain because it can occur at any site [9]. OI is now described as a self-limiting condition supported by CT imaging data at 1-3 years follow-up [5] and can be treated conservatively avoiding unnecessary surgery. An initial short trial period of conservative management is warranted in all cases. The surgery may be indicated for uncertain diagnosis or persisted abdominal pain despite conservative treatment.
9586
References
- Hosseinpour M, Abdollahi A, Jazayeri H, TalariHR, Sadeghpour A (2012)Omental Torsion After Repeated Abdominal Blunt Trauma.Arch Trauma Res 1: 75-78.
- Tsunoda T, Sogo T, Komatsu H, Inui A, Fujisawa T (2012) A case report of idiopathic omental infarction in an obese child. Case Rep Pediatr.
- Grattan-Smith JD, Blews DE, Brand T (2002) Omental infarction in pediatric patients: sonographic and CT findings. AJR Am J Roentgenol 178: 1537–1539.
- Helmrath MA, Dorfman SR, Minifee PK (2001) Right lower quadrant pain in children caused by omental infarction. Am J Surg 182: 729-732.
- Walia R, Verma R, Copeland N, Goubeaux D, Pabby S, et al. (2014) Omental Infarction: An Unusual Cause of Left-Sided Abdominal Pain ACG Case Rep J 1: 223-224.
- Chaudhary D, Rajkarnikar R, Joshi MR, Thapa P, Singh DR, et al. (2005) Omental torsion: a case report. Kathmandu Univ Med J (KUMJ) 3: 170-172.
- Hosseinpour M, Abdollahi A, Jazayeri H, Talari H R, Sadeghpour A (2012) Omental Torsion After Repeated Abdominal Blunt Trauma. Archives of Trauma Research 1: 75-78.
- Rimon A, Daneman A, Gerstle JT (2009) Omental infarction in children. J Pediatr155: 427–431.
- Park TU, Oh JH, Chang IT, Lee SJ, Kim SE, et al. (2008) Omental infarction: case series and review of the literature. J Emerg Med 42: 149-154.

