Keywords
Traumatic cervical spinal injury; Mortality and intensive care unit
Introduction
Cervical spine injury occurs in 1.5-3% of all patients with major trauma cases [1]. Acute cervical spine injury is associated with significant morbidity and mortality causing an immense social and financial burden on the society. Approximately 50% of traumatic spinal cord injuries occur in the cervical spine and because of the complex nature of this region and its association with vital structures, a person with cervical spinal cord injury is at immediate risk of significant neurological damage like quadriplegia, respiratory distress, hypoxia, cardiovascular instability or death [2,3].
Intensive care management is essential for monitoring, mechanical ventilation, inotropic support for the prevention of secondary injury due to a need for high-level acute care in the short term and associated secondary complications that can occur in the long term [4].
The outcome of these injuries depends not only on the primary injury that occurs at the time of accident but also on the carefulness of management of the secondary injury during resuscitation and the intensive care [5].
Despite improved emergency care, aggressive treatment of complication and the development of specialist center for spinal cord injury, the 3-months mortality rate of traumatic cervical spinal cord injury in the developed country was 20-21% [6]. However, in the developing country like Nigeria the mortality is as high as 34.1% [7].
The independent predictor of mortality in spinal cord injury are age, level of cord lesion, Glasgow coma score, respiratory failure [6,8]. The principal causes of death are respiratory disorder, cardiovascular disorders, pulmonary embolism, infection and suicide [6,8].
However, there is still dearth of information on outcome of traumatic cervical spinal cord injury in our Intensive Care Unit (ICU).
This study aims to determine the outcome and factors affecting the outcome of patients with traumatic cervical spinal cord injury admitted into a general ICU.
Literature Review
This was a descriptive retrospective review of records of patients with traumatic cervical spine injury admitted into the general ICU of University College Hospital, Ibadan, Nigeria over a five - year period (January 2015 to December 2019). The hospital is a tertiary health facility with a capacity of a thousand bed space and 10 ICU bed spaces, referral of patients was from Oyo state and its neighboring states. The ICU is a general one provided services for all the critically ill patients admitted into the hospital.
All traumatic cervical spinal cord injury managed conservatively between January 2013 to December 2017 was included into the study while patients who were surgically managed before admission into the ICU were excluded from the study. A consultant anaesthetist supervised the data extraction from the ICU admission and treatment register.
All the patients admitted through the accident and emergency unit of the hospital were resuscitated according to the Advanced Traumatic Life Support (ATLS) protocol. The patients had appropriate radiographic and haematological investigations. The patients were reviewed by the consultant anesthetist’s or Senior registrar in the ICU. The conservative management of patients with cervical spine injury involved keeping patients in bed with decompression and alignment maintained by longitudinal traction with skill traction using Gardner-wells traction and Philadelphia collar. Patients were given intravenous fluids, analgesic, antibiotics, oxygen therapy, mechanical ventilation and Dopamine Infusion where indicated.
Data extracted were age, gender, cause of injury, associated injury, mechanical ventilation or inotropic support given, number of days spent in ICU and outcome (alive or mortality).
Data were analyzed using Statistical Package for Social Sciences (SPSS 20.0 Inc). Chicago Illinois. Continuous variables were presented as means ± standard deviation whereas categorical variables were presented as frequency and percentages. Association between mortality outcome and demographic and clinical parameters was determined with chi square test and the level of significance was set at p value of less than 0.05.
Results
The total number of cervical spinal cord injured patients admitted during the five- year study period into the intensive care unit for conservative management was 32 consisting of 25 (78.1%) male and 7 (21.9%) female; the male: female ratio was 3:1. The mean age of the patients was 38.2 ± 16.16 years with the age range between 7 to 77years.
Twenty-eight (87.5%) patients sustained injury following road traffic injury (RT1) while 4 (12.5%) patients sustained injury from falls (Figure 1). Most of the injuries occurred between the second and the fourth decade of life (Figure 2). Seven patients had associated injury, 4 patients had head injury, humeral fracture in 2 patients and ribs fracture in one patient. Cervical spine injury at C3 was the commonest level of injury n=18 followed by C4 level n=11 and C5 level n=3 (Figure 3). The period of ICU stay ranged from 1-53 days and majority (42%) spent seven days in the ICU before demise or discharge (Figure 4).
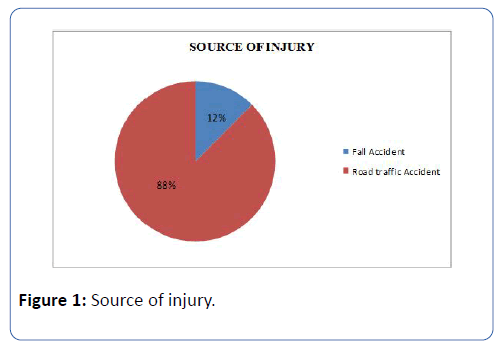
Figure 1: Source of injury.
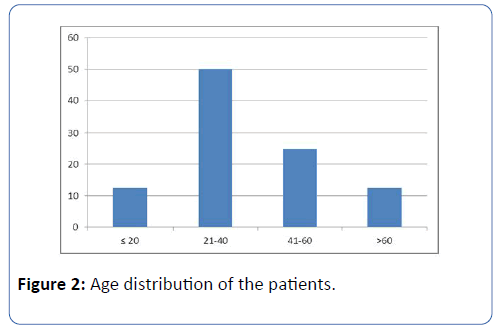
Figure 2: Age distribution of the patients.
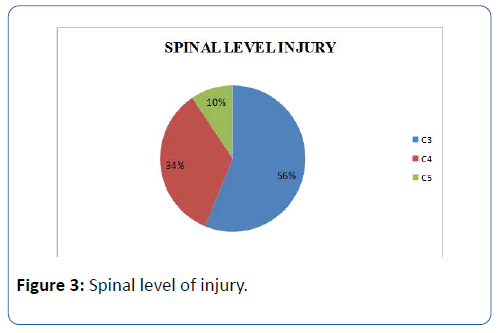
Figure 3: Spinal level of injury.
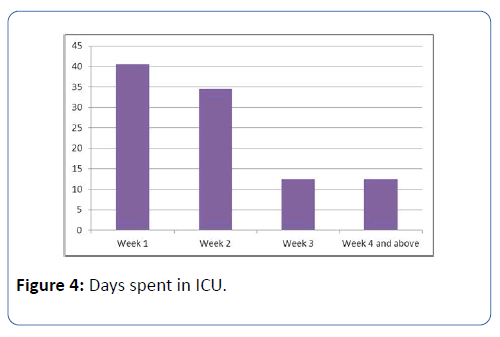
Figure 4: Days spent in ICU.
Fifteen patients died and the proportional mortality was 46.9%. Table 1 shows information of the bivariate analysis of factors associated with outcome management. A significant association was found among patients who stayed ≤ 7 days in ICU (P=0.036), mechanically ventilated (P=0.015) and inotropic support (P=0.001). Age, sex and level of cervical spine injury were not significantly associated with mortality in this study.
| Variables |
Outcome of spine injury |
P- value |
| Dead n (%) |
Alive n (%) |
| Sex |
| Male |
10 (40.0) |
15 (60.0) |
0.141 |
| Female |
5 (71.4) |
2 (28.6) |
| Age (years) |
| < 30 |
5 (55.6) |
4 (44.4) |
0.585 |
| ≥ 30 |
10 (43.5) |
13 (56.5) |
| Spinal level of injury |
| C3 |
7 (38.9) |
11 (61.1) |
0.144 |
| C4 |
5 (45.5) |
6 (54.5) |
| C5 |
3 (100.0) |
0 (0.0) |
| Ventilation |
| Yes |
7 (100.0) |
0 (0.0) |
0.015* |
| No |
8 (37.0) |
17 (68.0) |
| Inotrope use |
| Yes |
10 (90.9) |
1 (9.1) |
0.001* |
| No |
5 (23.8.) |
16 (76.2) |
| LOS in ICU (days) |
| ≤ 7 |
9 (69.2) |
4 (30.8) |
0.036* |
| > 7 |
6 (31.6) |
13 (68.4) |
| *Significant |
Table 1: Bivariate analysis of factors associated with outcome of spine injury.
Discussion
Spinal cord injury is a major cause of morbidity and mortality in both developed and developing countries [7-10]. The mortality in this review was 46.9% higher than 21% reported by Claxon et al. [6] and 26.2% documented in Brazilian data of traumatic cervical spinal cord injury [8] whereas Daverat et al. reported 20% mortality [9]. This higher figure in our study may be due to poor health care delivery and care in Nigeria generally.
Majority of the patients with spinal cord injury were males as reported in this study and from studies in Nigeria and other developed countries as males are more prone to outdoor work and other trauma [7-9]. Mortality was more in males but gender was not found to be a predictor of mortality in this study similar to a report by Kawu et al. [7,10].
Age has been shown to be associated with poor outcome in patients with spinal cord injuries [6,9]. Elderly patients generally have poor outcome after trauma and Wick et al. showed that mortality of patients greater than 50 years was greater in tetraplegic patients requiring long term ventilation [10]. However, our study did not demonstrate age as a predictor of mortality; mortality was more in patients less than 30 years of age. Finding in our study may be due to the fact that the peak age group of 21-40 years was the most susceptible for cervical spinal injury.
The level of cord injury had been found to be a predictor of mortality in some studies [6,7], in a similar study by Claxon et al. [6] they found that patients with low levels of cervical injury had higher mortality due to paralysis of the diaphragm with its attending respiratory complication. However, in our study level of cord injury was not found to be a significant risk factor for mortality similarly Daverat et al. [9] did not identify cord injury level to be an independent predictor of mortality, they attributed low level of cord injury to be related to respiratory difficulty which is in itself a more important predictor of mortality.
Our study also found that respiratory failure needing mechanical ventilation was found to be a predictor of mortality, this was found to be similar to a study by Neumann et al. [8] they found that the need for respiratory support was an independent predictor of deaths in cervical spine injury. Respiratory insufficiency and related complication are the most common causes of morbidity and mortality in the short and long term in patients with spinal cord injury with an incidence as high as 83% [11]. Claxion et al. also addressed factors associated with the need for mechanical ventilation in their study [6], and found copious sputum and pneumonia to be the independent predictors of the need for mechanical ventilation. They concluded that close attention to the prevention, recognition and treatment of secretion retention may reduce the need for mechanical ventilation after the onset of traumatic tetraplegia thereby improving outcome in mechanically ventilated patients.
Hypotension needing inotropic support was found to be a predictor of mortality in our study similar to a study by Neumann et al. [8]. Cardiovascular disorder is frequently seen following upper thoracic and cervical cord injury and is responsible for 40.5% of deaths in a study by Garshick et al. [12]. In a study of patients with complete spinal cord injury; 68% were hypotensive and 35% of them required inotropic support whereas people with incomplete cervical spine injury had fewer cases of hypotension and inotrope were noted [13].
Our study showed that the initial period where mortality was extremely higher was in the first week of admission into the ICU and this was significant. This may point to the fact that patients with cervical spinal injury may die on the spot of injury or experience early death in the ICU. Cardiopulmonary complications have been found to be the major cause of early death in patients with cervical spine injury [6-8]. Claxion et al. [6] attributed early mortality in their study to associated head injury causing respiratory abnormalities like pulmonary oedema, aspiration pneumonitis and ventilation: perfusion mismatch [6]. In a study by Lalwani et al. [14], conducted on mortality profile of patients with traumatic spinal injury, 20.5% of patients studied had early deaths due to respiratory failure or post- trauma complication and those that died after one week [15] were due to secondary complications like sepsis or multiple organ system failure similar observation was reported by Reber et al. [16].
Conclusion
There is a need for the establishment of a dedicated spinal cord injury ICU in our hospital and across the country with good accessibility to poor sections of society for comprehensive management of spinal cord injury. Training of paramedics to carry patients to prevent more damage to the spinal cord during transfer is also necessary.
28344
References
- Crosby ET, Lui A (1990) The adult cervical spine: Implications for airway management. Can J Anaesth 37: 77-93.
- Abu-Laban R (1991) Snowboarding injuries: An analysis and comparison with alpine skiing injuries. CMAJ 145: 1097-1103.
- Song J, Shao J, HH Q, Song D, Zhu W (2015) Risk factors for respiratory failure with tetraplegia after acute traumatic cervical spinal cord injury. Eur Rev Med Pharmacol Sci 19: 9-14.
- Krueger H, Noonan V, Trenaman L, Joshi P, Rivers C (2013) The economic burden of traumatic spinal cord injury in Canada. Chronic Dis Inj Can 33: 113-122.
- Lazar L, Yarkony G, Ortolano D, Heinemann A, Perlow E, et al. (2009) Prediction of functional outcome by motor capability after spinal cord injury. Arch Phys Med Rehabil. 70: 819-822.
- Claxton AR, Wong D, Chung F, Fehlings MG (1998) Predictors of hospital mortality and mechanical ventilation in patients with cervical spinal cord injury. Can J Anaesth 45: 144-149.
- Kawu AA, Salami AO, Olawepo A, Alimi FA, Gbadegesin AA, et al. (2011) Prehospital transport of patients with spinal cord injury in Nigeria. J Spinal Cord Med 34: 308-311.
- Neumann C, Albers B, Asil FA (2009) Risk factors for mortality in traumatic cervical spinal cord injury. Brazilian Data J Trauma 67: 67-90.
- Daverat P, Gagnon M, Dartgues JF, Mazaux M, Barat M (1989) Initial factors predicting survival in patients with a spinal cord injury. J Neurol Neurosurg Psychiatry 52: 403-406.
- Furlan JC, Krassioikou AV, Fuhlings MG (2005) The effect of gender on clinical and neurological outcome after acute cervical spinal cord injury. J Neurotrauma 22: 368-381.
- Burns AS, O’Connell C (2012) The challenge of spinal cord injury care in the developing world. J Spinal Cord Med 35: 3-8.
- Garshick E, Kelley A, Cohen SA, Garrison A, Tun CG, et al. (2005) A prospective assessment of mortality in chronic spinal cord injury. Spinal cord. 43: 408-416.
- Ahidjo KA, Mustapha AF, Sulaiman GAA, Abdulganiyu SOO (2011) Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria. Int J Biol Med Res 2: 646-651.
- Lalwani S, Singh V, Trikha V, Sharma V, Kumar S, et al. (2014) Mortality profile of patients with traumatic spinal injuries at a level I trauma cre centre in India. Indian J Med Res 140: 40-45.
- Radjou A, Pal R, Balliga D, Mahajan P (2012) Injury-related mortality audit in a regional trauma center at Puducherry, India. J Emerg Trauma Shock 5: 42-48.
- Reber P, Schmied B, Seiler C, Baer H, Ali E (1998) Missed diaphragmatic injuries and their long-term sequelae. J Trauma Acute Care Surg 44: 183-188.


