Noor Kamil1* and Saba Kamil2
1Department of Pharmaceutical Sciences, College of Clinical Pharmacy, King Faisal University, Saudi Arabia
2Cancer Hospital, King Faisal University, Saudi Arabia
Corresponding Author:
Noor Kamil
Department of Pharmaceutical Sciences, College of Clinical Pharmacy, King Faisal University, Saudi Arabia
Tel: 966534541157
E-mail: noorkamil@hotmail.com
Received date: 20 May 2016; Accepted date: 10 June 2016; Published date: 14 June 2016
Citation: Kamil N, Kamil S. Pediatric Cancer Incidences. Arch Can Res. 2016, 4:2.
Keywords
Cancer incidences, Pediatric cancer, Cancer causes
Introduction
In United States cancer is the top disease-related cause of mortality among children of less than 15 years of age. Although 5-year survival rate has increase significantly, but more than 100,000 person-years of life are lost in each cancer year [1]. Pediatric cancers vary according to the tissue type, its site of origin, genetics, gender and age. As an origin of fatalities, it differs in its comparative significance over the age range from neonate till 19. The possibility of developing cancer before the age of 20 fluctuates somewhat by gender. Probability of developing cancer in males is 1 in every 300 (0.32%) and in females it’s about 1 in every 333 (0.30%) [2]. Most forms of pediatric malignancies except Hodgkin’s disease, have raised approximately 1 percent yearly since 70s [3]. A greater increase has been recorded in the central nervous system cancer (25%) and acute lymphocytic leukemia (ALL) up to 20 percent, whereas it was reduced up to 10 percent when all the cancer types are collectively calculated between the periods of 1973 and 1991 in children less than 15 years of age. Some investigators believe that this rise in incidence of numerous pediatric cancers, like brain tumors, leukemias, and some neuroblastomas is due to the dramatic improvements in diagnostic techniques and reporting system [4]. Nonetheless these variations do not elucidate escalations for all classes of pediatric malignancies. However pediatric cancer rate has increased in past years, but the mortality rate in children due to cancer in USA has decreased significantly in present years due to the better and early identification and treatment. Though the pediatric cancer incidences have risen in all ages but greatest increased has found in pediatrics of ages from 10 to 14.
Material and Methods
Design, place and duration of study
The study has been conducted to determine the incidences of child hood cancer. Individuals were selected without the discrimination of race and sex. A two years study was done in the Children Cancer Hospital-Karachi. Data has been recorded on individual patient’s files and later collected on a specific form design for the study.
Subjects
A total 106 pediatric cancer patients were enrolled during the 2 years study period. Pediatric patients were categorized into 4 different groups i.e. Infants ages 1-12 months (Group I), 1 year to 4 years (Group II), 4 years to 10 years (Group III), 10 years to 18 years (Group IV).
Data has been analyzed to calculate percentages by the statistical software SPSS (Statistical Package for the Social Sciences) Version 20.0. Armonk, NY: IBM Corp.
Results
In the current study incidences of various neoplasms were correlated with sex and age of the pediatric population. 106 patients were enrolled in the current study, out of which 71% were males 29% were females, maximum number of patients were in the age group III (4-10 years) of both sex. Second highest numbers of female patients were in age group II and males in group IV. Minimum numbers of patients were in the age group I (infants) (Figure 1).
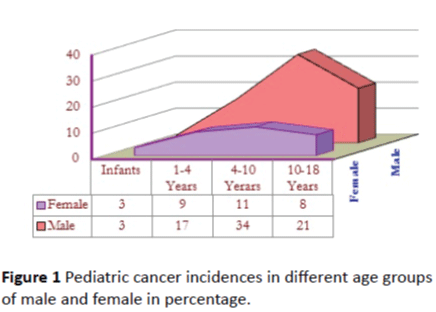
Figure 1: Pediatric cancer incidences in different age groups of male and female in percentage.
Data on incidences of different neoplasms with four age groups of both sexes (Figure 2) were analyzed by percentile and ranking statistics. Data showed that males (n=75, 71.4%) were more prone to cancer as compared to females (n=31, 28.5%). Acute Lymphocytic Leukemia was the most prevalent (n=46, 43%) type of cancer collectively in both sexes (45% in males and 38% in females), Hodgkin’s disease is the second most prevalent disease affects more than 11% of male population, while Germ cell tumor and Rhabdomyosarcoma were 5 percent. Whereas the incidences of other diseases were approximately similar in both sexes except Adenocarcinoma and Retinoblastoma which affect only female population as of B-Cell Acute Lymphoblastic Leukemia, Chronic Myelogenous Leukemia, Ewing's Sarcoma, Hepatoblastoma, Rhabdomyosarcoma, Synovial Sarcoma, and T-Cell Non- Hodgkin’s Lymphoma in males. Data also shows that the ALL relapse cases were more pronounced (66.6%) in males than females; conversely Acute Myelogenous Leukemia is more prevalent females (75%) than males. B-Cell Non-Hodgkin’s Lymphoma, Fibromatosis, Primitive neuroectodermal Tumor distributed equally in both sexes. Medulloblastoma and Osteosacroma were more prevalent in males (66.6%) than females, but Neuroblastoma was dominant (66.6%) in females. Maximum cases of ALL were seen in the age group III (4-10 years), inconsistent where most of the cases of ALL were reported in under the 5 years of age [5,6].
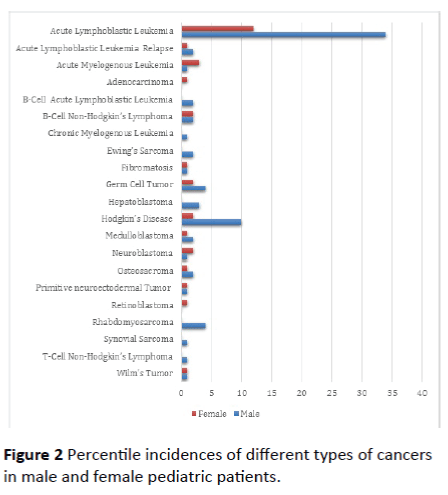
Figure 2: Percentile incidences of different types of cancers in male and female pediatric patients.
Discussion
In the current study male preponderance in male-to-female ratio was (M: F= 2.4:1) as already been reported [7,8]. The maximum numbers of cases were seen in the age groups III and IV in both males and females, which is in conformity with the earlier report [8,9]. However, the largest number of cases was seen in the age group III in male sex. This could probably be related to the general male dominance. The reason of the male preponderance is difficult to explain because no study proved the genetic or environmental factors contributing the male sex more vulnerable to different neoplasms [10,11].
Since 1970s nearly all the types of pediatric cancers have raised approximately 1 percent annually with the exception of Hodgkin’s disease. Central nervous system cancer has shown a significant increase of 25 percent whereas acute lymphocytic leukemia (ALL) up to 20 percent. Collective rate of all types of cancers found to increase 10 percent during the period of 1973 to 1991 in children of age less than 15 years. It is also suggested by some epidemiologist that increase in incidences of various pediatric cancers are due to the advancement in diagnostic procedures and reporting methods [8]. However this does not explain increase in all types of cancers in pediatrics. It is also noticed that, the incidences have increased but the death rate has decrease intensely due to marked improvement in early detection and treatment of cancer in USA. The incidence of pediatric cancer has increased in all ages but the significant increase was found ages between 10-14 years. In the current study Acute Lymphoblastic leukemia was the most frequent cancer found in, followed by Hodgkin’s disease which is consistent with the previous studies [12,13].
Involvement of genetics in cancer development has been discussed immensely over the years and now proved in various studies. Now a common consensus has developed that genetic makeup in the presence of environmental conditions trigger the uncontrolled cell division. Contribution of genetic factors in all cancers is only 5 percent but susceptibility is affected by rare mutations. Other genetic factors affect the metabolizing and detoxifying ability of various enzymes to repair the damage done by carcinogens [13,14]. Northern Europe study of twins concluded that maximum cancers were caused by environmental and behavioral factors like unhygienic and unhealthy life styles instead of genetic [15]. Another study on comparison of incidences of cancer in homozygous twins with heterozygous did not provide significant difference [16]. Some environmental factors like anticancer drugs, radiation, and diethylstilbestrol are well established causes of pediatric cancer. This chemical causes cancer in early age due to short latency nature, but some factors like ultraviolet exposure and tobacco smoke took long time to develop and appear in adulthood [17,18]. Multiple evidences suggested the role of different petrochemicals, organic solvents, pesticides, radio nucleoid, paint chemicals, electromagnetic radiations, heavy metals, hair colors used by mothers, alcohol consumption, coffee and tea [19,20]. Data suggested that children are more prone to some chemicals and radiation than adults [21,22].
Children exposed to various carcinogens from different routes through air, water and food.
It’s very difficult for government scientists and agencies to accurately quantify routine exposure to carcinogens. Children exposed more to these environmental carcinogens because of the fact they eat 4 times, drink twice, and breathe twice more than adults related to their body weight [23].
Conclusion
In the current study male preponderance in male-to-female ratio was (M: F= 2.4 :1) recorded. The maximum numbers of cases were seen in the age groups III & IV in both males and females. However, the largest numbers of cases were seen in the age group III in male sex. This could probably be related to the general male dominance. Acute Lymphocytic Leukemia was the most prevalent type of cancer found in this study.
9606
References
- Berrington de GA, Morton LM (2012) Converting epidemiologic studies of cancer etiology to survivorship studies: approaches and challenges. Cancer Epidemiol Biomarkers Prev21:875-880.
- Ross JA, Severson RK, Pollock BH, Robison LL (1996) Childhood cancer in the united states: A geographical analysis of cases from the Pediatric Cooperative Clinical Trials Groups. Cancer 77: 201–207.
- Robison LL, Hudson MM (2014) Survivors of childhood and adolescent cancer: life-long risks and responsibilities. Nat Rev Cancer14:61-70.
- Eden T (2010) Etiology of childhood leukaemia.Cancer Treat Rev36:286-297.
- Reulen RC, Winter DL, Frobisher C (2010) Long-term cause-specific mortality among survivors of childhood cancer. JAMA304:172-179.
- Friedman DL, Whitton J, Leisenring W (2010) Subsequent neoplasms in 5-year survivors of childhood cancer: the Childhood Cancer Survivor Study. J Natl Cancer Inst102:1083-1095.
- Ward E, DeSantis C, Robbins A, Kohler B, Jemal A (2014) Childhood and adolescent cancer statistics, 2014. CA: A Cancer Journal for Clinicians 64:83-103.
- Smith MA, Altekruse SF, Adamson PC, Reamon GH, Seibel NK (2014) Declining childhood and adolescent cancer mortality. Cancer
- Brunin GR (2004) Nongenetic causes of childhood cancers: evidence from international variation, time trends, and risk factor studies. ToxicolApplPharmacol 199:91-103.
- McNally RJ, Parker L (2006) Environmental factors and childhood acute leukemias and lymphomas. Leuk Lymphoma 47:583-598.
- Reis LA, Smith MA, Gurney JG (1999) Cancer incidence and survival among children and adolescents: United States SEER Program 1975–1995. Bethesda, MD: National Cancer Institute, SEER Program; 1999 (Report No. NIH Pub. No. 99-4649)
- Milne E, Greenop KR, Metayer C (2013) Fetal growth and childhood acute lymphoblastic leukemia: findings from the childhood leukemia international consortium. Int J Cancer 133:2968-2979.
- Bleyer A, Barr R, Hayes-Lattin B (2008) The distinctive biology of cancer in adolescents and young adults. Nature Reviews. Cancer 8:288-298.
- Berger AH, Pandolfi PP (2011) Cancer susceptibility syndromes. In: DeVita VT, Lawrence TS, Rosenberg SA, (eds.) DeVita, Hellman, and Rosenberg’s Cancer: Principles and Practice of Oncology (8thedn) 161–172.
- Rosana EN, Alexander R, Kristen G, Freddy S, James GS (2014) Environmental contributions to childhood cancers. J of Environmental Immunology and Toxicology 2: 86-98.
- Lichtenstein P, Holm NV, Verkasalo PK (2000) Environmental and heritable factorsin the causation of cancer-analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med 343:78-85
- Neri M, Ugolini D, Bonassi S (2006) Children’s exposure to environmental pollutants and biomarkers of genetic damage. II. Results of a comprehensive literature search and meta-analysis. Mutat Res 612:14-39.
- Bunin GR (2004) Nongenetic causes of childhood cancers: evidence from international variation, time trends, and risk factor studies. ToxicolApplPharmacol 199:91-103.
- Baan R, Grosse Y, Straif K (2009) A review of human carcinogens-Part F: chemical agents and related occupations. Lancet Oncol 10:1143-1144.
- Gilbert ES (2009) Ionising radiation and cancer risks: what have we learned from epidemiology? Int J RadiatBiol 85:467-482.
- Boice JD, Lauriston ST (2011) lecture: radiation epidemiology-the golden age and future challenges. Health Phys 100:59-76.
- Soto AM, Sonnenschein C (2010) Environmental causes of cancer: endocrine disruptors as carcinogens. Nat Rev Endocrinol 6:363-370.

