Keywords
Multiple sclerosis; Patient activity; Measurement devices; Gait pattern; Barefoot platform; Foot pathology.
Introduction
Multiple sclerosis (MS) is an autoimmune disease of the brain and spinal cord (central nervous system) when the immune system attacks the myelin cover of nerve fibres. MS affects more frequently the young working-age people. Neurological symptoms are progressing and can cause the disability. MS is on the fourth place after acute cerebral circulation disorders, epilepsy, and parkinsonism by prevalence among the neurological diseases of central nervous system. MS is on the second place after epilepsy in the young people [1,2]. Such symptoms as fatigue, pain, ataxia, weakness et al. often affect movement and cause the decreasing of the activity level [3]. Assessment and maintenance of the physical activity is a very important social problem. MS patients are significantly less active comparing with the healthy people even if they have non-significant impairments in the functional systems [4-6].
Monitoring of the physical activity was out of the neurologist’s attention during many years. However, the physical activity affects positively on the health of MS patients [7] and is the effective method of symptomatic therapy. Therefore it is very important to stimulate the activity of the MS patients [8-10]. Special rehabilitation complexes and actions including regular physical activity and training improve the physical status of the patient in achieving the optimal activity level without negative influence on the occurrence of the disease and on the course of exacerbations and symptoms development [11]. It is known also that more active life can decrease the risk of the MC in general [12].
Different questionnaires, walking tests, special devices with firmware (accelerometers, pedometers, gyroscopes etc). [3-12] are widely used in the health care and in the medical research [13,14] for the assessment of the physical activity now. Wireless devices and many smartphone applications can be used for the number of steps calculation. Number of steps is used often to estimate the distance or burned calories or other parameters [15].
Average daily activity of the MS patients and number of steps assessed with the portable accelerometers are in a good correlation with the gait parameters based on Six Minute Walk Test, 25-Foot Walk Test, and self-assessment of the physical activity [16-18].
The main feature of the up-to-date MS therapy is the individual approach to the patient. Interest to the monitoring of the individual load in the daily activity is tremendously increased the last years [8]. The efficacy of any method depends on the calculated parameters.
The purpose of this research was to demonstrate the possibility of the loading monitoring in the MS patients with a help of special measurement insoles and mobile application (both iOS and Android), allowing to calculate not only the number of steps, but also the total loading, contact time, foot contact areas, imbalance, and cadence.
Methods
Comparison of 2 patients with the same MS type and the same therapy was done. Both are males, differ by age and body mass index, with no disability (minimal disability in 2 functional systems (FS). Patients’ base-line characteristics are given in Table 1.
| Variables |
Patient no. 1 |
Patient no. 2 |
| Gender |
m |
m |
| Age |
27 years |
49 years |
| Height |
180 cm |
174 cm |
| Weight |
67 kg |
76 kg |
| BMI |
21 kg/m2 |
25 kg/m2 |
| MS type, therapy |
Relapsing-remitting MS Anti-B-cell therapy since September, 2017 (during 2 years) |
| Debut |
2014 |
2004 |
| Year of diagnosis |
2014 |
2017 |
| EDSS |
1.5 |
2.5 |
| Pyramidal |
1 |
2 |
| Cerebellar |
1 |
2 |
| Brainstem |
1 |
1 |
| Sensory |
1 |
1 |
| Bowel and bladder |
0 |
1 |
| Visual |
0 |
0 |
Table 1: Patient’s base-line characteristics.
• emed®, pedar®, and loadsol® measurement systems (novel gmbh, Munich, Germany www.novel.de) were used for examination of 2 MS patients.
• emed® platform provides pressure data under the foot (barefoot walking across the platform) for the foot function analysis and foot pathology diagnosis (frequency-25 Hz, resolution-2 sensors/cm2), five dynamic records of each foot were made with first step procedure.
• pedar® in-shoe pressure measurement system allows monitoring of the local loads between the foot and the shoe (frequency-50 Hz, 99 sensors per insole), 3 trials were done in walking along 20 m corridor.
• loadsol® system enables the measurement of the normal ground reaction force on the plantar surface of the foot in the footwear (frequency-100 Hz). Hindfoot and medial and lateral forefoot separately were captured. Nine hours measurement was carried out for monitoring the loading. The patients wrote the time interval with definite type of activity (outside walking, driving the car, being indoors etc.) in the diary.
The following parameters were calculated: emed® ? pedar® systems: peak pressure (kPa), maximum force (N), contact time (s) in concert with gait line analysis; emed® system: arch index; loadsol®: contact time (s), force-time integral (N*s), factor of imbalance, averaged body load over time (N), cadence (steps/ min), foot contact (over areas). Standard mask was used in emed® data analysis (hindfoot, midfoot, 5 metatarsal heads (MTH1- MTH5), big toe (T1), second toe (T2), and lateral toes (T345). Mask including hindfoot and medial and lateral forefoot was used in pedar® data analysis. Comparison with normal parameters (novel gmbh, Munich, Germany www.novel.de) was done for emed® system parameters. One factor ANOVA (p<0,05) was used for the parameters comparison. Maximum pressure pictures (MPP) for emed® data for both patients are given in Figure 1.

Figure 1: MPP for Emed® data for patients no. 1a and no. 2b.
Significantly different parameters (p<0,05) for left and right feet for both patients are given in Table 2.
| Variables |
Patient no. 1 |
Patient no. 2 |
Patient no. 1 |
Patient no. 2 |
| Foot areas |
Left |
Right |
Left |
Right |
Left |
Right |
Left |
Right |
| Peak pressure, kPa |
Maximum force, N |
| Hindfoot |
- |
- |
469 ± 12 |
375 ± 26 |
- |
- |
703 ± 26 |
627 ± 45 |
| Midfoot |
131 ± 41 |
178 ± 27 |
- |
- |
97 ± 24 |
146 ± 17 |
- |
- |
| MTH2 |
- |
- |
- |
- |
156 ± 11 |
178 ± 12 |
- |
- |
| Big toe |
- |
- |
- |
- |
126 ± 23 |
176 ± 42 |
- |
- |
| T345 |
- |
- |
171 ± 27 |
78 ± 24 |
- |
- |
34 ± 8 |
16 ± 6 |
Table 2: Significantly different parameters for left and right feet (p<0.05).
Patient no. 1: Significantly increased loading of the right midfoot may indicate on the development of longitudinal flat foot with time. However, it is no difference in the value of arch index (ratio of the midfoot contact area and foot contact area without toes) for left and right feet (0,20 ± 0,02 and 0,22 ± 0,02) now. Difference in MTH2 and big toe loading exists but does not influence on the symmetry of walking.
Patient no. 2: Significantly increased loading of left hindfoot and lateral toes testifies that left foot is a take-off foot and plays the bigger role in the weight bearing in the walking.
Discussion
To compare the parameters of examined patients with the normal left feet are mirrored to right feet. MPP for emed® data for both patients in comparison with normal are given in Figure 2. Significantly different parameters (?<0.05) compared with normal are given in Table 3.
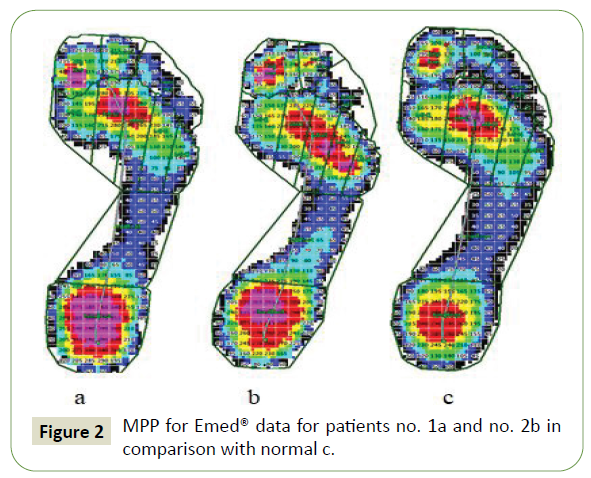
Figure 2: MPP for Emed® data for patients no. 1a and no. 2b in comparison with normal c.
| Variables |
Patient no. 1 |
Patient no. 2 |
Normal |
Patient no. 1 |
Patient no. 2 |
Normal |
| Contact time, ms |
| Foot areas |
658 ± 21 |
788 ± 42 |
928 ± 111 |
- |
- |
- |
| Peak pressure, kPa |
Maximum force, N |
| Hindfoot |
459 ± 66 |
422 ± 53 |
334 ± 80 |
575 ± 19 |
665 ± 53 |
493 ± 80 |
| Midfoot |
156 ± 40 |
176 ± 47 |
115 ± 46 |
- |
157 ± 39 |
121 ± 49 |
| MHT1 |
351 ± 175 |
- |
247 ± 137 |
- |
- |
- |
| MHT2 |
- |
270 ± 26 |
365 ± 132 |
- |
- |
- |
| MHT4 |
- |
330 ± 104 |
261 ± 86 |
|
152 ± 31 |
116 ± 37 |
| MHT5 |
129 ± 49 |
- |
230 ± 154 |
- |
- |
- |
| T1 |
- |
- |
- |
90 ± 88 |
197 ± 50 |
135 ± 62 |
| T2 |
- |
288 ± 50 |
171 ± 88 |
54 ± 19 |
46 ± 7 |
30 ± 16 |
Table 3: Significantly different parameters (p<0.05) compared with normal.
Contact time does not exceed the normal value. No difference is found in the loading of MTH3. Loading of the hindfoot is greater compared with normal? Therefore minimal impairments in the pyramidal and cerebellar FS do not cause noticeable disorder in the walking [19]. Increased loading of the midfoot (especially for Patient no. 2), loading shift to MTH1 with decreasing loading of MTH5 (Patient no. 1), or loading shift to MTH4 (Patient no. 2), increased loading of big toe or/and second toe are the results of foot deformities. Gait line course starts at the center of the hindfoot for both patients (normal loading of the hindfoot) and ends in the area of forefoot (Patient no. 1) because of increased loading of MHT1 and in area of big toe (Patient no. 2). MPP for pedar® data for both patients are given in Figure 3.
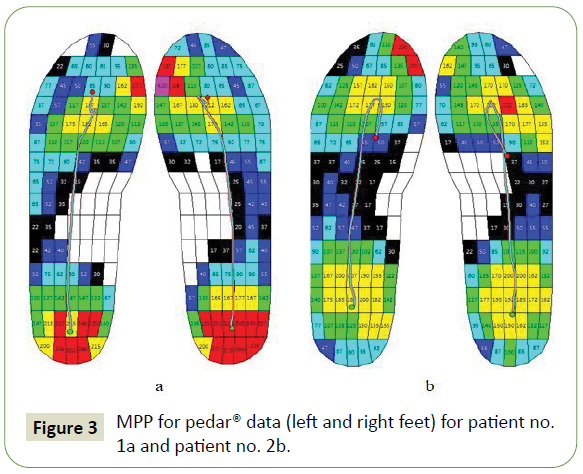
Figure 3: MPP for pedar® data (left and right feet) for patient no. 1a and patient no. 2b.
Absence of significant difference in the loading of left and right feet allow to mirror left feet to right feet for further analysis. MPP for in-shoe pedar® data (left feet mirrored to right feet) for both patients are given in Figure 4. Significantly (?<0,05) different parameters are given in Table 4.
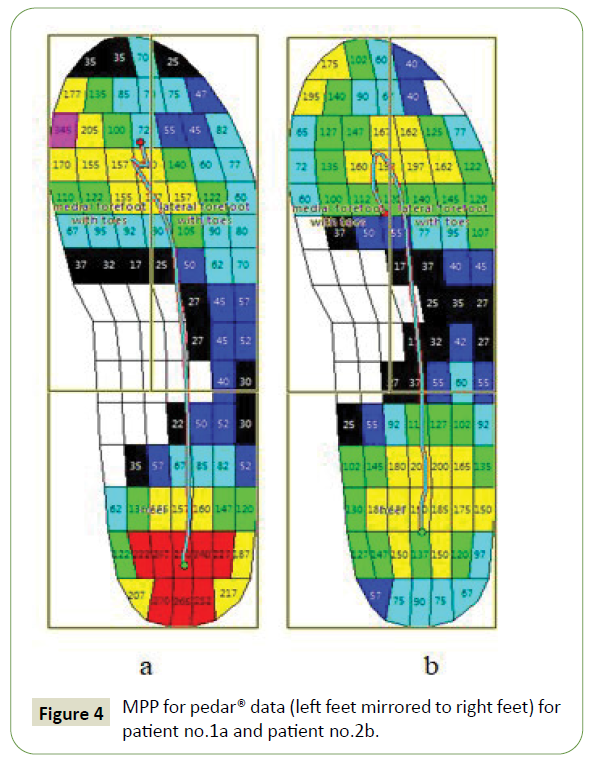
Figure 4: MPP for pedar® data (left feet mirrored to right feet) for patient no.1a and patient no.2b.
| Variables |
Patient no. 1 |
Patient no. 2 |
Patient no. 1 |
Patient no. 2 |
| Contact time, ms |
| Foot areas |
597 ± 37 |
639 ± 114 |
- |
- |
| Peak pressure, kPa |
Maximum force, N |
| Hindfoot |
278 ± 38 |
210 ± 36 |
- |
- |
| Medial forefoot |
357 ± 102 |
237 ± 43 |
422 ± 75 |
360 ± 58 |
| Lateral forefoot |
- |
- |
300 ± 70 |
367 ± 65 |
Table 4: Significantly (p<0, 05) different parameters.
Contact time is normal for both patients although significantly less for Patient no. 1. Loading of the hindfoot and medial forefoot is significantly greater for Patient no. 1 compared with Patient no. 2. At the same time lateral forefoot is loaded greater for Patient no. 2. In-shoe measurements correlate with barefoot measurements. Gait line changes the direction in the area of forefoot when toeoff should take place for Patient no. 2. This disorder in weight bearing can be a result of uncomfortable shoes. The results of the barefoot and in-shoe measurements allow to conclude that minimal impairments in FS should not limit the physical activity of the patients. Nine hours measurement of force for both patients is given in Figure 5.
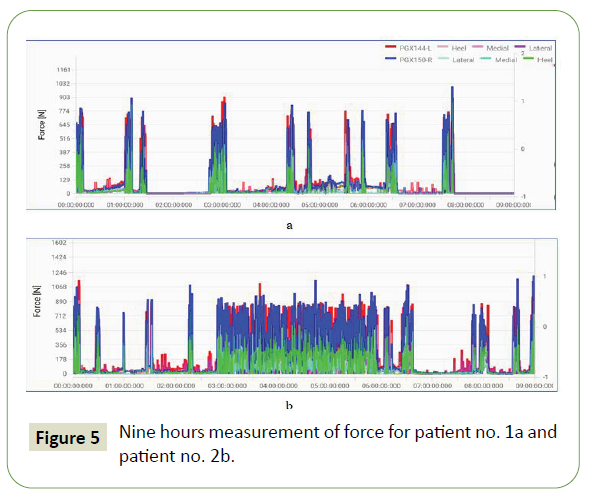
Figure 5: Nine hours measurement of force for patient no. 1a and patient no. 2b.
Patient no. 2 compared with Patient no. 1 has done more (1.75) steps. But his activity (force-time integral) is much higher (2.86). FOIB and contact time are greater. Greater loading of the left foot correlates with the results from emed® measurements (Table 5). The structure of foot contact (% of trials) is similar. Hindfoot contact is prevailed in the steps (68% and 77%).
| Parameters |
Patient no. 1 |
Patient no. 2 |
| Number of steps (left+right) |
5307 |
9271 |
Force-time integral, N*s  , where t- measuring time, in [s] , where t- measuring time, in [s] |
2385044,6 L* |
7064917,4 L |
| 2357116,8 R* |
6516990,4 R |
| 4742161,4 |
13581907,8 |
Factor of imbalance  , where FTIL, FTIR- force time integral of left and right insoles correspondingly, in [Ns] , where FTIL, FTIR- force time integral of left and right insoles correspondingly, in [Ns] |
0,01 L |
0,04 L |
| Contact time, ms |
756 L 791 R |
943 L 950 R |
| Foot contact (% of trials) |
- |
- |
| Hindfoot |
69 L 66 R |
72 L 82 R |
| Medial |
5 L 12 R |
10 L 8 R |
| Lateral |
9 L 9 R |
14 L 12 R |
| *L-left, R-right |
Table 5: Results of nine hours force measurement.
Three minutes interval was determined for each patient for the detailed analysis of walking and explanation why the activity of Patient no. 2 is almost 3 times higher compared with the activity of Patient no. 1. The results for three minutes interval of walking are given in Table 6.
| Parameters |
Patient no. 1 |
Patient no. 2 |
| Selected time interval (walking outside) |
00:03:12:360 |
00:03:12:500 |
| Number of steps (L + R) |
376 |
368 |
| Force-time integral, N*s |
136473,9 |
162068,7 |
| Factor of imbalance |
0,06 R |
0,04 L |
| Contact time, ms |
639 L 636 R |
653 L 639 R |
Cadence (steps/min)
Avg. Cadence [steps/min]=(Steps left+Steps right)*60/t |
114 |
116 |
Averaged Body Load over Time, in [N]  |
709,5 |
841,9 |
| Foot contact (% of trials) |
|
|
| Hindfoot |
100 L 100 R |
97 L 97 R |
| Medial |
0 L 0 R |
2 L 1 R |
| Lateral |
0 L 0 R |
4 L 4 R |
Table 6: Results for three minutes interval of walking.
No significant difference (p=0.98) was found in number of steps during the short period of walking, but activity (force-time integral) and averaged body load over time are slightly higher (1,19) for Patient no. 2. Non-significant difference exists also in the values of factor of imbalance, contact time and cadence. First contact with the surface starts with the hindfoot mostly (100% and 97% correspondingly). The activity becomes significantly higher with time for Patient no. 2 compared with the activity of Patient no. 1.
Conclusion
Application of up-to-date measurement devices and mobile application allows estimating the daily patient activity as well as the other parameters characterizing the gait pattern and its impairments. Functional diagnostics during barefoot platform measurements and influence of the shoes in in-shoe measurements give the opportunity to assume the limitation of physical activity in persons with MS.
36325
References
- Gusev EI, Boiko AN, Stolyarov ID (2009) Multiple sclerosis. Reference book Real Taim.
- Stolyarov ID, Belyaev AM, Votinsteva MV (2019) Multiple sclerosis. Monoclonal treatment. М.: Meditsina-Inform LLC.
- Klaren RE, Motl RW, Dlugonski D, Sandroff BM, Pilutti LA (2013) Objectively quantified physical activity in persons with multiple sclerosis. Arch Phys Med Rehabil 94: 2342-2348.
- Krüger T, Behrens JR, Grobelny A, Otte K, Mansow-Model S, et al. (2017) Subjective and objective assessment of physical activity in multiple sclerosis and their relation to health-related quality of life. BMC Neurol 17: 1-2.
- Balantrapu S, Sosnoff JJ, Pula JH, Sandroff BM, Motl RW (2014) Leg spasticity and ambulation in multiple sclerosis. Mult Scler Int 2014: 1-8.
- Dlugonski D, Pilutti LA, Sandroff BM, Suh Y, Balantrapu S, et al. (2013) Steps per day among persons with multiple sclerosis: Variation by demographic, clinical, and device characteristics. Arch Phys Med Rehab 94: 1534-1539.
- Motl RW, Snook EM, McAuley E, Scott JA, Douglass ML (2006) Correlates of physical activity among individuals with multiple sclerosis. Ann Behav Med 32: 154-161.
- Doerksen SE, Motl RW, McAuley E (2007) Environmental correlates of physical activity in multiple sclerosis: a cross-sectional study. Int J Behav Nutr Phys Act 4: 1-7.
- Gosney JL, Scott JA, Snook EM, Motl RW (2007) Physical activity and multiple sclerosis: validity of self-report and objective measures. Fam Community Health 30: 144-150.
- Motl RW, McAuley E, Klaren R (2014) Reliability of physical-activity measures over six months in adults with multiple sclerosis: Implications for designing behavioral interventions. Behav Med 40: 29-33.
- Halabchi F, Alizadeh Z, Sahraian MA, Abolhasani M (2017) Exercise prescription for patients with multiple sclerosis: Potential benefits and practical recommendations. BMC Neurol 17: 1.
- Dorans KS, Massa J, Chitnis T, Ascherio A, Munger KL (2016) Physical activity and the incidence of multiple sclerosis. Neurology 87: 1770-1776.
- Allet L, Knols RH, Shirato K, Bruin ED (2010) Wearable systems for monitoring mobility-related activities in chronic disease: a systematic review. Sensors 10: 9026-9052.
- Pedišić Ž, Bauman A (2015) Accelerometer-based measures in physical activity surveillance: current practices and issues. Br J Sports Med 49:219-223.
- Case MA, Burwick HA, Volpp KG, Patel MS (2015) Accuracy of smartphone applications and wearable devices for tracking physical activity data. JAMA 313: 625-626.
- Snook EM, Motl RW, Gliottoni RC (2009) The effect of walking mobility on the measurement of physical activity using accelerometry in multiple sclerosis. Clin Rehabil 23: 248-258.
- Weikert M, Motl RW, Suh Y, McAuley E, Wynn D (2010) Accelerometry in persons with multiple sclerosis: measurement of physical activity or walking mobility?. J Neurol Sci 290: 6-11.
- Weikert M, Suh Y, Lane A, Sandroff B, Dlugonski D, et al. (2012) Accelerometry is associated with walking mobility, not physical activity, in persons with multiple sclerosis. Med Eng Phys 34: 590-597.
- Petrov AM, Stolyarov ID, Shkilnyuk GG, Ilves AG, Mineev KK, et al. (2015) Time course of changes in the development of gait disorders in multiple sclerosis. Neurol Neuropsychiatry Psychosomatics 7: 27-32.

