Introduction
Nephrometry is a score used to stratify renal lesions into low, medium or high complexity, assisting the surgeon for the planning of conservative operations. Depending on the method of how the measures are made, we could generate a wrong score, limiting the reproductibility of the method (Table 1 and Figure 1).
| |
1 Pt |
2 Pts |
3 Pts |
| (R)adius (maximal diameter in cm) |
≤4 |
>4 or <7 |
≥7 |
| (E)xophytic/endophytic properties |
≥50% |
<50% |
Entirely Endophytic |
| (N)earness of the tumors the collecting system or sinus (mm) |
≥7 |
>4 or <7 |
≤4 |
| (A)nterior/Posterior |
No points given. Mass assigned a descriptor of a, p or x |
(L)ocation relative to the polar lines*
Suffix “h” assigned if the tumor touches the main renal artery or vein |
Entirely above the upper or below the lower polar line |
Lesion crosses polar line |
>50% of mass is across polar line (a) or mass crosses the axial renal midline (b) or mass is entirely between the polar lines (c) |
Table 1: Nephrometry score system.
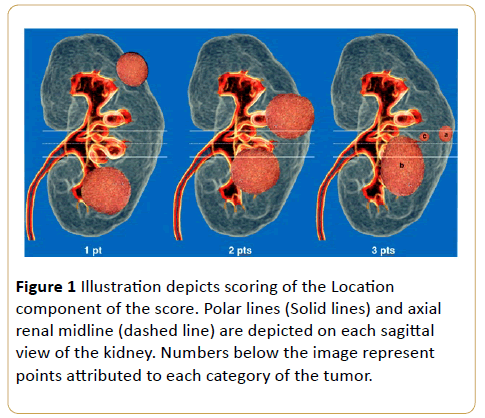
Figure 1: Illustration depicts scoring of the Location component of the score. Polar lines (Solid lines) and axial renal midline (dashed line) are depicted on each sagittal view of the kidney. Numbers below the image represent points attributed to each category of the tumor.
Materials and Methods
Images obtained by intravenous contrast enhanced computer tomography were utilized. The recommended protocol consists of unenhanced, arterial, nephrographic and excretory phases, after evaluation on at least two different perpendicular planes.
Results and Discussion
The nephrometry score is based on five parameters which characterize the anatomy of a solid renal mass. The term “RENAL” is utilized for better memorization of these parameters, as follow: “R” (ray): tumor’s greatest diameter; “E”: Endophytical/Exophytical properties of the tumor; “N”: proximity of the tumor’s deepest part to the renal collecting system (near); “A”: Anterior (A)/Posterior (P); “L”: Localization of the tumor and its relations to the polar lines. The suffix “x” is attributed to the tumor if its location is not well defined. An aditional “h” suffix is used to designate a hilar located tumor when there is contact with renal arteries or veins. Every component of the acronim, except for the letter “A”, is scored in a scale from 1 to 3.
Best axis to analyze the renal mass
Since the axial renal axis differs from the axial human body axis, an inattentive measure and application of the renal nephrometry protocol could lead to an inaccurate result.
Best axis to analyze the renal mass and the differences between abdomen and kidney axial axis is shown in Figures 2 and 3.
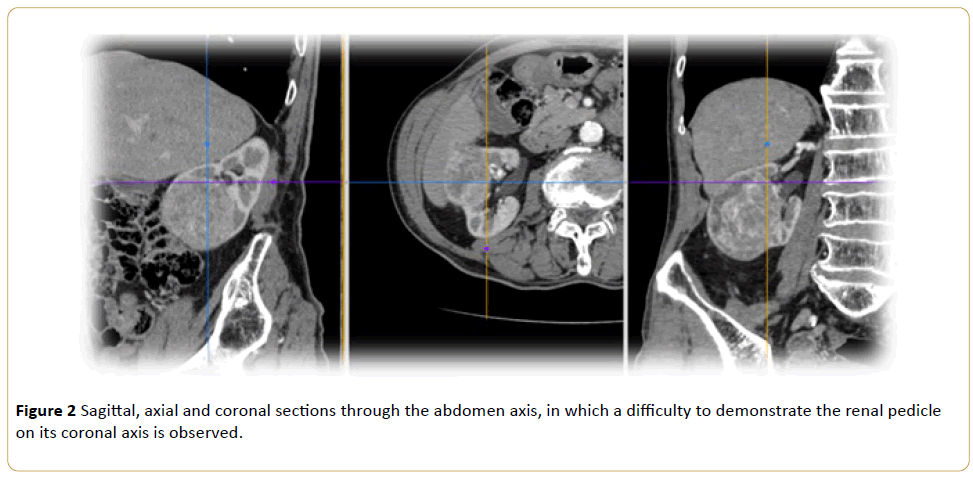
Figure 2: Sagittal, axial and coronal sections through the abdomen axis, in which a difficulty to demonstrate the renal pedicle on its coronal axis is observed.
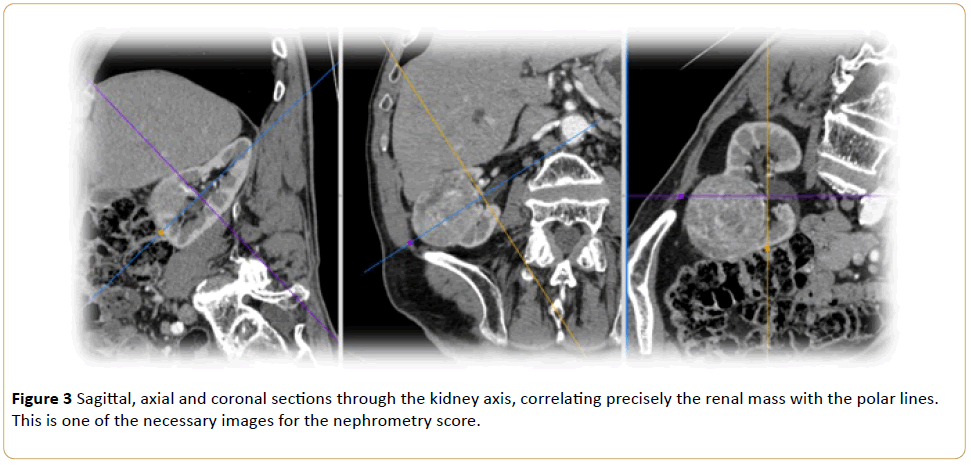
Figure 3: Sagittal, axial and coronal sections through the kidney axis, correlating precisely the renal mass with the polar lines. This is one of the necessary images for the nephrometry score.
The importance of the utilization of kidney related ortogonal planes is shown in Figures 4-6.
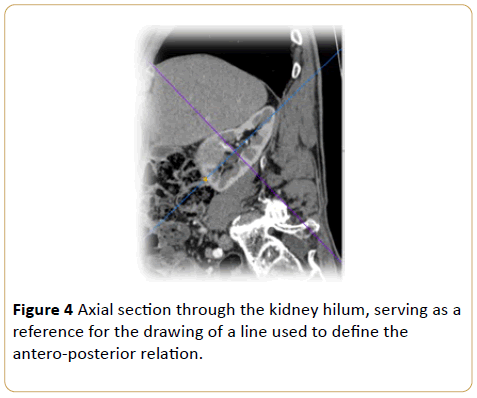
Figure 4: Axial section through the kidney hilum, serving as a reference for the drawing of a line used to define the antero-posterior relation.
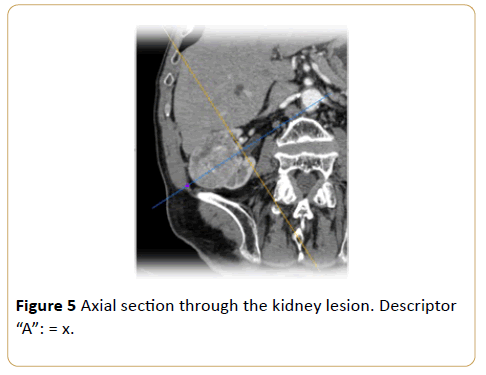
Figure 5: Axial section through the kidney lesion. Descriptor “A”: = x.
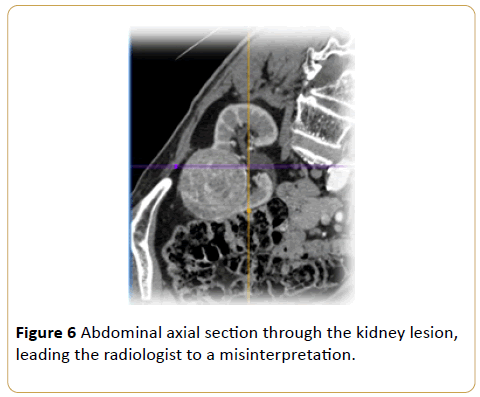
Figure 6: Abdominal axial section through the kidney lesion, leading the radiologist to a misinterpretation.
Multiplanar reconstruction visualization modes
During the evaluation of the renal mass, it is important to observe the visualization mode (MIP, MinIP, Average, Volume Rendering), because depending on the slice width during the post processing analysis, its measures could be underestimated (Figures 7-9).
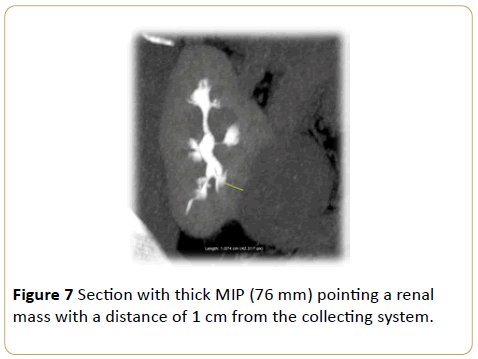
Figure 7: Section with thick MIP (76 mm) pointing a renal mass with a distance of 1 cm from the collecting system.
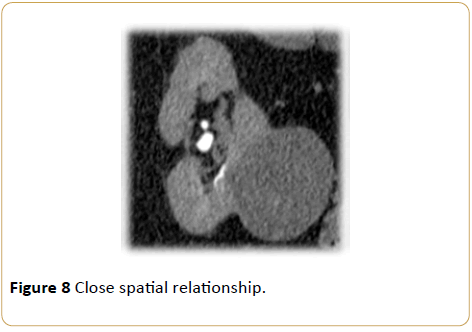
Figure 8: Close spatial relationship.
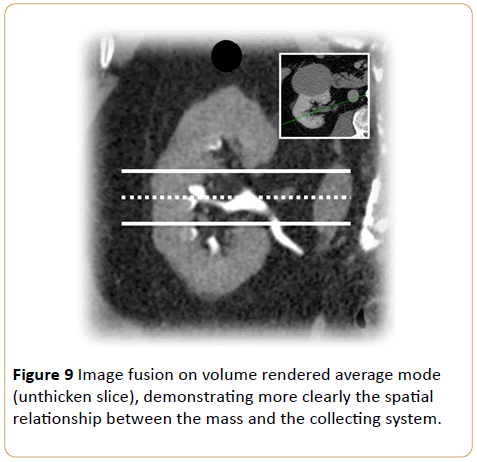
Figure 9: Image fusion on volume rendered average mode (unthicken slice), demonstrating more clearly the spatial relationship between the mass and the collecting system.
Polar and anterior/posterior meso renal masses
There is a difficulty in the anterior/posterior characterization (Figures 4 and 5), which corresponds to the descriptor "A", that represents polar masses. There might be also a difficulty to correlate the mass with the polar lines (Figures 10 and 11), as assigned in the descriptor "L", in meso renal anterior or posterior masses. This problem is given by the fact that one couldn't visualize the kidney hilum (reference image) and the renal mass in one image only to use the nephrometry protocol.
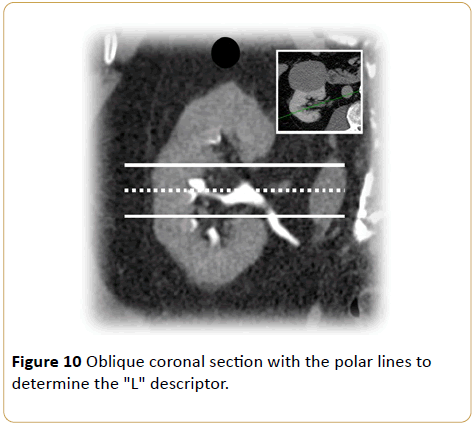
Figure 10: Oblique coronal section with the polar lines to determine the "L" descriptor.
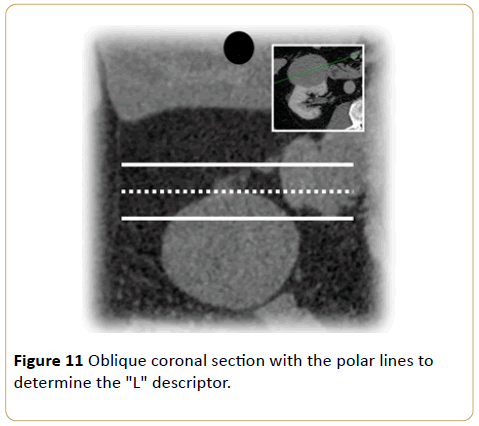
Figure 11: Oblique coronal section with the polar lines to determine the "L" descriptor.
The importance of the contrast enhanced phase
The administration of endovenous contrast media is recommended.
Two descriptors might be affected in this example: "R" - When the measure of the greatest diameter is made, an overestimation could easily be obtained in the unenhanced phase (Figure 12). During the evaluation of the enhanced phase (Figure 13), the close contact of the cyst (yellow arrow) with the mass (green arrow) can be perceived, since the contrast media gives a better definition of its limits. Another affected descriptor would be the "E" – after a line that represents the kidney contour (red arrow) is traced, a lesion that is < 50% exophytic (descriptor "E" = 1) during the unenhanced phase is noted (Figure 14).
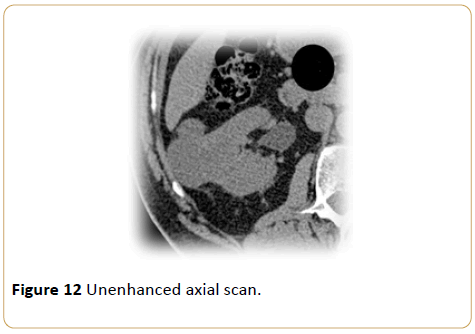
Figure 12: Unenhanced axial scan.
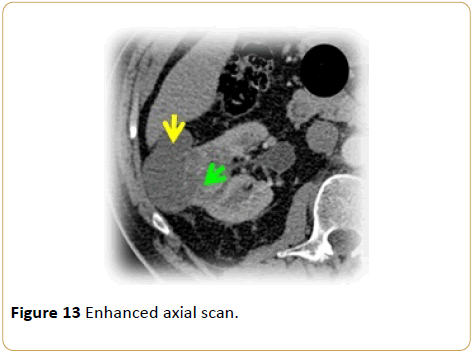
Figure 13: Enhanced axial scan.
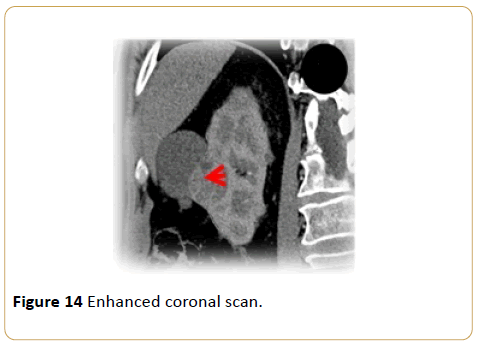
Figure 14: Enhanced coronal scan.
It is necessary that the images are acquired in a resolution good enough not to lose definition as the plane of study is changed, since there isn't a definitive plane for each descriptor, so every case should be evaluated on a single and individual basis. The use of MPR on swivel mode is suggested with the central point laying on the renal mass, and also the documentation of images in Volume Rendering (VR) that aids to correlate the mass, specially the polar lines (Figure 15).
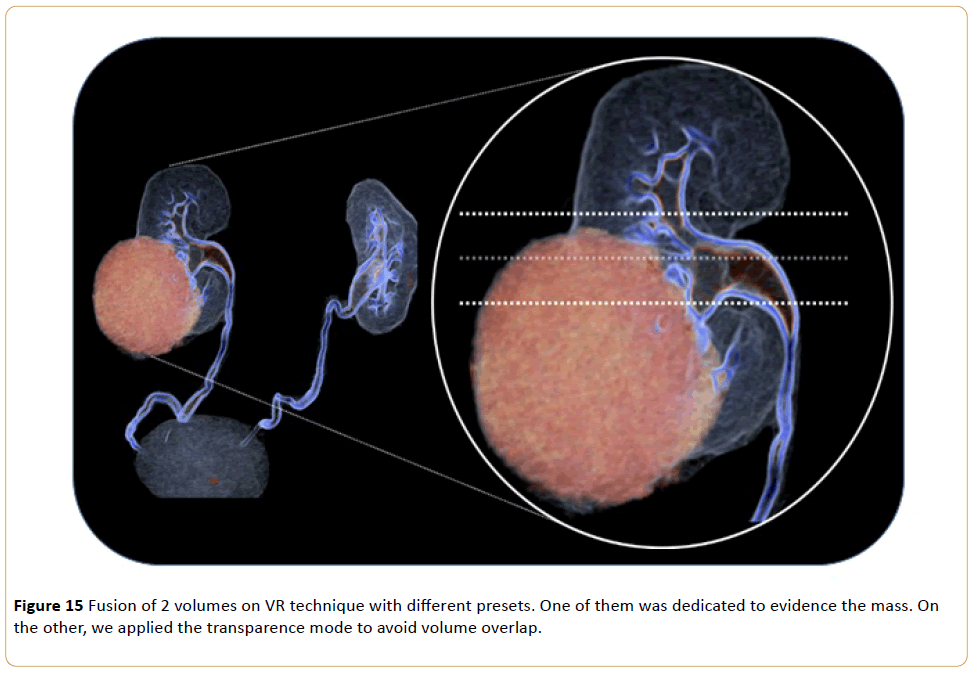
Figure 15: Fusion of 2 volumes on VR technique with different presets. One of them was dedicated to evidence the mass. On the other, we applied the transparence mode to avoid volume overlap.
Final result/documentation of the nephrometry score is seen in Figure 16.
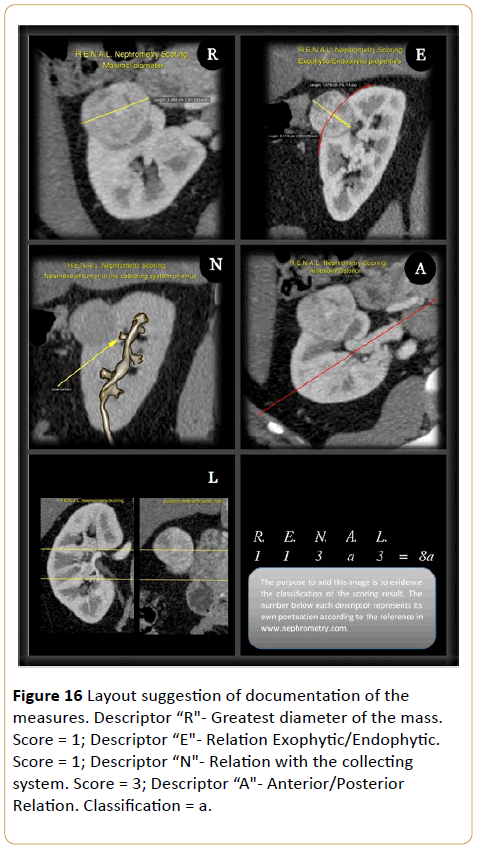
Figure 16: Layout suggestion of documentation of the measures. Descriptor “R"- Greatest diameter of the mass. Score = 1; Descriptor “E"- Relation Exophytic/Endophytic. Score = 1; Descriptor “N"- Relation with the collecting system. Score = 3; Descriptor “A"- Anterior/Posterior Relation. Classification = a.
Conclusion
Since its implementation, the R.E.N.A.L scoring system has been used to supply pre-nephrectomy information, predicting results in the long run [1-5].
Given the importance of the application of the nephrometry scoring system in the radiologist report, the responsible subject of these reconstructions has a fundamental role on the contribution to a more reliable report and should be careful not to induce a false diagnosis.
17373
References
- Parsons RB, Canter D, Kutikov A, Uzzo RG (2012) TheR.E.N.A.Lnephrometry scoring system: The radiologist’s perspective. AJR Am J Roentgenol. Setembro de 199:355–359.
- Kutikov A, Uzzo RG (2009) The R.E.N.A.Lnephrometry score: A comprehensive standardized system for quantitating renal tumor size, location and depth. J Urol. Setembro de182:844–853.
- Schmit GD, Thompson RH, Kurup AN, Weisbrod AJ, Boorjian SA, et al. (2013) Usefulness of R.E.N.A.L nephrometry scoring system for predicting outcomes and complications of percutaneous ablation of 751 renal tumors. J Urol. Janeiro de 189:30–35.
- Canter D, Kutikov A, Manley B, Egleston B, Simhan J, et al. (2011) Utility of the R.E.N.A.L nephrometry scoring system in objectifying treatment decision-making of the enhancing renal mass. Urology. Novembro de 78:1089–1094.
- R.E.N.A.LNephrometry Scoring System (2016)[homepage da internet]. Disponívelem: . Acessoem 10 mar 2016.

