Yang Liu1, Yan Hua1, Wang Bing2, Zhou Henghua3 and Guo Mei4
1Department of Gastroenterology, Shanghai Ninth People's Hospital, Shanghai Jiaotong University, School of Medicine, Shanghai, 200011, PR China
2Department of Surgery, Shanghai Ninth People's Hospital, Shanghai Jiaotong University, School of Medicine, Shanghai, 200011, PR China
3Department of Pathology, Shanghai Ninth People's Hospital, Shanghai Jiaotong University, School of Medicine, Shanghai, 200011, PR China
4Department of Iconography, Shanghai Ninth People's Hospital, Shanghai Jiaotong University, School of Medicine, Shanghai, 200011, PR China
*Corresponding Author:
Yang Liu
Department of Gastroenterology, Shanghai Ninth People's Hospital
Shanghai Jiaotong University, School of Medicine, Shanghai, 200011, PR China
Tel: 86-13301782257
E-mail: yang_241@aliyun.com
Received Date: October 13, 2016; Accepted Date: October 25, 2016; Published Date: October 31, 2016
Citation: Liu Y, Hua Y, Bing W, et al. Polymyalgia Rheumatica and Asthma Attack Presenting as the Initial Symptoms of Gastric Cancer. Ann Clin Lab Res. 2016, 4:4 doi: 10.21767/2386-5180.1000130
Keywords
Gastric cancer; Polymyalgia Rheumatica; Paraneoplastic symptom
Abbreviations
GI: Gastro-Intestine; MTX: Methotrexate; Hb: Haemoglobin; Alb: Albuminemia; CRP: C-Reactive Protein; LDH: Lactate Dehydrogenase
Background
Gastric cancer is a common disease in China as well as in the world. Patients with gastric cancer always have varied manifestations such as abdominal pain, anemia, gastrointestinal hemorrhage, weight loss, vomit, nausea and so on. But we also found some cases of gastric cancer who hasn't had any of these common symptoms of gastric cancer. Those non-specific manifestations or paraneoplastic presentation were varied a lot in gastric cancer, including dermatitis [1,2], polyarthritis [3], neuropathy [4], or kidney problems and so on. Doctors should pay more attention to those patients who couldn't get any effect from the treatments to their initial manifestations.
Case Presentation
A 51-year old female patient was hospitalized for intermittent fever, polymyalgia Rheumatica for three months, accompanied with asthma attack and abdominal mass for 2 weeks. She had abdominal surgeries for appendicitis and abdominal trauma in her teenage, and was well until April 30 2009, when she was first at the out-patient department for pain involving in bilateral wrists, elbows, knees and shoulder joints with intermittent high fever over 39°C. She was admitted to hospital as" polymyalgia Rheumatica" and the lab tests showed anemia of hemoglobin (Hb) 87 g/L, hypoalbuminemia (Alb: 20 g/L), C-reactive protein (CRP) 75.9 mg/L, lactate dehydrogenase (LDH) 269 U/L, no other serum values abnormal were found. She had been treated with prednisone, MTX and folic acid for 2 months but turned out without any relief of her symptoms. She underwent abdominal pain with vomit when she was still in the hospital, and was diagnosed as small intestinal obstruction. She also underwent upper GI endoscopy, a mucosa lesion on the lesser curve of the angulus was found, and the specimen for biopsy were only found to be nothing serious but erosive inflammation. 2 weeks before hospitalization of this time, she went through abdominal pain and episodic asthma-like attack and with the un-relieved multi-joints pain. Because of an acute flare-up of her arthritis and refractory cough with higher fever, as well as an abdominal mass in her lower right quadrant, she was readmitted to hospital in July 2009. By then she had been treated with prednisone for three months, and had lost her weight of 10 kg. A mass of 3*3 cm was found at her right lower quadrant, with clear line and light-tenderness, scars at middle and the right lower abdomen were also found on PE. No any redness or swelling of joints involved was found. The chest CT showed bronchiectasis at inferior lobe of left lung, accompanied with infection. Lab results: the blood hemoglobin level was 87 g/L to 95 g/L, erythrocyte sedimentation rate (ESR) 136 mm/h, serum albumin level was 24 g/L, the ratio of albumin vs globulin was 0.6, and serum protein electrophoresis showed a total protein concentration of 64 g/L, (A47.9%, α2 12.7%, γ25.4%). CRP was 75.9 mg/L. The results of rheumatoid factor and antinuclear factor were negative. CEA, CA19-9, AFP were normal and CA-125 27.54 U/ml. X-ray films of the patient's hands, elbows, shoulders, ankles and knees were normal. She received abdominal ultrasound examination and endoscopy of whole GI once again. The ultrasound showed a low-echo mass of 20*17*18 mm in the left lobe of liver which indicating an enlargement of lymph node. Upper GI endoscopy found a lesion on the lesser curve of gastric angulus with white-like changes around the basement (Figure 1), multiple pieces of biopsies were made for the histopathologic diagnosis and turned out to be poorly-differentiated adenocarcinoma. Colonoscopy found protrusion on the ileocecal valve, but no mucosa lesion (Figure 1). Reproductive ultrasound showed a uterine myoma and an adhesive mass of the right adnexa uteri. Consulted by doctors from general surgeon and gynecology, the patient underwent radical gastrectomy with D2 lymph node dissection and complex of intestinal adhesion release. In the process, a 1.5 cm-long ulceroinfiltrative lesion involving the muscular layer was found, but the omentum and liver revealed negative. The severe intestinal adhesion found in the surgery was thought to be the cause of her intestinal obstruction. The mass at the right lower quadrant abdomen was found to be a adnexa uteri cyst. The postoperative histopathological analysis revealed poorly-differentiated stage IIb (pT2N2M0) adenocarcinoma, cancerous thrombosis was seen in vessels (Figure 2).
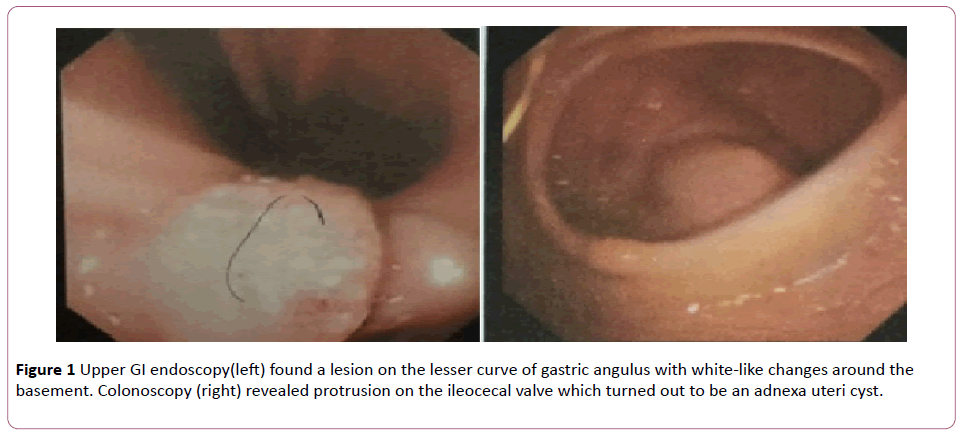
Figure 1: Upper GI endoscopy(left) found a lesion on the lesser curve of gastric angulus with white-like changes around the basement. Colonoscopy (right) revealed protrusion on the ileocecal valve which turned out to be an adnexa uteri cyst.
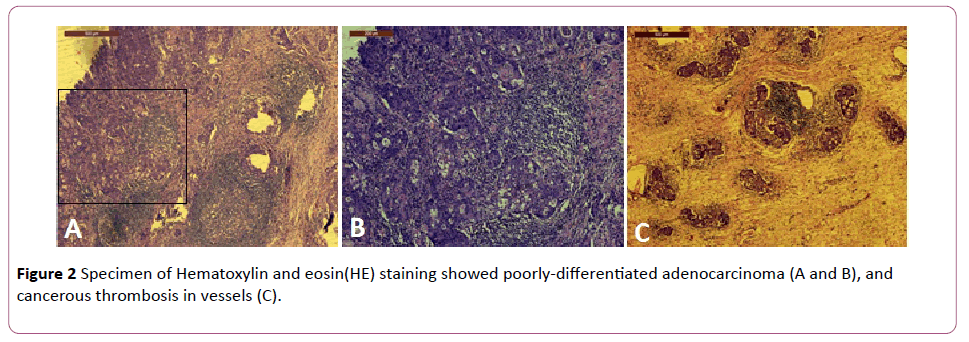
Figure 2: Specimen of Hematoxylin and eosin(HE) staining showed poorly-differentiated adenocarcinoma (A and B), and cancerous thrombosis in vessels (C).
One week later, the arthritis and the asthma-like attack related to the bronchiectasis infection dramatically resolved. She was discharged with blood hemoglobin level at 9 g/L, then she received 6 times of continuous chemotherapy of FOLFOX4, and has been followed up for more than 5 years in the outpatient department and lately had a thorough examination which showed that everything was well. She has never had flare-up of polyarthritis or asthma-like attack again during the whole follow-up. She gained weight and her blood hemoglobin level was up to 120 g/L. Repeated upper GI endoscopy showed no abnormality in the gastric remnant (Figure 3). CT scan and chest X-ray showed no abnormality either (Figure 4).
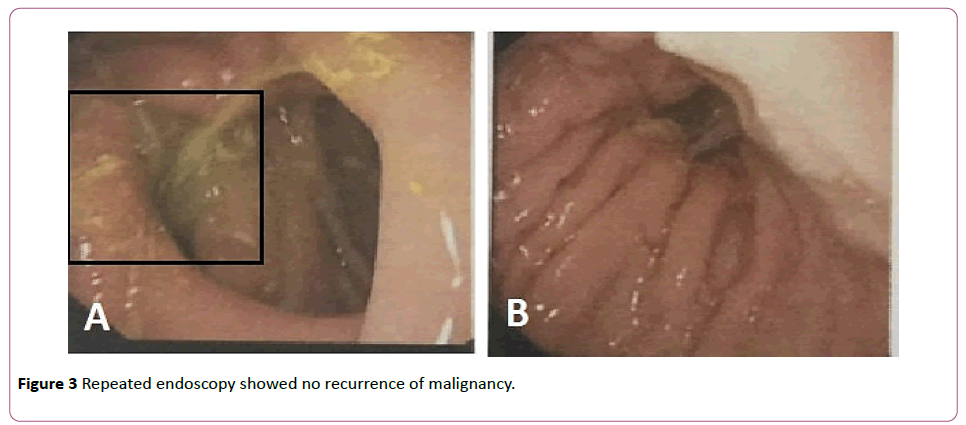
Figure 3: Repeated endoscopy showed no recurrence of malignancy.
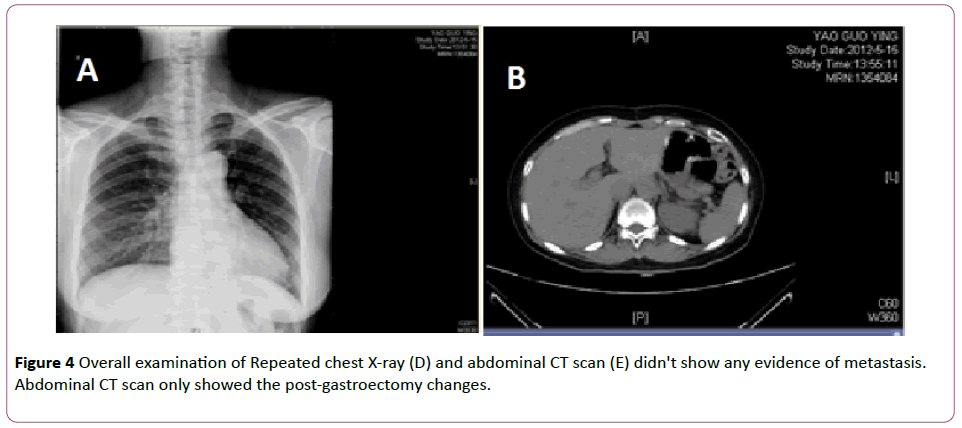
Figure 4: Overall examination of Repeated chest X-ray (D) and abdominal CT scan (E) didn't show any evidence of metastasis. Abdominal CT scan only showed the post-gastroectomy changes.
Discussion
This patient was totally relieved off her polymyalgia Rheumatica and her asthma-like attack, and never had another attack during the whole follow-up. After more than 5 years, she remained well which could also excluded the possibility of metastatic lesions of bones and lungs. Gastric cancer is the second leading cause of cancer-related mortality and the fourth most common cancer globally [5]. Gastric cancer has varied symptoms, patients of gastric cancer went to the doctor mostly for gastrointestinal related-symptoms, but there were still some patients didn't have any typical GI symptoms. Our patient's polymyalgia Rheumatica and asthma relieved totally after the surgery, which also might indicate all the symptoms were paraneoplastic symptoms of the gastric cancer, when the cancer removed, they never came back.
We reviewed the reports of paraneoplastic symptoms of gastric cancer and found the symptoms varied a lot and involved in the whole body, mostly were dermatitis, polyarthritis, neuropathy and kidney problems [6]. And among these cases [6,7], only one case had positive result of RF, one case presenting with kidney problem as initial manifestation as well. Polymyalgia Rheumatica was the popular one among these paraneoplastic symptoms, and NSAIDs took no effect in any of these case, all the symptoms relieved only after surgeries. This was also what we had in this case. But no any case of gastric cancer presenting with asthma-like symptoms was reported like what we had in this case. We presumed that the paraneoplastic symptoms were related to the mast cells (MC). MC accumulates in the tumor microenvironment and is associated with the prognosis in aggressive cancers [8]. Mediators derived from MC are stored in cytoplasmic granules include histamine, neutral protease, heparin proteoglycans, and cytokines such as TNF-α. And in this case, we think the asthma-like attack and the polyarthritis are all inflammatoryrelated reaction which could be the results of histamine and its receptors. When the cancer was removed, the cancer-related paraneoplastic symptoms were relieved simultaneously and patient never had another attack.
Doctors should consider the possibility of the underlying carcinoma in the patients who had refractory polyarthritis or asthma or kidney problems as well. Those patients should be given the endoscopy examination and further examinations when it's necessary. Multiple tools including NBI, LSCM and EUS were needed sometimes to go for a specific diagnosis. And in some cases, repeated endoscopy with biopsies was also necessary because of the high possibility of conceal lesion in those cases.
Conclusion
The rare manifestations of gastric cancer are non-specific, which makes it difficult for us doctors to come to the diagnosis of gastric cancer. So, we should give careful examinations to those patients with atypical symptoms, and those who could not get benefit from the anti-arthritis or treatments preventing asthma-attack, we should give the GI endoscopy to exclude the underlying malignancy of stomach.
Consent
Written informed consent was obtained from the patient for the publication of this report and any accompanying images.
Authors' contributions
YH, YL performed endoscopic procedures; GM performed the iconography; YL managed the patient; WB performed operation for the patient; ZHH managed the pathological diagnosis. YL wrote the manuscript and WB reviewed it. All authors approved the final manuscript.
Acknowledgements
The study was supported by Shanghai Ninth People's Hospital Foundation (2010-25).
17315
References
- Kubicka-Woowska J, Dbska-Szmich S, Lisik-Habib M, Noweta M, Potemski P (2014) Malignant acanthosis nigricans associated with prostate cancer: a case report. BMC Urol 14: 88.
- Robert M, Gilabert M, Rahal S, Ries P, Raoul JL (2014) Bazex syndrome revealing a gastric cancer. Case Rep Oncol 7: 285-287.
- Kurihara Y, Oku K, Suzuki A, Ohsone Y, Okano Y (2012) A case of calcinomatous polyarthritis presenting rheumatoid arthritis-like polyarthritis as the initial symptom of gastric cancer. Nihon RinshoMeneki Gakkai Kaishi 35: 439-445.
- Choi HS, Kim DH, Yang SN, Sung HJ, Choi SJ (2013) A case of paraneoplastic vasculitic neuropathy associated with gastric cancer. Clin Neurol Neurosurg 115: 218-221.
- Ang TL, Fock KM (2014) Clinical epidemiology of gastric cancer. Singapore Med J 55: 621-628.
- Jiang JH, Chen LD (2002) Misdiagnosis of gastric cancer in 5 cases with joints pain and nephropathy as the initial presenting symptoms. Chinese general practice 5: 322.
- Papagoras C, Kountouras J, Brilakis S, Chatzopoulos D, Zavos C, et al. (2007) Rheumatic-like syndrome as a symptom of underlying gastric cancer. Clin Rheumatol 26: 1029-1031.
- Dalton DK, Noelle RJ (2012) The roles of mast cells in anticancer immunity. Cancer Immunol Immunother 61: 1511-1520.


