Keywords
Otologic emergencies, Prevalence, Prognostic profile, Low resource Country
Introduction
Emergencies are sudden serious events requiring immediate action to avert grave consequences. However, that definition may not subsist in other forms described as otologic emergencies in oto-laryngologic practice. Most often, the anxiety exhibited by sufferers, because of the air of uncertainty, is responsible for such classifications, for example, in clinical conditions as an inert bead in the ear; however, in cases of facial nerve palsy, it is the disfigurement which poses the psychological alarm to the victims [1]
Emergency service is an integral part of any discipline of clinical medicine and it is considered as an indicator of quality of healthcare system [2]. Foreign bodies in the airway, ear, nose and throat have been found to be most common oto-laryngologic emergency in children in Tropical Africa [3] whereas, upper airway obstruction was found to be the commonest in the Geriatric age group [4].
Literature on the subject is scant, it is in this light the authors present the prevalence and prognostic profile of otologic emergency in our environment and suggest ways of curtailing them.
Methods
The case files and operation notes were collected and studied for detailed clinical information, investigations, diagnosis, complications and management outcome of otologic emergencies seen over a 3-year period, January 1, 2003-December 31,2005 in the Department of Oto-Rhinolaryngology, Head and Neck Surgery (ORL, HNS Dept), University College Hospital, Ibadan, Nigeria. Retrieval of case notes was from the health record’s database according to standard codes as contained in the International Classification of Diseases (ICD-10) version 10. Cases of sudden hearing loss were confirmed by pre- and post treatment Pure Tone Audiometric (PTA) and Tympanometric values. Those with PTA threshold values less than 25dB were excluded from the study. Cases with multiple otologic emergencies had one principal symptom utilised to generate data in order to have both internal and external validity.
All cases of HIV were those confirmed by the Westernblot method while only fungal agents cultured on Sabouraud’s Dextrose agar at between 27-30°C [5] were included in the study. High resolution CT-scan including clinical assessments confirmed intracranial complications of CSOM and longitudinal temporal bone fractures while CSF confirmation was basically clinical. Tympanic membrane perforations were evaluated by the use of the Video-otoscope, facial nerve paralysis was by clinical assessment while diagnosis of glomus tumors was by Histo-pathologic reports.
The results were collated and analysed by the IL, Chicago, SPSS 16.0 and presented by simple descriptive format, tables and diagrams.
The study observed the Helsinki declaration
Results
There were 231 Otologic emergencies (OE) of the 346 Otolaryngologic emergencies. This constitutes 66.8% and 22.5% of Oto-laryngologic emergencies and ENT consultations, respectively. This was followed by Rhinologic 52 (15.0%), the pharyngeal 8.5%, Laryngeal 6.4% and esophageal 3.3%. Males were 113 (48.9%) and 118 (51.1%) females, this gives a slight female preponderance. Their ages ranged from 2 weeks-101 years with a mean age of 29.4 ± 22.3 yr. There appears to be an inverse relation of occurrences of Otologic emergencies with age. The age group 0-10yrs had the highest 58 (25.1%) while those above 65yrs were 26 (11.3%) among the least (Figure 1).
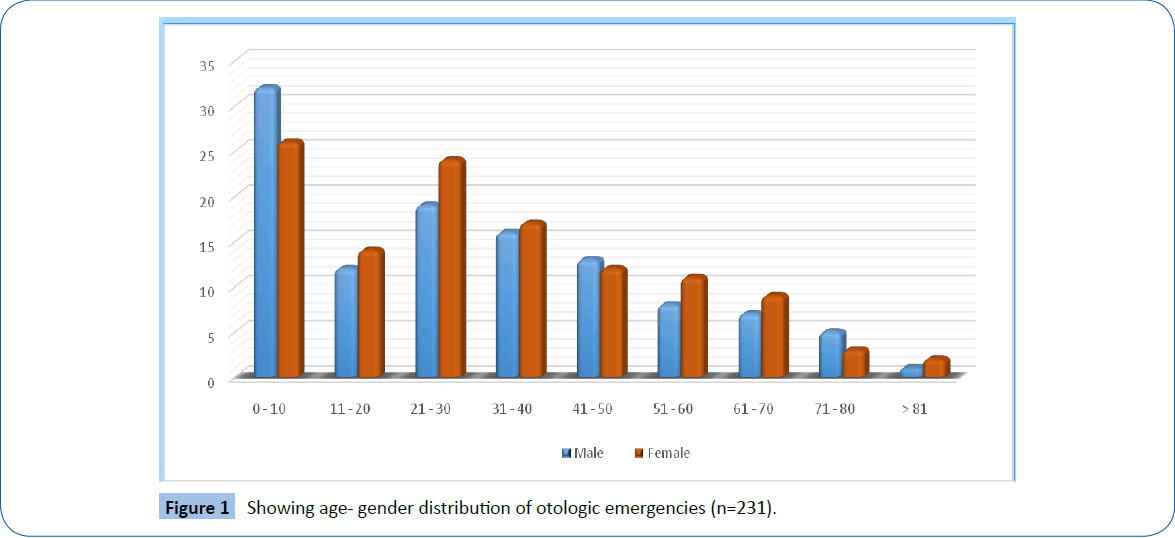
Figure 1: Showing age- gender distribution of otologic emergencies (n=231).
Bloody otorrhoea was the most common presentation with 94(40.7%). Of this, 39(37.9%) which constitute 1.0% of Otolaryngologic consultations, were from domestic violence (slaps) leading to tympanic membrane(TM) perforation (Tables 1). Among these, 28 (12.1%) were adult females, 9 (3.9%)-children and 2 (0.9%) were adult males implying 94.9% of victims being women and children. Thirty (76.9%) of these were left sided whereas 9 (23.1%) were right sided (Table 2). A total of 61(26.4%) had acute otitis media (AOM) of which 45 (73.2%) were children. Forty-five (19.5%) were cases of Road Traffic Accident (RTA) with lateral skull base fracture and Cerebrospinal Fluid leak (CSF leak). Satisfactory resolution was recorded in 30 (13.0%) leaving fifteen (6.5%) with residual morbidities ranging from unstable gait, hearing impairment, tinnitus amongst others. The study had 23 cases (10.0%) with vertigo in which 11 (4.8%) were cases of Benign Positional Paroxysmal Vertigo (BPPV) while Meniere’s disease had 9 (3.9%). There was an interesting case of Otolithic crisis of Tumarkin, first to be reported in our environment. There was a persistence of symptoms in 5 (2.2%) despite all manoeuvres and therapies though surgery was not embarked upon. There were 16 (6.9%) cases of facial nerve palsy of which 5 (2.2%) were cases of HIV/AIDS and 2 (0.9%) were fatal cases of malignant otitis external. In these, a 21/2 year old male child had severe protein energy malnutrition while the other, an elderly male with poorly controlled type 2 diabetes mellitus. There was an interesting case of a 27 year old male that had a partially amputated left ear following an assault at a political rally. The sharp cut came from anterior part of the tragus, the parotid gland and severed the external auditory canal at near the junction of the cartilaginous and bony parts. Symptoms of facial nerve palsy became manifest 72 hr post repair. He developed Frey’s syndrome, subsequently. Seven had persisting House-Brackmann’s grade II palsy. Fifteen (6.5%) had sudden hearing loss, including a 55 year old woman that had a spontaneous sudden bilateral sensorineural hearing loss (SNHL). An urgent Random Serum plasma glucose level was 536 mg/dl (29.8 mmol/l). The otologic symptoms regressed within a week of commencement of anti-diabetic regimen. In the rest, 6 (2.6%) were due to bilateral impacted cerumen auris, 3 (1.3%) from otomycosis, 3 (1.3%) idiopathic sudden unilateral SNHL and 2 (0.9%) were found to be reactive for HIV antibody.
| Ear Emergencies(EE) |
No |
Percentage(%) |
| Acute otitis media |
61 |
26.4 |
| Lateral skull base# & CSF leak |
45 |
19.5 |
| TM perforation from slaps |
39 |
16.9 |
| Vertigo |
23 |
10.0 |
| Facial nerve palsy |
16 |
6.9 |
| Sudden hearing loss |
15 |
6.5 |
| Mastoid abscesses |
10 |
4.3 |
| Bleeding from CSOM |
5 |
2.2 |
| FB in middle ear |
5 |
2.2 |
| Intracranial complications of CSOM |
5 |
2.2 |
| Glomus tumours |
4 |
1.7 |
| Otogenic tetanus |
3 |
1.3 |
| Total |
231 |
100.0 |
| NB: Bloody otorrhoea=2+3+7+8 above=45+39+5+5=94 |
Table 1: Distribution of Otologic emergencies n=231.
| Side |
Male |
Female |
Total |
Percentage(%) |
| Right |
3 |
6 |
9 |
23.1 |
| Left |
8 |
22 |
30 |
76.9 |
| Total |
11 |
28 |
39 |
100.0 |
| % |
28.2 |
71.8 |
100.0 |
|
| Distribution by side and gender n=39 |
Table 2: Showing traumatic TM perforation from slaps.
The study recorded 10 (4.3%) cases of mastoid abscesses and 5 (2.2%) cases of foreign body (FB) in the middle ear cavity of which 2 were cases of alkaline batteries. All were removed under general anaesthesia via a Wilde’s approach. All 3 (1.3%) cases of otogenic tetanus expired during treatment due to late presentation including 2 (0.9%) cases of intracranial complications of chronic suppurative otitis media (CSOM)-Meningitis and cerebellar abscesses with obstructive hydrocephalus. The case of meningitis was a 39 year old medical practitioner that succumbed to the disease shortly on admission into the Accident and Emergency.
There were 4 (1.7%) cases of middle ear tumours (glomus tumours) who expired also due to Oldring and Fisch type D disease. The overall morbidity was 27 (11.7%) and a cohort fatality of 11 (4.8%).
Discussion
Prevalence of 22.5% of Otologic emergencies is quite significant bearing in mind that this invariably would affect hearing. Learning and speech development in children are a product of satisfactory hearing while in adults would affect their socioeconomic development. It has been estimated that 80% of jobs are communication based. A similar prevalence was reported in a study [6] with no clear explanation.
A cohort fatality rate of 4.8% of Otologic emergencies in this study is also worthy of note. High mortalities were associated with intracranial complications of CSOM, malignant otitis external and advanced middle ear tumors all of whom succumbed from the diseases. Similar findings have been reported by other researchers [7,8]. Furthermore, a morbidity of 11.7% recorded in this study is also worth noting as hearing loss has been referred to by some researchers as a ‘hidden handicap’ and ‘internal deformity’ [6]. The middle ear cavity is a biconcave disc with a volume of 1-2 cubic centimetres that contains the multiplier mechanism for hearing- the ossicles. This is surrounded by vital structures that include; the roof, formed by the tegmen tympani (a thin bone that separates it from the brain), floor-the jugular bulb, anteriorly-the carotid wall that houses the internal carotid artery and eustachian tube opening, medial wall-the labyrinth and the fallopian canal which houses the facial nerve, posteriorly the aditus ad antrum while the lateral wall-Tympanic Membrane (TM) [9,10]. Any pathologic process affecting the middle ear space has the potentials of involving these surrounding structures and even worse if unattended to promptly.
A female preponderance of OE has been reported [6] of which the researchers speculated that the male gender being opt to delay in seeking medical attention thus presenting only when complications set in. This is particularly observed in the developing countries, probably due to several competing interests. This is confirmed in this study where three of the five mortalities were seen in adult males including an unfortunate medical doctor. He died shortly after admission into the casualty of meningitis that complicated CSOM.
Various authors documented the age bracket 0-10 yr as the most commonly involved in acute otitis media [11,12]. In this study, we had similar findings as most of the OE 58 (25.1%) were from that age-group of which 73.2% were cases of acute otitis media. Severe nature of otalgia experienced in AOM is commonly the main reason for presenting. The International Association for the Study of Pain (IASP), as accepted by the American Pain Society defines pain as an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage’. In the seventeenth century, Rene Descartes, a French philosopher and Mathematician proposed that the human body works like a machine that can be studied by scientific methods and that injury activates certain specific pain receptors and fibres that project to the brain. He further postulated that the intensity of pain is directly related to the amount of associated tissue injury’ [13]. The peculiar anatomy of the Eustachian tube, forceful feeding and recurrent respiratory tract infections have been implicated in children. Furthermore, malnutrition, parasitic infestation and the HIV/ AIDS pandemic have been found to contribute immensely to the rise in incidence [14,15].
The sight of blood from any part of the human body is usually terrifying which explains bloody otorrhoea (n=94, 40.7%) the commonest presenting symptom of OE. One of the leading causes was from slaps secondary to domestic violence (n= 39, 37.9%). The preponderances of women and children as victims which constitute 94.9% worth emphasis as they represent the vulnerable group in the society. The frequent involvement of the left side, further agrees with our argument in favour of slaps as the aetiology of the perforations of tympanic membrane. This is true, as 91% of the society are right handed [16]. Lou et al. [17] reported similar findings. This is a picture depicting societal violence against women and children which still exist despite the Geneva convention for the protection of their rights [18,19]. Spontaneous healing of the tympanic membrane perforations via conservative methods with strict avoidance of any form of otic drops usage was the treatment modality observed. The spontaneous healing rate was 91.2% while the average healing time was 40 ± 10 days as evaluated by the Video-otoscope. Those that had delayed healing were a result of otitis media following self-medication with ear drops before presentation. Satisfactory spontaneous healing has also been reported by various authors [17]. New methods of traumatic tympanic membrane perforations regeneration technique using gelatin sponge patch, gelfoam patch soaked in basic Fibroblast Growth Factor (bFGF) after edge approximation, in order to reduce healing rate and overall healing time has been described [20,21].
Worthy of note is the high number of cases of lateral skull base fracture with CSF leak from commercial motor cycle accidents which was responsible for 45 (19.5%) of the cases. A significant number of the victims, (n=15, 6.5%) were left with varying degrees of residual morbidities. These, fortunately, are preventable events. The high figure is as a result of the use of motor cycles as taxis, a common feature of the developing countries. These agents are 2-wheeled thus less stable than the cars. This is further compounded by the non-use of Crash helmets in our environment [22] exposing them to high risks of severe injuries and deaths.
Road traffic accidents are a major cause of deaths from head injury, globally. According to Genarelli, Chairman of the American Association of Neurosurgeons while addressing a joint session in 1989 stated ‘About one person dies of head injury every 5 minutes in the U.S, which means that in the last 12 years, the number of deaths from head injury has exceeded all the military deaths in all the wars fought by the nation since 1776. In addition, an equal number of people survived head injury with substantial permanent impairments and twice may have temporary dysfunction. The direct and indirect cost of these, principally because they involve the youths and young adults alike, is estimated at $25 Billion yearly’ [23].
There were 16 (6.9%) cases of facial nerve palsy of which 5 (2.2%) were cases of HIV/AIDS. Researchers in other parts of the globe have reported similar findings of which viral neuropathy have been implicated [24]. The occurrence of facial nerve palsy with no apparent cause should raise suspicion. However, 2 (0.9%) of the patients were fatal cases of malignant otitis external. In these, a 21/2 year old male child had severe protein energy malnutrition while the other, an elderly male with poorly controlled type 2 diabetes mellitus. They all succumbed to the disease progression during treatment. High fatalities have been reported to be associated with the disease [8]. A unique cause of facial nerve palsy was observed in this series. It involved a 27 year old male who had his left pinna nearly amputated following assault in a political rally. Assessment at operation was that of a sharp knife cut through the anterior part of the tragus, cutting through the parotid gland and dividing the external auditory canal almost at the junction of the outer cartilaginous 2/3 and medial bony 1/3. Features of facial nerve palsy manifested 72 hours post repair as oedema had subsided significantly. He ended up with a Frey’s syndrome, subsequently. Political violence is a common phenomenon in developing countries and thus a threat to democratic governance. All the patients had ipsilateral hemifacial physiotherapy along with low dose Steroids, Vitamin C and Encephabol with 7 (3.0%) that ended with Grade II House and Brackmann’s facial palsy persisting after 1year out of which all were cases of HIV. In a randomised controlled trial, Cardoso et al. [25] also observed facial exercise with EMG biofeedback satisfactory, though not statistically significant in managing facial paralysis.
Facial nerve paralysis poses a serious psychological alarm in patients as it has often been confused for a ‘stroke’ by most members of the public in our environment.
We evaluated 23 (10.0%) cases of vertigo of which BPPV accounted for almost half (n=11, 4.8%) followed closely by Meniere’s disease (n=9, 3.9%). The Epley’s manoeuvre was employed along with B-histine on BPPV treatment with satisfactory results based on prompt resolution of symptoms and reduced frequency and severity of attacks that impacted positively on patients’ healthrelated quality of life (HRQoL). A recent study reported the efficacy of these treatment modalities [26]. The study recorded a rare form of vertigo termed otolithic crisis of Tumarkin yet to be reported in West Africa. A significant number (n=5, 2.2%) were still left with residual disease expected to visit the hospital regularly for a long period of time.
This study recorded 16 cases (6.9%) of sudden hearing loss which were mainly unilateral. However, for a 55 year old woman, she had a simultaneous sudden bilateral sensorineural hearing loss. Reported result of her random plasma glucose was 536 mg/ dl (29.8 mmol/l). This was the first time she was diagnosed of type 2 diabetes mellitus. A study reported that sudden hearing is a terrifying experience with unilateral idiopathic sudden sensorineural hearing loss occurring in over 90% cases in which spontaneous resolution is the norm. However, bilateral sudden sensorineural hearing loss points to something sinister, therefore requires careful evaluation [27]. This is one of the few documented cases in the literature. Her symptoms regressed significantly on commencement of anti-diabetic regimen within a week. Cochleovestibular complications of diabetes mellitus has been described [28] being a result of diabetic micro-angiopathy.
The persisting excruciating pains associated with otomycosis and wax impaction were a cause of OE in 9 (3.9%). Two (0.9%) of the cases of unilateral Sudden hearing loss were incidentally found to be reactive for HIV antibody by the Rapid test and confirmed by the Western blot. They had no previous history of ear disease. Therefore, sudden hearing loss in an apparently healthy adult not previously having ear disease should be suspected for HIV.
Both were middle-aged males of high social status in the society who presented for the first time with the symptom. Human immunodeficiency viral infection has also been documented as aetiology of sudden sensorineural hearing loss [29].
Foreign body (FB) in the middle ear are still being observed in our environment. The attending first physician, commonly, a non-specialist, makes several futile attempts that eventually get the FB in the middle ear space. The dearth of ENT surgeons estimated at 1/26.7 million [30] in our environment could partly be responsible. Two of the FBs were alkaline batteries. The dreaded complication, middle ear necrosis with facial nerve palsy seen in alkaline battery observed by McRae et al., [31] was not seen, probably as it had not stayed long enough to discharge its alkaline chemical contents before removal.
Mastoid abscesses 10 (4.3%) were the most common extracranial complications of CSOM found in this study. They had mastoid exploration, type II tympanoplasty and necessary adjunctive treatments. Results of treatment were satisfactory though recurrence was a problem in a few of them.
The occurrence of otogenic tetanus, which accounted for 1.3% with the attendant high mortality, is a result of the poor hygiene, poor immunisation coverage as stipulated by WHO; a feature of Low resource countries. In the developed world, however, CSOM is virtually non-existent [32] thus otogenic tetanus an uncommon presentation.
All cases of lateral skull base fractures with CSF leak were longitudinal as confirmed by high resolution CT-scan. They were managed conservatively with satisfactory outcome though a sizable number (n=15,3.9%) had residual morbidities including tinnitus, vertigo and mild-moderate sensorineural hearing loss which did not affect their social life significantly. In a case series, spontaneous recovery was reported also in 77.9% by Brodie et al. [33] thus advocate surgical intervention for a few cases with persistent fistulae after a week of occurrence for fear of meningitis as a complication.
Otomycosis was managed using Otomed impregnated wick dressing for 2-4 weeks after ear syringing for the fungal collections in the external auditory canal. The outcome was satisfactory while cases of HIV and AOM were managed conventionally. Mgbor et al. [34] reported Mercurochrome as a viable treatment option for otomycosis for which both symptomatic and fungal clearance was observed within a week of therapy in 95.8%.
Finally, the 11.7% of the patients that had various persistent morbidities will eventually affect their Health Related Quality of Life (HRQoL) adversely, the inconceivable cost of which only them can tell.
Conclusion
Otologic emergencies are the most prevalent in Otolaryngologic practice with a grave prognosis.
Acknowledgement
We wish to acknowledge the consultant staff of the Department for accepting the recruitment of their patients into this study. We shall also not forget to say a big thank you to Ms Clara Ajayi, the Departmental secretary, for her great secretarial work which made the study a huge success.
Authors contributions
DK-Performed the literature search, collected data and statistical analysis
TI- Mentorship, conceptualised the idea and proof read.
7040
References
- Bademosi O,Ogunlesi TO, Osuntokun BO (1987) Clinical study of unilateral peripheral facial nerve paralysis in Nigerians. Afr J Med MedSci 16: 197-201.
- Barman D,Maridal S, Goswami S, Hembram R (2012) Three years audit of the emergency patients in the department of ENT of a rural medical college. J Indian Med Assoc 110: 370-374.
- Ijaduola GT, Okeowo PA (1986) Foreign body in the ear and its importance: the Nigerian experience. J Trop Pediatr 32: 4-6.
- Ibekwe TS,Nwaorgu OG, Onakoya PA, Ibekwe PU (2005) Spectrum of otorhinolaryngology emergencies in the elderly in Ibadan, Nigeria. Niger J Med 14: 411-414.
- Fayemiwo SA,Ogunleye VO, Adeosun AA, Bakare RA (2010) Prevalence of otomycosis in Ibadan: a review of laboratory reports. Afr J Med MedSci 39 Suppl: 219-222.
- Kokong DD,Bakari A, Ahmad BM (2014) Ototoxicity in Nigeria: why it persists. Ear Nose Throat J 93: 256-264.
- Osma U,Cureoglu S, Hosoglu S (2000) The complications of chronic otitis media: report of 93 cases. J LaryngolOtol 114: 97-100.
- Chen CN, Chen YS, Yeh TH, Hsu CJ, Tseng FY (2010) Outcomes of malignant external otitis: survival vs mortality. ActaOtolaryngol 130: 89-94.
- Lee KJ (2003). Anatomy of the ear. Essential Otolaryngology, Head & Neck surgery(8th edn), McGraw-Hill Medical publishing Division, USA.
- Groves J, Gray FG, Downton D, Blau JN (1985) A Synopsis of Otolaryngology. (4th edn),Wright publishers, USA.
- Teele DW, Klein J, Rosner B(1989) Epidemiology of Otitis media during the 1st 7years of life in children of the Great Boston. J Infect Dis 160:83-84.
- Alho OP,Koivu M, Sorri M, Rantakallio P (1991) The occurrence of acute otitis media in infants. A life-table analysis. Int J PediatrOtorhinolaryngol 21: 7-14.
- Huether SE,Defriez BC (2006) Pain, Temperature regulation, sleep and sensory function. McCance and Huether’s Pathophysiology:The biologic basis of disease in Adults and Children.(5th edn), Mosby Elsevier Inc publishers, USA.
- Ingvarsson L, Lundgren K, Olofsson B, Wall S (1982) Epidemiology of acute otitis media in children. ActaOtolaryngolSuppl 388: 1-52.
- Giebink GS1 (1992) Otitis media update: pathogenesis and treatment. Ann OtolRhinolLaryngolSuppl 155: 21-23.
- Ganong WF (1999) Higher functions of the Nervous system: Conditioned Reflexes, Learning and Related phenomenon.Review of medical physiology (19th edn), Appleton and Lange, Stamford, Connecticut Publishers, USA.
- Lou ZC, Lou ZH, Zhang QP (2012) Traumatic tympanic membrane perforations: a study of etiology and factors affecting outcome. Am J Otolaryngol 33: 549-555.
- Article 27 of the 1949 Geneva Convention in response to violence against women.
- United Nations study on violence against children. 61st Session, item 62 of the provisional agenda. General Assembly Resolution 60/231 On follow up, monitoring and implementation of the conclusion.
- Kanemaru S,Umeda H, Kitani Y, Nakamura T, Hirano S, et al. (2011) Regenerative treatment for tympanic membrane perforation. OtolNeurotol 32: 1218-1223.
- Lou ZC, Hu YX, Tang YM (2011) Effect of treatment at different time intervals for traumatic tympanic membrane perforation on the closure. ActaOtolaryngol 131: 1032-1039.
- Adogu POU, Ilika AL, Okaro CAN (2006) Road Safety Education and Mobilopathy Among Commercial Motorcyclists within Anambra State. Nig Med J 47:74-77.
- Gennarelli TA, Champion HR, Sacco WJ, Copes WS, Alves WM (1989) Mortality of patients with head injury and extracranial injury treated in trauma centers. J Trauma 29: 1193-1201.
- Timon CI, Walsh MA (1989) Suddensensorineural hearing loss as a presentation of HIV infection. J LaryngolOtol 103: 1071-1072.
- Cardoso JR, Teixeira EC, Moreira MD, Fávero FM, Fontes SV, et al. (2008) Effects of exercises on Bell's palsy: systematic review of randomized controlled trials. OtolNeurotol 29: 557-560.
- Hilton MP, Pinder DK (2014) The Epley(canalith repositioning) manoeuvre for Benign positional paroxysmal vergo. Cochrane Database of systematic Reviews 12: CD003162
- Sara SA,Teh BM,Friedland P1 (2014) Bilateral sudden sensorineural hearing loss: review. J LaryngolOtol 128 Suppl 1: S8-15.
- Lasisi OA, Nwaorgu OGB, Bella AF (2003)Cochleo-Vestibular Complications of Diabetes Mellitus in Ibadan, Nigeria. Intl Congress Series 1240:1325-1328.
- Lin C, Lin SW, Weng SF, Lin YS (2013) Increased risk of sudden sensorineural hearing loss in patients with human immunodeficiency virus aged 18 to 35 years: a population-based cohort study. JAMA Otolaryngol Head Neck Surg 139: 251-255.
- Badoe EA (2007) Middle Level ManPower Development A Necessity to Curb Shortage of Surgical Specialties. Proceedings at the 47th Scientific Conference of the West Africa College of Surgeons at Hotel De Meridien, Dakar Senegal.
- McRae D,Premachandra DJ, Gatland DJ (1989) Button batteries in the ear, nose and cervical esophagus: a destructive foreign body. J Otolaryngol 18: 317-319.
- Acuin JM (2007) Chronic Suppurative otitis media: A Disease Still Waiting For Solutions. Community Ear and Hearing Health 4: 17-32.
- Brodie HA, Thompson TC (1997) Management of complications from 820 temporal bone fractures. Am J Otol 18: 188-197.
- Mgbor N,Gugnani HC (2001) Otomycosis in Nigeria: treatment with mercurochrome. Mycoses 44: 395-397.


