Introduction
Chlamydia trachomatis(CT) causes the commonest sexually transmitted diseases in the United States and Europe [1,2] with approximately 4 million cases reported each year in the USA alone with paucity of information about the pathogen in Nigeria and other sub-Saharan Africa. Wilson et al. [3] reported that the highest prevalence in the USA is in people <25 years of age. Information about relative frequency of CT in Nigeria is sparse [4]. However, some studies have implicated Chlamydia trachomatis as a major cause of infections in Africa.
Okoror et al. [5] reported them as a likely cause of complications in patients visiting gynecological clinics in South East Nigeria which included both males and females visiting prenatal clinics for infertility cases and concluded that CT may have been involved in complications resulting in infertility of either males or females. Brunham et al. [6] had earlier reported that CT would be a major problem in Africa as its population begins to grow and therefore recommended more researches in sub-Saharan Africa in order to provide preventive and also prophylaxis knowledge needed to arrest the growth of this organism.
Sturm-Ramirez et al. [7] reported high prevalence of CT in asymptomatic commercial sex workers in Senegal with genotype E predominating and the women had no visible signs of infection. A major problem with CT infection is its ability to remain latent for a very long time [8] and then comes with very serious sequelae if left untreated. Such sequelae can include pelvic inflammatory diseases (PID), cervicitis, salpingitis, endometritis and infertility [9]. Though the effect of CT infection in females has been given more attention, it is also a cause of very serious infection in males which included urethritis, epididymitis and sometimes reactive arthritis. Okoror and Agbonlahor, [10] reported that CT could be a cause of male infertility where they linked CT to low sperm counts. In 2003, Ngandjigo et al. [11] screened 1277 Cameroonian students and found over 44% positive to molecular screening. CT has recently been given the status of a global pathogen by the WHO [12] and yet no routine screening of CT is carried out in Nigerian hospitals and this has called for more needed researches in Nigeria.
A study in Johannesburg has reported over 88% of pregnant women carrying CT and the possibility of 18% of them coming up with postpartum PID [13]. They also reported about 33% possibility of maternal infant transfer of the pathogen. This has also been reported by an earlier study where the mother, umblical cord fluid, the father were all positive to CT complement fixing antibody (CCFA) [5].
Despite all these reports, information about relative frequency and risk of CT in sub-Saharan Africa is still sparse when considering the magnitude of the pathogen with its sequelae. And the fact that the pathogen is not routinely screened for in the day to day laboratories in Nigeria presents enough rationale for more studies regarding CT.
Materials and Method
Urine samples (n=699) were collected from symptomatic individuals attending clinics in Akure, Nigeria. The consenting subjects were taught how to collect first course urine aseptically into sterile universal containers. The samples were immediately brought to the laboratories for analysis. All samples arrived at the laboratory less than one hour after collection.
A well-structured questionnaire was administered onto the subjects, this included their knowledge of STIs, sex education, number of sex partners, age, sex, condom use, age at first sex, sexual orientation, ethnicity, marital status, educational background, salary, occupation and length of stay in the study area. Other behovoural patterns also formed part of the questionnaire as well as the type of symptoms exhibited by the subjects which was well examined by a clinician was also taken into consideration.
All samples and reagents were allowed to attain room temperature. The urine samples were centrifuged at 3000 rpm. The supernatant were collected into a separate tube while the sediments were discarded. Centrifugation continued until there were no more sediments. The Enzyme Linked Immunosorbent Assay (ELISA) was carried out using the Human Chlamydia trachomatis IgM (CT IgM) and test carried out as outlined by the manufacturer (WKEA, China). Absorbances was measured in a microplate reader (Thermomax, Molecular Devices) at 405 which was the default and then at wavelength of 450 with blanking included and then the optical densities for individual samples were determined. The concentration of individual samples was carried out with Myassays ELISA online software, the concentration of the standards as against the samples were determined in milliMolar which was then multiplied by the dilution factor in order to get the actual density of IgM in each of the samples.
Results
Of the total of 699 symptomatic individuals screened for Chlamydia trachomatis (CT) infection, 546 (91.2%) were positive for CT IgM using the ELISA technique of which 221 (40.5%) were males and 325 (59.5%) were females. The mean age of the positive individuals was 21.5 years.
Their sociodemographic data and characteristics are shown in table 1. Age group 21-30 had the highest number of participants and the highest prevalence of 0.880 other age groups also have high prevalence mean of prevalence was 0.839 (SD=0.041). Of all the subjects, 281 were Yorubas, 122 were Ibos, Hausa had 21 subjects participating while the South-South had 172 participants. The Yoruba participants had the highest number of positive individuals with 40.4% of them being positive. The Ibos had 16.7% positive participants while the Hausas was 2.8% and the South-South participants had 21% positive participants. The Yoruba ethnic group also had the highest prevalence (crude=0.892, adjusted= 0.870); OR (crude=8.265, adjusted=The mean prevalence of all the positive individuals in the ethnic groups was 0.871 (SD=0.061).
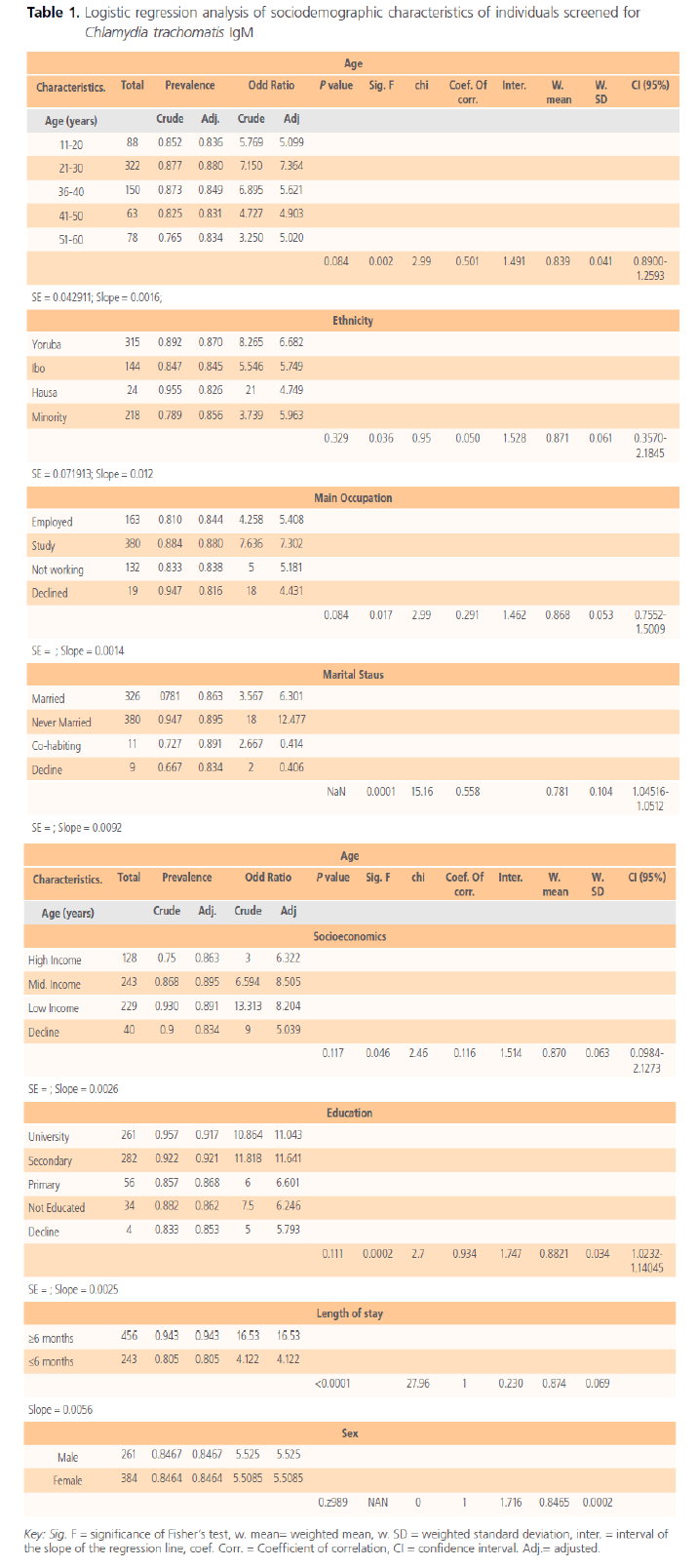
Table 1. Logistic regression analysis of sociodemographic characteristics of individuals screened for Chlamydia trachomatis IgM
The percentage of participants gainfully employed was 23.3%, while those still studying was 54.4%, those not working was 18.9% while 2.7% declined to give their occupational status. The studying groups comprising of mainly University undergraduates and some secondary school students had the highest prevalence (crude=0.884, adjusted=0.880); OR (crude=7.636, adjusted=7.302). The occupational mean prevalence of positive individuals was 0.868 (SD=0.053). The percentage of married participants was 46.6% while those not married was 54.4% and those co-habiting was 1.6%, 1.3% declined to reveal their marital status. The never married group had a prevalence of 0.947 and when adjusted it was 0.895; OR (crude=18, adjusted=12.47). The mean prevalence of all positive individuals according to their marital status was 0.781 (SD=0.104). Of the total participants 18.3% were individuals of high income while 34.8% were of medium income and low income earners were 32.8% while 5.7% decline to reveal their socioeconomic status. The highest prevalence was seen in the low income earners. University students had the highest prevalence and were closely followed by secondary school students. It was observed that those who stayed in the study area for about 6 months and above had higher prevalence and odd ratio than those who stayed less. Sexual characteristics shows that both male and females had the same prevalence and the same odd ratio, and the mean prevalence was 1.716 (SD=0.8465).
Table 2 shows the behavioral characteristics of individuals screened for CT IgM of which 31% were involved in heavy drinking and 50.8% were not and 3.9% decline to attest the questionnaire. The prevalence of CT IgM in both cases was moderate. Those participants who had first sex at age 11-20 years of age was 11.7% while 45.9% had first sex between ages 21-30 years. Those who had sex for the first time at age between 36-40 years was 28% of the participants. Sexual behavior of the participants show that 25.5% had 1 sexual partner while 27.3% had between 1-3 sex partners, 13.5% had more than 3 sex partners, 17.5% had no sex partner and 3.9% decline giving information. The percentage of participants regularly having protected sex by using condoms was 27.6%, 43.7% do not use condoms while 28.6% use it but not frequently.
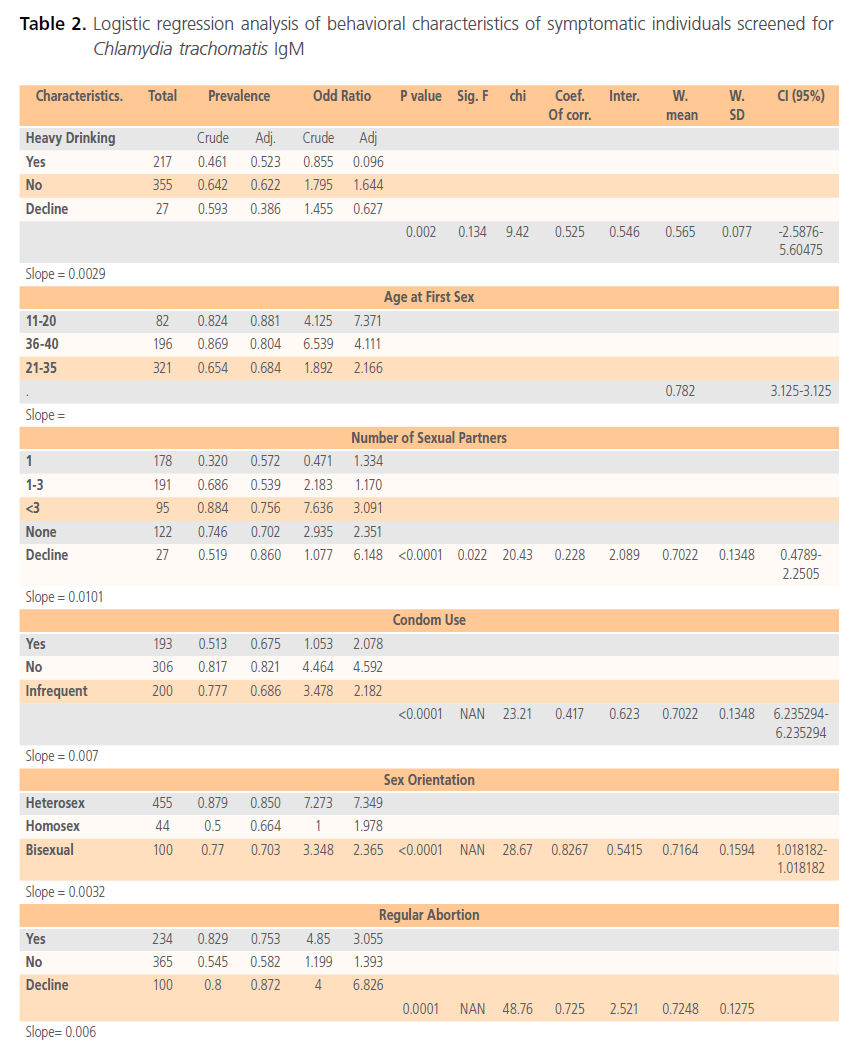
Table 2. Logistic regression analysis of behavioral characteristics of symptomatic individuals screened for Chlamydia trachomatis IgM
Of the total participants 65.1% were heterosexual while 6.2% were homosexual and 14.3% were bi-sexual. There was 33.5% of the participants involved with regular abortion while 52.2% were not and 14.3% declined. The mean prevalence of heavy drinking characteristics was 0.565 (SD=0.077, CI at 95%, -2.5876-5.60475) with engaged in regular heavy drinking having the lowest prevalence of 0.461 (adjusted=0.523), OR 0.855 (adjusted=0.096), for age at first sex the mean prevalence was 0.782 (CI 95%=3.125-3.125) and those who had sex later in life for the first time having a prevalence of 0.869 (adjusted=0.804), OR is 6.539 (adjusted=4.111), this was however not too different from those who had sex for the first time earlier in life.
Number of sexual partners had mean prevalence of 0.702 (SD=0.135, CI at 95%=0.4789-2.2505), those with more than 3 sexual partners had the highest prevalence to CT IgM (0.884, adjusted=0.756) OR (7.636 adjusted OR=3.091) while the mean prevalence of CT for the use of condom was 0.702 (SD=0.1345, CI at 95=6.235-6.235) individuals not using condoms at all had the highest prevalence of 0.817 (adjusted=0.821) OR (4.464, adjusted=4.592) and for sex orientation the mean prevalence was 0.7164 (SD=1.0182-1.0182) and the heterosexuals had the highest prevalence to CT IgM (0.879, adjusted= 0.850; OR=7.273, adjusted OR=7.349).
Participants interviewed for regular abortion had mean prevalence of 0.7248 (SD=0.1275) where those going for regular abortion have the highest prevalence of 0.829, OR (4.85, adjusted=3.055). The concentration CT IgM concentration (Figure 1) of all the samples were high as well as the actual density which was measured in Pg/ml of sera (Figure 2).
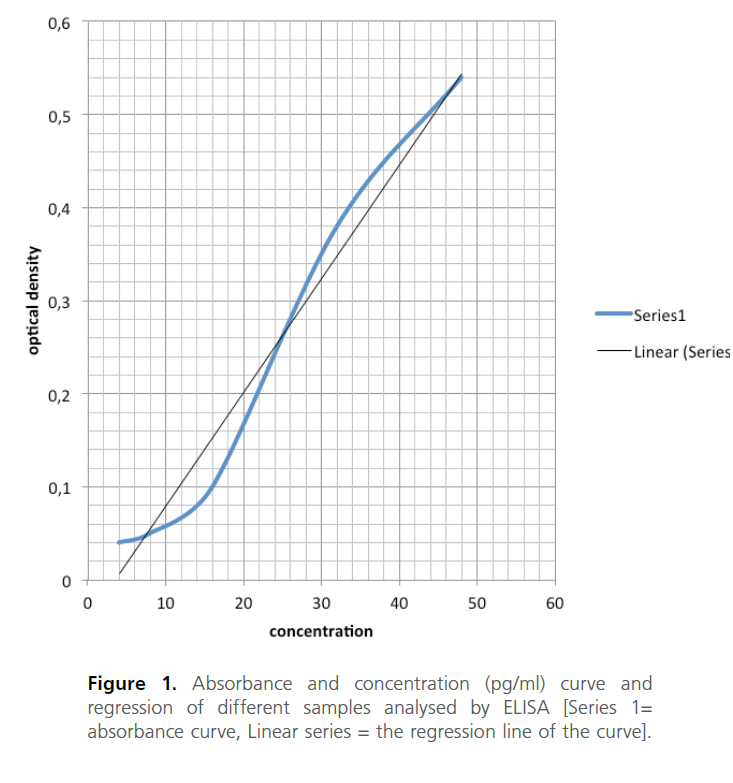
Figure 1. Absorbance and concentration (pg/ml) curve and regression of different samples analysed by ELISA [Series 1= absorbance curve, Linear series = the regression line of the curve].
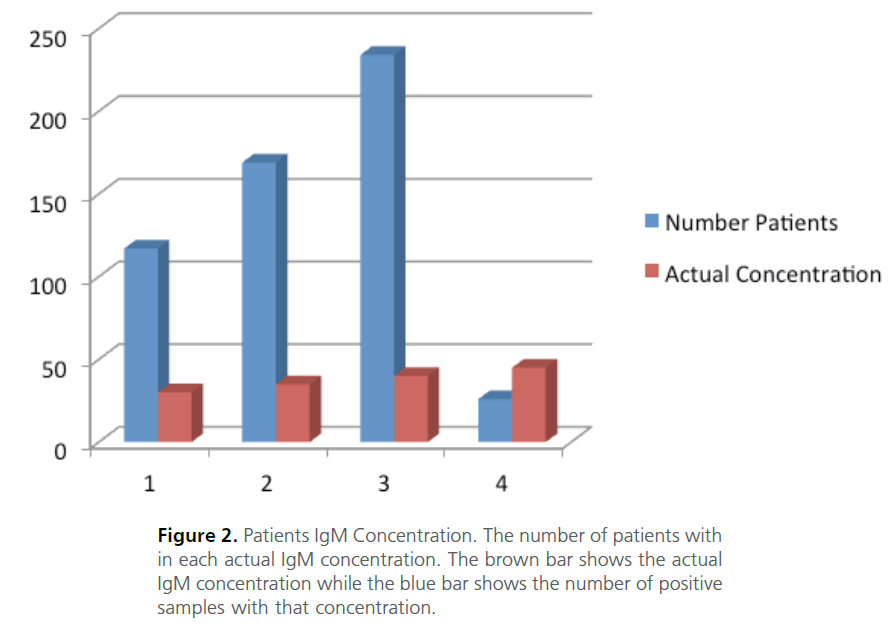
Figure 2. Patients IgM Concentration. The number of patients with in each actual IgM concentration. The brown bar shows the actual IgM concentration while the blue bar shows the number of positive samples with that concentration.
Discussion
This is the first study to provide prevalence data and risk factors for CT in symptomatic individuals based on their sociodemographic characteristics and behavioral patterns in Nigeria and especially in the study area. Previous studies in other areas of Nigeria have reported 29% prevalence in 2011 [14], in 2008 Okoror et al. [15] reported a 35.74% positive individuals attending gynaecological clinics which also includes their spouses, in 2009 34.1% were positive males for Chlamydia complement fixing antibody with non-specific urethritis while females were 46.3% positive [5]. However, all these studies are from a general or near general population with the exemption of Agbonlahor et al. [16], which was from a symptomatic individuals but with a specific disease condition.
In this present study with 91.2% positive result (p=0.084, CI=0.8900-1.2593) was statistically significant which was higher than the prevalence in USA in 2002 [3], in Nigeria 2008 [4]. Though Tukur et al. [4] screened the general population without specific symptoms. The positive cases in this study was also higher than that reported by Okoror et al. [5], Agbonlahor et al. [16] also screened a nonsymptomatic patients attending gynaecological clinics. The high prevalence in this study is in agreement with earlier reports of Sturm-Ramirez [7] where it was reported that prevalence of CT will continue to grow in African population. Results from this study are in contrary with that of Baud et al. [17] where low prevalence was reported among Swiss young men.
The result from this study supports earlier study by Okoror, [18] where high prevalence of CT was reported among patients with non-specific Urethritis. In 2012 Okoror et al. [10] also reported a high prevalence of CT in individuals with low sperm counts. Age groups 21-30 years of age had the highest prevalence and followed by age group 11-20 which is in tandem with age group of high sexual activity and forms the high risk group, which has also, being reported by Baud et al. [17] in Switzerland and Ikeme et al. [14] in Nigeria. A positive correlation (0.501) infers that age grouping correlates with CT infection.
Though the Yorubas had the highest prevalence most probably because the study area was in the Yoruba ethnic location, CT infection did not give a high correlation enough to implicate ethnicity in CT infection even when positive (0.05, p=0.329), Though the Yorubas had more odds (OR=8.265, adjusted=6.682) of having CT infection. There was no statistical significance between ethnicity and CT infection.
The occupation of participants correlates with CT infection (r2 =1.462; p=0.084) with those who are on regular employment being the least prevalence while the students and those not working having highest prevalence suggesting that lack of occupation may have cause high level of sexual activities due to the urge to engage in commercial sexual activity since there is the tendency to have less income or other activities likely to influence more contact with CT and other STI [18]. This is opposed to earlier study by Kohli et al.[22] who in their study reported that those on regular occupation stand a more risk of contracting CT.
Lack of regular income may also be an impediment to access proper health care and inability to detect CT earlier since there was a significant association between CT infection and lack of regular income. Marital status of participants also correlated (r2=0.558; p=0.0001) with CT infection as the never married participants had the highest prevalence and highest odd (OR=18, adjusted=12.47) at contacting CT. This means that those never married are more exposed to CT infection, a situation similar to those obtained in America and Europe [1,2] and in Cameroon [11].
The medium and the low income earners had higher exposure to CT with higher odds. Hence there was correlation among there different socio-sseconomics status with statistically significance. The high income earners will usually have access to improved health care which is rather expensive in this part of the world. Hence the medium and the low income earners will naturally present with symptoms and are more prone to later CT sequelae which might be other secondary symptoms like cervicitis, PID, endometritis, salpingitis, infertility etc.
Educationally, University and Secondary school students had the highest prevalence and also the highest odd of contacting CT which is as a result of high sexual activity of individuals in this sub-group since a correlation of 1.747 (p=0.111) shows a correlation of educational status with CT. This is another surprising result because it is expected that the awareness to protected sex should be more with higher education as is the case with other STI, this part of the result is then in consistent with an earlier report that not all the risk factors for STI are acceptable risk for CT [19]. The length of stay in the study area did give enough association to CT infection and both of the parameters having high prevalence. There is no evidence statistically to show that the individuals contacted the pathogen in the study area or outside the study area.
Males and females have equal chances of contacting the pathogen having the same prevalence and a correlation of 1. This is in parity with earlier study by Beydoun et al. [19]. Several behavioral patterns was also studied which included heavy drinking, age at first sex, number of sexual partners, condom use, sex orientation and regular abortion and all high correlation to CT.
The striking surprise is that those involved with heavy drinking had lower prevalence which is contrary than those involved in heavy drinking, this is however, in agreement with Beydoun et al. [19] which reported no association with heavy drinking especially with the risk of high sexual activity and thereby risk for CT [20]. Age at first sex did not yield any correlation with CT infection which is consistent with Beydoun et al. [19]. This study is consistent with other studies regarding unprotected sex and increase in sexual partners; the odds are higher with lack of use of condoms and increase in unprotected sex [17,19]. Though this study does not present a high correlation with sexual orientation the heterosexual individuals presented with higher risk than with homosexuals and bisexuals, a finding that differs from earlier studies but at this point it must be made know that these type of sexual behavior is not popular in the study population as compared with those in the Western World.
Individuals undergoing regular abortion were shown to be more at risk as there was a strong association between regular abortion and CT infection which was significant. The high concentration of CT IgM in all the positive samples is a pointer to recent CT infection which goes to point to the fact that CT is very active in the population.
Conclusively, this study presents a cross sectional risk associated with CT and confirms that CT is very active in the population with more risk factors associated with it.
45
References
- Schillinger JA, Dunne EF, Chapin JB, Ellen JM, Gaydos CA, Willard NJ, Kent CK, Marrazzo JM, Klausner JD, Rietmeijer CA, Markowitz LE Prevalence of Chlamydia trachomatis infection among men screened in 4 U.S. cities. Sex Transm Dis, 2005; 32:74-77.
- Miller WC, Ford CA, Morris M, Handcock MS, Schmitz JL, Hobbs MM, Cohen MS, Harris KM, Udry JR Prevalence of chlamydial and gonococcal infections among young adults in the United States. JAMA, 2004; 291:2229-2236.
- Wilson JS., Honey E, Templeton A., Paavonen J, Mardh, PA, Stary A. and Stray-Pedersen, B A systematic review of the prevalence of Chlamydia trachomatis among European women. Journal of Human Reproduction Update 2000; 8 (4): 385-394.
- Tukur J, Shittu, SO and Abdul AM. A case control study of active genital Chlamydia trachomatis infection among patients with tubal infertility in northern Nigeria. Journal of Tropical Doctors. 2006; 36 (1): 14-16.
- Okoror LE, Agbonlahor DE, Esume FI and Umolu P.I Prevalence of Chlamydia in patients attending gynaecological clinics in South Eastern Nigeria. African Health Sciences 2007; 7 (1) 18-24.
- Brunham RC, Cheang M, McMaster J, Garnett G, Anderson R. Chlamydia trachomatis, infertility, and population growth in sub-Saharan Africa. Sex Transm Dis. 1993; 168-73.
- Sturm-Ramirez K.; Brumblay H, Diop K, Guèye-Ndiaye, A, Sankalé, J, Thior I, N’Doye I, Hsieh C, Mboup S, Kanki P Molecular epidemiology of genital Chlamydia trachomatis infection in high-risk women in Senegal, West Africa. Journal of Clinical Microbiology, 2000; Vol.38, No.1, pp. 138
- Nelson HD and Helfand, M.et. al. Screening for chlamydial infection. American Journal of Prevntive Medicine. 2001; 20 (3): 95-107.
- Bennett S, McNicholas A. and Garrett N. Screening and diagnostic practices for Chlamydia infections in New Zealand. New Zealand Medical Journal 2001; 114:349–352.
- Okoror LE and Agbonlahor DE High Prevalence of Chlamydia Trachomatis in the Sperm of Males with Low Sperm Count in Nigeria. Journal of Medical Microbiology and Diagnosis 2012; 1:3 https://dx.doi.org/10.4172/2161-0703.1000108
- Ngandjio A, Clerc M, Fonkoua, M Thonnon J, Njock F, Pouillot R, Lunel F, Bebear C. De Barbeyrac B, Bianchi A. Screening of volunteer students in Yaounde (Cameroon, Central Africa) for Chlamydia trachomatis infection and genotyping of isolated C. trachomatis strains. Journal of Clinical Microbiology, .2003; Vol.41, No.9, pp. 4404-4407, ISSN 1098-660X
- World Health Organization. Prevention and control of sexually transmitted infections: draft global strategy. [https://www.who. int]. WHO, 2006.
- Rours G, Duijts L, Moll H, Arends L, de Groot R, Jaddoe V, Hofman A, Steegers E, Mackenbach J, Ott, A, Willemse H, van der Zwaan E, Verkooijen R, Verbrugh sH. (2011) Chlamydia trachomatis infection during pregnancy associated with preterm delivery: a population-based prospective cohort study. European Journal of Epidemiology, Vol.26, No.6, (May 2011) pp. 493-502, ISSN 1573-7284-145, ISSN 1098-660X
- Ikeme AC, Ezegwui HU, Ikeako LC, Agbata I and Agbata E (2011) Seroprevalence of Chlamydia trachomatis in Enugu, Nigeria. Nigerian Journal of Clinical Practice. (14) 2; 176-180
- Okoror LE, SA Omilabu, PO Orhue and G Ajayi (2008) Seroepidemiological of Chlamydia trachomatis in patients attending pre and post natal clinics in Lagos Nigeria. The Open Tropical Medicine Journal 1, 83-86.
- Agbonlahor DE, Okoror LE and Esumeh FI, (2009) Seroepidemiological survey of Chlamydia in Noth West zone of Nigeria. Asian Pacific Journal of Tropical Medicine. 2(4) 1-8.
- Baud D, Jaton K, Bertelli C, Kulling J, and Greub G. (2008) Low prevalence of Chlamydia trachomatis infection in asymptomatic young Swiss men. BMC Infectious Diseases, 8: 45. Doi:10.1186/1471-2334-8-45
- Okoror L. Chlamydia trachomatis in non-specific urethritis. In: Clinical Management of complicated urinary tract infection, 2011; Ed. Ahmed Ali Nikibakhsh. Intech Open Access Publisher. Pp 71-82.
- Beydoun HA, Dail J, Tamim A, Ugwu B and Beydoun MA. Gender and Age disparities in the prevalence of Chlamydia trachomatis infection among sexually active adults in the United States. Journal of Women’s Health. 2010; 19: 12 ; 2180-2190. Doi: 10.1089/jwh.2010.1975.
- O’Leary A, Broadwell SD, Yao P, Hasin D. Major depression alcohol and drug use do not appear to account for sexually transmitted Diseases, and HIV epidemics in southern United States. Sexually Transmitted Diseases, 2006; 33, S70-77.
- Lowry R. Vassar Stat. Clinical Statistics Calculator https:// vassarstats.net/index.html
- Kholi R, Konya WP, Obura T, Stones W and Revathi G. Prevalence of Chlamydia infection in urban women of reproductive age, Nairobi, Kenya. BMC Research Notes 2013; 6:44

