Anna Zampetti1,2, Rossella Ceschini2, Giuliana Caporicci2, Marco Sigona2, Guido Massi3, Raffaele Manna1 and Paola Mariani4
1Rare Diseases and Periodic Fevers Research Center, Policlinico A Gemelli, Rome, Italy
2Complex Operative Unit of Dermatology, General Civil Hospital, Macerata, Azienda Sanitaria Unica Regionale, Marche, Italy
3Department of Histopathology, Università Cattolica del Saco Cuore, Rome, Italy
4Department of Histopathology, General Civil Hospital, Macerata, Azienda Sanitaria Unica Regionale, Marche, Italy
*Corresponding Author:
Anna Zampetti
Rare Diseases and Periodic Fevers Research Center
Policlinico A Gemelli, Università Cattolica del Sacro Cuore, Rome, Italy
Tel: 390630151
E-mail: anna.zampetti@gmail.com
Received Date: 17 November 2016; Accepted Date: 21 November 2016; Published Date: 24 November 2016
Citation: Zampetti A, Ceschini R, Caporicci G, et al. Rapidly Fatal Pseudo Gumma as First Presentation of Breast Cancer. Arch Can Res. 2016, 4:4 doi: 10.21767/2254-6081.1000114
Case Presentation
Keywords: Breast cancer; Gumma; Adenocarcinoma; Her2 receptor; HIV; Syphilis; Tuberculosis
A 46-year old single woman was seen following the appearance of a rapid onset ulcer of the anterior trunk (Figure 1A). According to the patient, the lesion appeared approximately two weeks before and it was followed by the onset of some other lesions on her back on the same side.
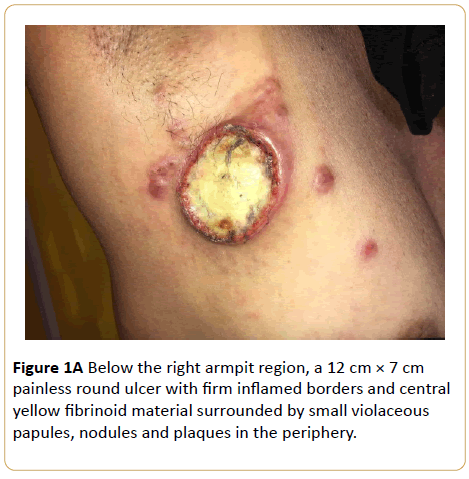
Figure 1A: Below the right armpit region, a 12 cm × 7 cm painless round ulcer with firm inflamed borders and central yellow fibrinoid material surrounded by small violaceous papules, nodules and plaques in the periphery.
They were not painful and the patient did not seek any medical advice, except for the local general physician who requested an urgent dermatological consultation. No topical or systemic therapy had hence been tried. Symptoms such as fever or cough were not reported neither weight loss. The medical history showed no relevant past diseases or surgery. Recent general blood tests, namely blood count and liver and kidney function tests, were all within the normal range. Family history was negative for any background for neoplastic diseases in first-degree relatives and social history failed to find recent travels abroad.
Objective Examination
Physical examination revealed under the right armpit, a well-defined crater-like ulcerative firm lesion with necrotic center, filled in by yellowish amorphous material and surrounded by inflamed borders. The main lesion was accompanied by smaller violaceous nodules in the periphery and plaques in the homolateral area of the back (Figure 1B). A remarkable axillary lymphadenopathy and of supraclavicular region were noted; breast was extremely firm and not moveable on lower layers.
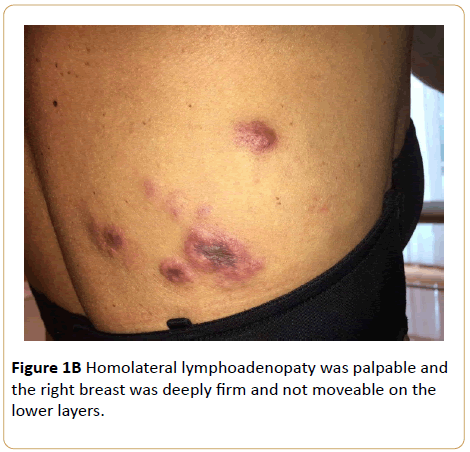
Figure 1B: Homolateral lymphoadenopaty was palpable and the right breast was deeply firm and not moveable on the lower layers.
Investigations
The main clinical differential diagnosis were syphilis or tubercular gummas, scrofuloderma, primary neoplastic process, including squamous cell carcinoma, and metastasis. Therefore, skin biopsy was performed urgently and other investigations such as chest X ray in two projections and VDRL, breast ultrasonography were requested.
Skin Biopsy and Histology
Histology of skin biopsy showed a massive infiltration of the dermis (Figure 2A) of cells with atypical morphology, several with nuclear atypia and mitoses that were characterized as adenocarcinoma (Figure 2B). A higher magnification allowed to highlight neoplastic emboli inside the vascular lumen (Figure 2C). Immunohistochemistry for oestrogen, progesterone and Her2 receptors showed triple negativity while Ki67 marker was positive up to 90% (Figure 2D).
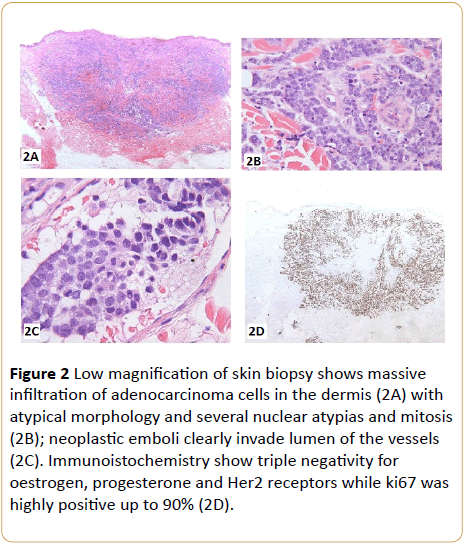
Figure 2: Low magnification of skin biopsy shows massive infiltration of adenocarcinoma cells in the dermis (2A) with atypical morphology and several nuclear atypias and mitosis (2B); neoplastic emboli clearly invade lumen of the vessels (2C). Immunoistochemistry show triple negativity for oestrogen, progesterone and Her2 receptors while ki67 was highly positive up to 90% (2D).
Unfortunately, diagnosis of metastasis of breast adenocarcinoma was confirmed only post-mortem since the patient died 10 days after our observation in another hospital. It was impossible to investigate the patient for HIV serology that could have potentially explained the rapidly fatal progression; syphilis serology was instead negative.
Discussion
Cutaneous metastases occur most often in breast cancer than in other neoplastic diseases of the female sex. In general, interventions for skin metastases should aim to arrest the progression of the disease, although such events often indicate a poor prognosis [1].
Cutaneous metastasis of breast adenocarcinoma usually occurs as inflammatory nodules most often on the trunk and rarely as lumps on the scalp. Sometimes, however, they can also mimic common pathological processes such as cellulite and lymphedema in the mammary region [2,3].
A major cause of morbidity and mortality in patients with breast cancer is the delay in seeking medical help. A recent study of 120 women with breast cancer has analyzed the "perception of disorder" and "the delay in seeking help" and found that the perception of the tumour influences the delay in seeking help, stressing the importance of educational interventions and counselling [4]. However in some cases the denial of illness may be related to simple negligence and, rarely, to dysfunctional psychological mechanisms. In our case we were unable to ascertain the immunological status of the patient and understand if the rapidly fatal progression was related to immunosuppression or just the result of a neglected disease. We know that HIV-infected patients with cancer have higher cancer-specific mortality than HIV-uninfected patients and more rapid and rapidly progressive deterioration, independently of cancer stage and treatment. This can be a direct consequence of relationship between immunosuppression and tumor progression [5].
In conclusion, we suggest always checking HIV serology, whenever possible, in any case of a rapid onset ulcer of unknown aetiology.
17592
References
- Lookingbill DP, Spangler N (1990) Skin involvement as the presenting sign of internal carcinoma. A retrospective study of 7316 cancer patients. J Am Acad Dermatol 22:19-26.
- Paolino G, Panetta C, Didona D, Donati M, Donati P (2016) Folliculotropiccutaneous metastases and lymphangitis carcinomatosa: When cutaneous metastases of breast carcinoma are mistaken for cutaneous infections.Acta Dermatovenerol Croat24:154-157.
- Kofteridis DP, Valachis A, Koutsounaki E, Maraki S, Mavrogeni E, et al. (2012) Skin and soft tissue infections in patients with solid tumours. Scientific World J804518.
- Attari SM, Ozgli G, Solhi M, Alavi Maid H (2016) Study of Relationship Between Illness Perception and Delay in Seeking Help for Breast Cancer Patients Based on Leventhal's Self-Regulation Model. Asian Pac J Cancer Prev 17: 167-174.
- Coghill AE, Shiels MS, Suneja G, Engels EA (2015) Elevated Cancer-Specific Mortality Among HIV-Infected Patients in the United States. J Clin Oncol33:2376-2383.

