Emily M Miner, Harini Gurram, Tennie Renkens and Julie L. Welch*
Department of Emergency Medicine, Indiana University School of Medicine, Indianapolis, Indiana, USA
Corresponding Author:
Julie L Welch
Department of Emergency Medicine, Indiana University School of Medicine
Indianapolis, Indiana, USA
Tel: 317-962-8880
E-mail: jlwelch@iu.edu
Received date: August 08, 2017; Accepted date: August 14, 2017; Published date: August 16, 2017
Citation: Miner EM, Gurram H, Renkens T, Welch JL. Recurrent Takotsubo Cardiomyopathy: A Rare Diagnosis with a Common Emergency Department Presentation. Arch Med. 2017, 9:4. doi: 10.21767/1989-5216.1000229
Copyright: © 2017 Miner EM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Takotsubo cardiomyopathy; Cardiomyopathy; Anxiety chest pain
Introduction
Takotsubo cardiomyopathy, a stress-induced cardiomyopathy also referred to as “broken heart syndrome,” is a non-ischemic cardiomyopathy that produces left ventricular dysfunction with characteristic left ventricular apical ballooning [1]. This most commonly affects post-menopausal women and is often precipitated by a physical or emotional stressor. The specific mechanism of Takotsubo is unknown but research suggests catecholamine excess and estrogen deficiency may be contributory. Excess levels of catecholamines and sympathetic hyperactivity, especially following a stressful event, are proposed to cause decreased myocyte contractility and apical akinesis due to a denser population of beta adrenoreceptors at the apex of the heart [2,3]. Post-menopausal women account for more than 90% of the cases, as such; estrogen is proposed to have a protective role against the toxic effects of catecholamines [4].
The incidence of recurrent Takotsubo cardiomyopathy after initial diagnosis is about 5% at 6 years with recurrence being more common when the initial episode has more severe left ventricular dysfunction [4]. While the long-term prognosis of Takotsubo is favorable in >95% of cases, acute symptoms of an episode can be life-threatening and lead to cardiogenic shock [5]. Proper diagnosis is crucial in these life-threatening situations. This is a case of a woman with recurrent Takotsubo cardiomyopathy presenting only with tachycardia and nonspecific ST-T wave changes in the lateral leads on her ECG who went on to experience dramatic hemodynamic instability and cardiogenic shock. After an eventual hospital stay, she made a full recovery. Emergency medicine physicians need to have an awareness of recurrent Takotsubo cardiomyopathy as its presentation can mimic other common diagnoses such as acute coronary syndrome and pulmonary embolism, but management priorities are often different.
Case Report
A 57-year-old female presented to a community emergency department (ED) with onset of chest palpitations after an argument. She described the palpitations as flutter-like with associated fatigue and chest tightness. Her past medical history was significant for atrial fibrillation status post ablation, anxiety, dyslipidemia, hypothyroidism, and an episode of Takotsubo cardiomyopathy 6 years prior to her presentation. Her most recent echocardiogram, 10 months prior, showed normal left ventricular function. Her medications included levothyroxine, venlafaxine, rosuvastatin and calcium plus vitamin D. Physical examination was significant only for tremulousness, tearfulness and sinus tachycardia. Initial vital signs showed heart rate=141, blood pressure=135/86 mmHg, respiratory rate=18/min, oxygen saturation=99% on room air, temperature=36.6°C (21:39). Initial electrocardiogram (ECG) showed sinus tachycardia rate of 128 with non-specific ST-T wave changes in the lateral leads and no ST elevation (Figure 1).
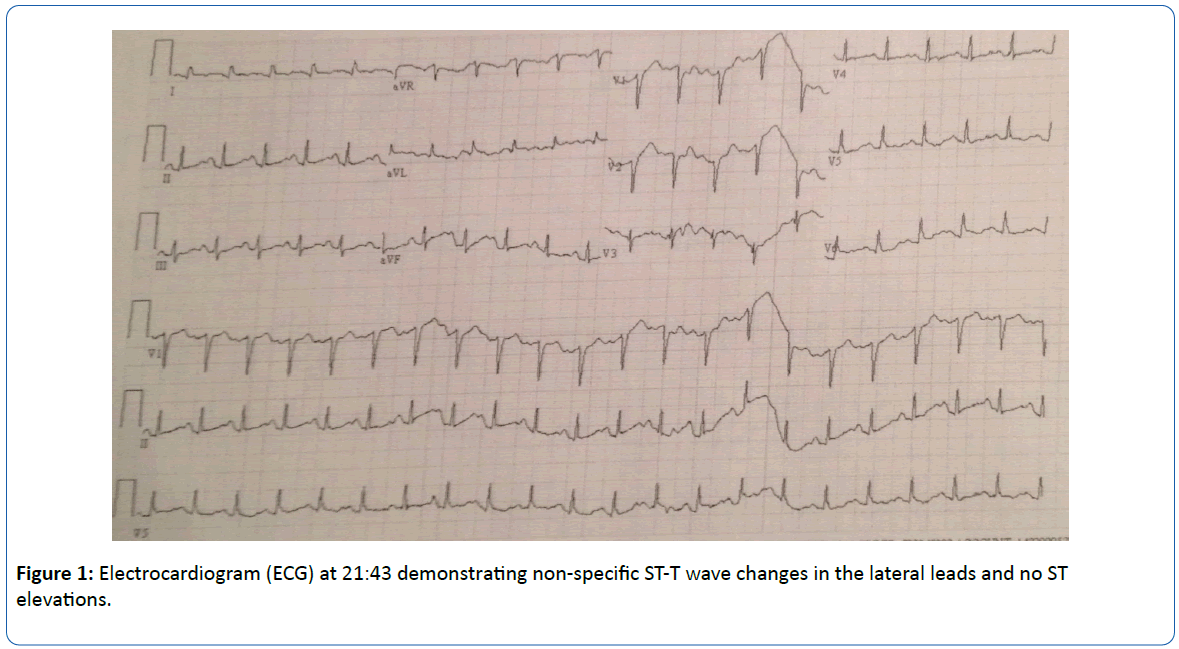
Figure 1: Electrocardiogram (ECG) at 21:43 demonstrating non-specific ST-T wave changes in the lateral leads and no ST elevations.
With pending laboratory results, a preliminary diagnosis of anxiety was made. Because the patient planned to drive herself home, no anxiolytics were administered; instead diltiazem 10 mg IV was administered to treat her tachycardia. When the patient was re-evaluated 10 minutes later she was hypotensive at 86/64 mmHg (22:23), and her blood pressure continued to decompensate to a systolic blood pressure (SBP) in the 60’s (23:11). Normal saline fluid boluses were initiated (22:23), totaling 4 liters, and her SBP improved into the 80s (23:20). Throughout her course, the patient remained responsive.
Due to the concern for cardiogenic shock, cardiology was emergently consulted. Her labs revealed an elevated troponin of 2.49 ng/mL (normal 0.00-0.06 ng/mL) (22:50). Interventional cardiology was also consulted for concerns of an acute coronary syndrome. Dopamine was initiated and titrated to 15 mcg/min (23:06). Within minutes, the patient developed atrial fibrillation with rapid ventricular response with intermittent ventricular tachycardia (23:17). Amiodarone 100 mg IV bolus was administered and a drip of 1 mg/min was started in an attempt to stabilize the patient.
It is significant to note here that due to the nature of this ED, the time of day, and other factors, a bedside echocardiogram could not be performed until the interventional cardiologist arrived. Consequently, other potential diagnoses were ruled out first. Once the patient was relatively stable, a chest CT angiogram was performed which ruled out pulmonary embolism (23:57). The interventional cardiologist performed a bedside echocardiogram, which revealed apical wall akinesis which is a near pathognomonic finding of Takotsubo cardiomyopathy (00:11). The patient was then taken to the cardiac catheterization laboratory (00:15) where she was found to have patent coronary arteries. However, due to refractory hypotension, an intra-aortic balloon pump was placed and remained for 48 hours. Over the next week, the patient’s condition improved with supportive care and she recovered to be discharged to home.
Discussion
This case is significant because it demonstrates a relatively rare clinical entity with common clinical cardiac symptoms. Upon initial presentation, the patient’s vital signs were notable with a sinus tachycardia of 141. Considering her past medical history of atrial fibrillation, Takotsubo cardiomyopathy, and anxiety, it was particularly important to explain this abnormal vital sign. Caution was warranted in interpreting the sinus tachycardia as simply anxiety, in this case because of her significant additional past cardiac history.
The typical presentation of a patient with Takotsubo cardiomyopathy is new onset chest pain, dyspnea, or syncope with and without ECG changes, and at times progressing to cardiogenic shock and frequently following an emotionally or physically stressful episode [6]. Possible differential diagnoses for Takotsubo include anxiety, panic attack, acute coronary syndrome (ACS), pulmonary embolism, Printzmetal’s variant angina, dilated cardiomyopathy, cocaine cardiomyopathy, hypertrophic cardiomyopathy, coronary artery vasospasm, and esophageal pathology. When a diagnosis is not clear upon initial presentation, it is important to re-evaluate any abnormal vital sign and expand the work up to ensure a diagnosis is not missed.
Important aspects of the initial workup that can aid in diagnosing Takotsubo cardiomyopathy include ECG, troponins, echocardiogram, high clinical suspicion, key historical elements such as previous MI precipitated by a stressful event and/or prior diagnosis of non-ischemic cardiomyopathy, cardiac catheterization without coronary artery stenosis, and left ventriculogram (Table 1). Since Takotsubo mimics other common diagnoses, on initial presentation patients may have had other episodes in the past. Upon review of this patient's chart, she had two previous acute coronary episodes classified as non-ischemic cardiomyopathy in 2003 and 2005.
| Clinical or Diagnostic Test |
Typical findings in Takotsubo Cardiomyopathy |
| Clinical evaluation (history and physical) |
Key historical elements such as previous MI precipitated by a stressful event. Prior diagnosis of non-ischemic cardiomyopathy. High clinical suspicion. |
| Laboratory evaluation of cardiac markers: Troponin, Creatinine Kinase Myocardial Band (CK-MB), Beta Naturiuretic Peptide (BNP) |
May or may not be elevated |
| ECG (Electrocardiogram) |
Changes can include non-specific ST and T wave changes and/or QTc prolongation |
| Echocardiogram |
Typically reveals evidence of left ventricular (LV) akinesis with reduced LV ejection fraction. |
| Cardiac Angiography |
No occlusive coronary artery disease. |
| Left Ventriculogram |
Typically reveals evidence of LV akineses of apical and mid ventricular segments and hyperkinesis of base. |
Table 1: Typical diagnostic findings in Takotsubo Cardiomyopathy [2,3].
Distinguishing the diagnosis of Takotsubo cardiomyopathy from an acute coronary syndrome is important due to the differences in management. There are medications that offer potential benefit in patients to reduce the risk of recurrence such as angiotensin converting enzyme inhibitors and angiotensin receptor blockers [4]. Because episodes of Takotsubo often follow stressful events, these patients can also be counseled differently to learn stress coping and relaxation strategies [7]. Furthermore, the implications of misdiagnosing and mismanaging Takotsubo cardiomyopathy can be fatal. If a patient is treated with inotropes, it could result in worsened outcomes by causing immediate hemodynamic instability worsening the left ventricular outflow tract (LVOT) obstruction [8]. In this case, the administration of a diltiazem resulted in hypotension and the administration of dopamine resulted in atrial fibrillation with rapid ventricular response. Diligence in pharmacotheraphy management is imperative.
Outcomes of Takotsubo cardiomyopathy are very promising as >95% completely recover. The severity of left ventricular dysfunction varies and some patients require intra-aortic balloon pump support, but many of these cases fully recover to a normal ejection fraction within a few weeks. Sequelae can include chronic intermittent chest pain and possible recurrence with arrhythmias occurring in ~2% and embolic events in 5% of patients; the post-hospital survival of these individuals does not differ significantly from the general population, most of their mortality is attributed to malignancy or non-cardiac conditions [5].
Conclusion
This case is a presentation of a rare condition, recurrent Takotsubo cardiomyopathy. This is an important disease to include in a differential diagnosis in the emergency department because prompt diagnosis and appropriate treatment helps avoid adverse outcomes. The cause of abnormal vitals such as tachycardia should be sought out and re-evaluated when a diagnosis has not been established. Emergency medicine physicians should have a higher suspicion of recurrent Takotsubo if there is history of a previous diagnosis of an acute coronary syndrome precipitated by a stressful event, cardiac catheterization without coronary artery stenosis, or a diagnosis of a non-ischemic cardiomyopathy.
20018
References
- Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, et al. (2004) Systematic Review: Transient left ventricular apical ballooning: A syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med 141: 858-865.
- Bounhoure JP (2012) Takotsubo or stress cardiomyopathy. Cardiovasc Psychiatry Neurol 2012: 1-4.
- Milinis K, Fisher M (2012) Takotsubo cardiomyopathy: Pathophysiology and treatment. Postgrad Med J 88: 530-538.
- Singh K, Carson K, Usmani Z, Sawhney G, Shah R, et al. (2014) Systematic review and meta-analysis of incidence and correlates of recurrence of takotsubo cardiomyopathy. Int J Cardiol 174: 696-701.
- Sharkey SW, Maron BJ (2014) Epidemiology and clinical profile of Takotsubo cardiomyopathy. Circulation Journal 78: 2119-2128.
- Templin C, Ghadri JR, Diekmann L, Napp LC, Bataiosu DR, et al (2015) Clinical features and outcomes of takotsubo (stress) cardiomyopathy. N Engl J Med 373: 929-938.
- Costin G, Mukerji V, Resch DS (2011) A psychosomatic perspective on takotsubo cardiomyopathy: A case report. Prim Care Companion CNS Disord 13:2.
- Vyas C, Shah S, Pancholy S, Patel T, Moussa I (2012) Consequences of misdiagnosis and mismanagement of takotsubo cardiomyopathy. Acute Card Care 14: 117-119.


