Keywords
Mobile phones; CCM; Diarrhea and Pneumonia; Children under five; Health workers
Introduction
Diarrhea and pneumonia are the leading causes of morbidity and mortality among children under five years of age [1,2]. Together, these two early childhood infections lead to one-fifth of the total number of under five deaths across the globe [3]. Major proportion of these deaths occurs in the resource scarce settings of Sub-Saharan Africa and South Asia [4].
Millennium Development Goal 4 had called for reducing childhood mortality by bringing down deaths from pneumonia to fewer than three children per 1,000 live births and diarrhea to less than one in 1,000 by 2015 [5]. However, Pakistan is still struggling to meet targets of improving child survival as each year 53,000 and 91,000 children die from diarrhea and pneumonia respectively thus contributing to 46% of overall under-five mortality in the country [4-6].
The National Programme for Family planning and Primary Health Care also known as the Lady Health Worker Program (LHW-P) was initiated by the Government of Pakistan in 1993 to provide “universal health coverage” to the underserved and poor communities of the rural and semi urban areas. The program includes deployment of lady health workers (LHWs) as first line caregivers in the rural communities [7,8].
These LHWs provide a broad range of primary health care services to their assigned communities including community case management (CCM) of childhood diarrhea and pneumonia. Currently, LHW-P covers 60% of Pakistan’s rural population and there are 130,000 LHWs deployed all over the country. This program also hires Lady Health Supervisors (LHSs) who are responsible for on-going supervision and mentoring of their LHWs. LHSs are supposed to be local female health workers of 22- 45 years of age with at least higher secondary level educational background and experience of working as a Lady Health Visitor (LHV) or a LHW for several years. LHS is the immediate supervisor of LHWs, attached with the first level care facility (FLCF) and supervises 15 to 25 LHWs according to a standard checklist. LHS reports to the Assistant District Coordinator (ADC) based at the District Program Implementation Unit (DPIU) [7].
The LHW-P has a community based information system which is part of the national health management information system (HMIS). In this routine information system, LHW identifies child health issues such as diarrhea and pneumonia during her household visits or within the static health houses established at her residence. Upon identification, LHW assesses sick child and provides appropriate management or referral as indicated in Integrated Management of Childhood Illness (IMCI) protocol. She also records information in her treatment register and reassesses the child during follow-up visit if required [7]. Supportive supervision remains a key approach to improve performance of the LHWs. As per the national LHS curriculum, it is defined as “a supervision strategy in which every supervisor knows about the needs of his/her subordinates. The supervisor tries to improve the performance of staff to achieve the goals of the program.” However within the current system, an LHS is required to visit each LHW only twice a month and hence gets informed about identified cases only on a monthly basis through LHW monthly reports. This reduces chances of timely feedback to LHWs by LHS on their case management skills and it’s an evidence of weak supportive supervision within LHW-P.
The fourth evaluation of the LHW-P has indicated that this weak supervision by the LHSs has led to inadequate case management of diarrhea and pneumonia by LHWs which may contribute to the stagnant under five 5 mortality and morbidity in Pakistan [9]. Evidence from this report also indicated lack of demand for high-quality information from all levels of the LHW-P leading to compromised accuracy, timeliness and relevance of data despite a high level of compliance by LHWs on filling the monthly reports [9,10]. One of the important reasons identified for weak supervision was lack of coordination between LHW and her LHS due to delayed flow of information. This gap of communication together with unavailability of transport reduces the chances of LHS making timely follow-up visits to homes of sick children, assess performance of LHWs in terms of CCM of diarrhea and pneumonia and provide feedback [9,11,12].
Project NIGRAAN (Urdu word, meaning supervision) aims to improve diarrhea and pneumonia related knowledge and case management skills of LHWs by addressing structural supervisory gaps in the existing LHW-P [13]. It aims at provision of timely feedback and supervision to LHWs by their assigned LHS using simple text based messages on mobile phones. Mobile phone technology (a component of mHealth) has already contributed to promote health care services in India, Bangladesh and Botswana [14,15]. Interventions based on use of mobile phones enhance efficiency of service delivery ensuring timely feedback and supervision by the health mangers through improved communication. Mobile technology has also revealed a promise of better child health outcomes by facilitating remote diagnosis and treatment in countries like Uganda and Rwanda [16,17].
This paper discuses usefulness of the mobile phones for early case reporting by LHWs resulting in timely follow-up visits and feedback provision by LHS in Project NIGRAAN. The ultimate goal is to improve CCM of childhood diarrhea and pneumonia through better LHW-LHS communication and connectivity.
Methods
NIGRAAN is an ongoing cluster randomized trial in District Badin, located in rural Sindh, Pakistan (area>6700 square kilometers, population 1.4 million). District Badin comprises of 5 sub districts (talukas) and 46 union councils (the smallest administrative unit) where 1098 LHWs are working under the supervision of 34 functional LHSs.
All LHSs working permanently in Badin who regularly conduct and report field visits were eligible to be enrolled in the study. Thirty four LHSs were allocated randomly to either intervention or control arms with a ratio of 1:1. The catchment area of one LHS was considered as a cluster. Thus there were 17 clusters in intervention and control arms each. Five LHWs were randomly picked from each cluster. This constituted the study sample (34 LHSs and 170 LHWs). These were then regularly monitored. The study focused on LHSs in intervention arm to enhance their core knowledge; clinical and mentorship skills related to CCM of childhood diarrhea and pneumonia through a specialized training ensuring mandatory written feedback to LHWs. In the control arm, refresher trainings were provided on CCM of diarrhea and pneumonia and routine standard of care was continued.
A surveillance system using mobile phones was set up by NIGRAAN in all clusters. All the 34 LHSs were trained and given simple mobile phones for real-time communication with their LHWs. Each LHS and her 5 enrolled LHWs received a minimum monthly communication allowance. ADC Badin assisted in coordinating the participation of health workers in the study.
The NIGRAAN surveillance system was superimposed on routine Management Information System (MIS) of LHW-P (Figure 1). LHWs in both study arms identified cases of diarrhea and pneumonia among children under five from their catchment areas as per their routine practice. Few specific monitoring tools were introduced by NIGRAAN adapted from already existing LHW-P MIS toolkit.
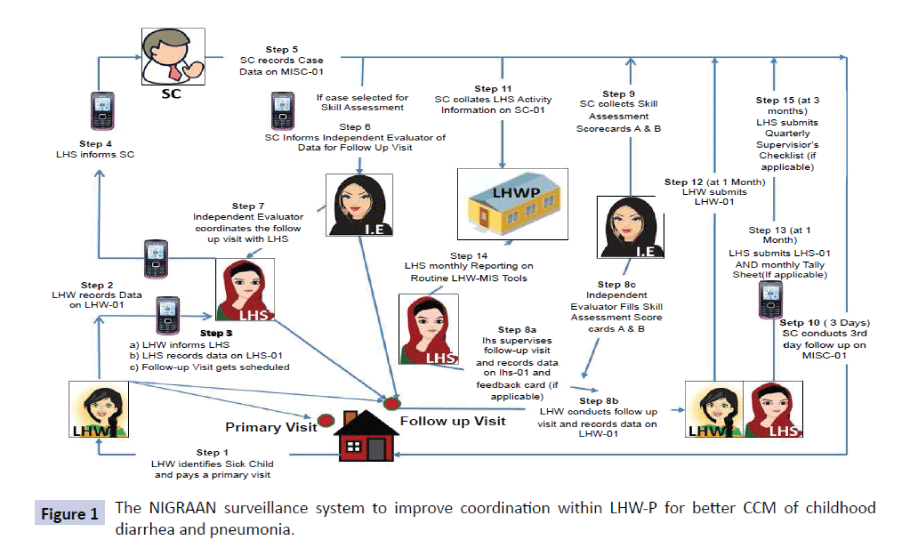
Figure 1: The NIGRAAN surveillance system to improve coordination within LHW-P for better CCM of childhood diarrhea and pneumonia.
Hence, after paying a primary visit to the household for case assessment, LHWs were also expected to record findings in a specially designed form (LHW 01) and inform her LHS via mobile phone short messaging system (SMS). At this point the LHW was also supposed to discuss and coordinate a suitable time when her LHS would accompany her for a follow-up visit to the home of the identified sick child. NIGRAAN encouraged that the latter visit take place within 24 hours of case identification. These follow-up visits by LHS were meant to ascertain the clinical findings of LHW and review case management plan. The LHS maintained data on LHS-01 form which assisted her to relay certain information to NIGRAAN study coordinator (SC) via mobile phone. The SC then recorded case information on a specially designed weekly case tracking sheet. SC concurrently maintained a database of diarrhea and pneumonia cases reported by LHSs right from identification till complete case management. The case management options including prescription of oral rehydrating salts (ORS), antibiotic, and counseling of care giver or advice for referrals to next level of care were carefully recorded. As a next step in the surveillance chain NIGRAAN appointed Independent evaluators (IEs) made telephonic follow-up of cases on third day of case identification to ascertain child health outcomes in terms of morbidity or mortality. This surveillance system was therefore sensitive enough to detect if cases were reported within 24 hours of identification and appropriately followed up by LHSs with timely feedback. Information about distribution of written feedback cards was obtained only from the intervention arm.
The LHW-01 forms (filled by the LHWs) were collected by their respective LHSs and submitted to SC during the LHSs’ routine monthly meeting in the LHW program office in Badin. This was to ensure that LHSs realize that it is their responsibility to get accurate information from their LHWs and provide the required supervision. SC sent these forms to project NIGRAAN’s research office at the Aga Khan University for data entry, analyses and report generation.
Spot maps were also maintained to identify emergent cases in each cluster and ensure proper surveillance. Gramin eTrex 10 was used to collect GPS coordinates from field and map out cluster level boundaries. Subsequently, mapping Software ArcGIS 9.3.1 was used to map the tracked cases of diarrhea and pneumonia to make cluster wise maps for cases identified through surveillance. The data obtained from these forms was analyzed using Statistical Package for Social Sciences (SPSS) version 19. Data are presented as frequency graphs.
Results
Use of SMS for case reporting
LHWs reported cases from their respective catchment areas. Between May 2014 and June 2015, a total of 6128 cases of suspected diarrhea and pneumonia among children under five were reported using SMS communication. Of these, 3058 were reported as suspected diarrhea and 3070 as suspected pneumonia. A positive trend in quarterly case reporting was observed overtime (Figure 2a).
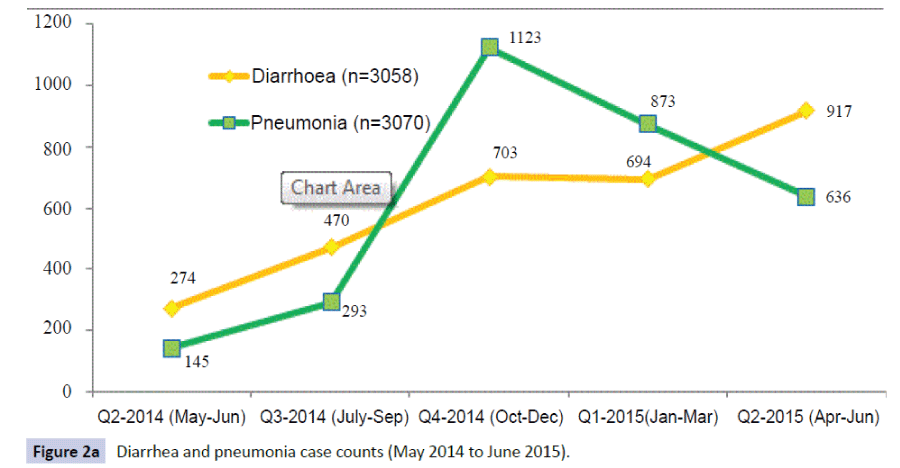
Figure 2a: Diarrhea and pneumonia case counts (May 2014 to June 2015). Figure
Figure 2b shows a comparison of spot maps of cases reported by LHWs during first and last quarters of surveillance. It is important to note that over time the clustering of cases has become dense as a result of better SMS based case reporting. As the momentum of SMS based coordination between LHWs and LHSs picked up, approximately a threefold increase in case reporting was noted by the last quarter of surveillance. Even though the actual cases in real time may be different, the case reporting of diarrhea and pneumonia was generally aligned with the expected seasonal trends for that quarter in the province with diarrhea being more prevalent during summer months and pneumonia during winter season [18].
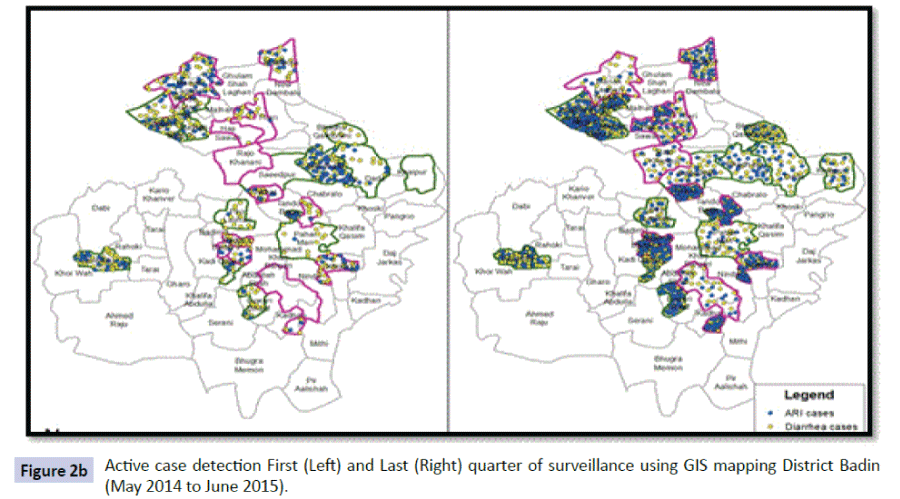
Figure 2b: Active case detection First (Left) and Last (Right) quarter of surveillance using GIS mapping District Badin (May 2014 to June 2015).
Compliance of LHWs and LHSs for SMS based case reporting
Figure 3 reveals that with continuous enforcement of surveillance system over a period of one year, both LHW and LHS reporting for diarrhea and pneumonia improved to almost 100% as compared to the baseline quarter (May-June 2014).
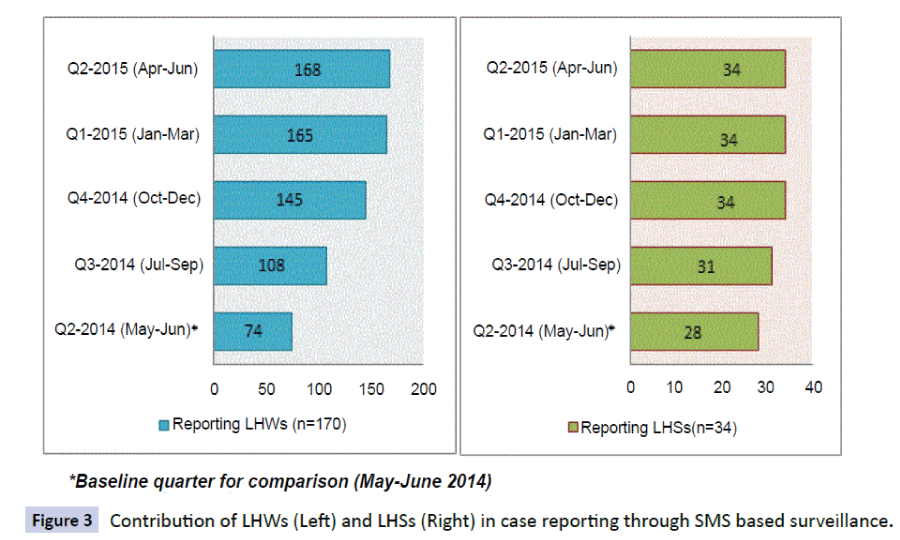
Figure 3: Contribution of LHWs (Left) and LHSs (Right) in case reporting through SMS based surveillance.
Timeliness of flow of information
Upon case identification, the information was relayed swiftly upwards within the surveillance system i.e. from LHW-LHS-SC. During the initial two quarters of setting up this surveillance system, only 67% of cases were reported from LHW to LHS within 24 hours of case identification. However, trends improved significantly during subsequent quarters reaching to 99% during the last quarter of surveillance. Similarly the relay of case information from LHS to SC level (within 24 hours of case identification by LHW) also displayed remarkable improvements; from 65% during first two quarters to 100% during the last quarter of surveillance.
NIGRAAN specific feedback cards to LHWs reporting cases
In general, SMS based relay of information from LHW to LHS also improved the chances of follow-up visits and feedback provision by LHS to LHWs. In the intervention arm of NIGRAAN, LHSs additionally aimed to provide written feedback cards to their LHWs as part of the supportive supervision intervention. During the first quarter of NIGRAAN intervention (Oct-Dec 2014), 86% LHWs reporting cases received feedback cards. This improved during subsequent quarters (Figure 4).
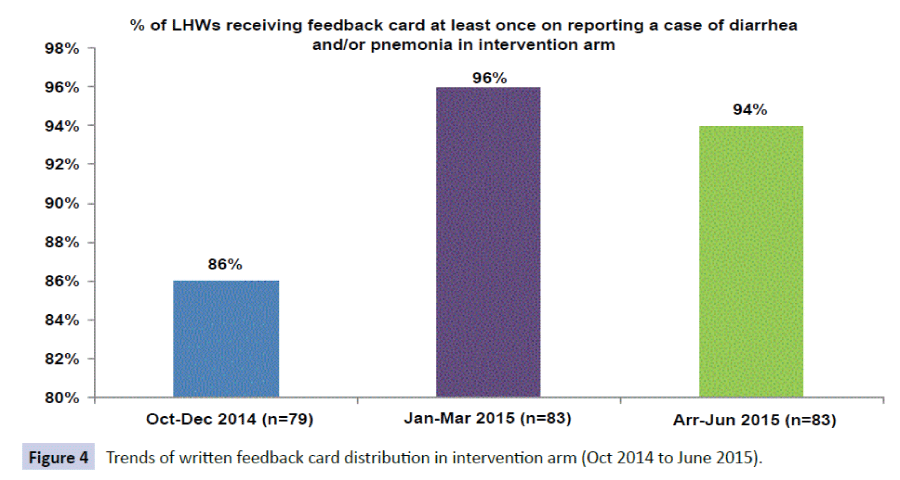
Figure 4: Trends of written feedback card distribution in intervention arm (Oct 2014 to June 2015).
Quality of service provision by LHWs
The surveillance system picked up several logistic issues which acted as a barrier in delivery of quality services by the LHWs. Despite timely case identification by LHWs and prompt followup visits by LHSs, shortage of supplies resulted in LHWs mainly resorting to counseling and/or referral services. Of the total 3058 suspected cases of diarrhea, ORS was provided to 709 (23%), while zinc was provided to only 308 (10%) cases. Likewise, out of a total 3070 cases of suspected pneumonia, antibiotics were provided to 63 (2%) and paracetamol to 403 (13%) only. Referral rates to other facilities were high (76% diarrhea; 88% pneumonia).
Child outcome on 3rd day of follow-up
Of all the reported cases (6128; diarrhea 3058, pneumonia 3070), successful telephonic contacts were made by IEs of NIGRAAN surveillance system on 3rd day of follow-up for 2500 (41%) cases to record the outcome of the episode of illness. It was noted that 47% had recovered with private treatment, 26% with government facility treatment and only 3% with LHW treatment. Only two deaths were reported.
Discussion
This is one of the first studies in Pakistan which has demonstrated that simple text messages delivered through mobile phones have the potential to improve coordination and communication between health workers resulting in early case identification and timely feedback from LHS to LHWs. Provision of personal low cost mobile phones and a minimal communication allowance increased health workers’ buy in within the established surveillance system. The ownership inculcated among the health workers slowly led to an evolving sense of responsibility to report cases within 24 hours of identification and provide care to the communities they are assigned. The results are quite similar to those found in Uganda, where wireless devices by health workers were used for disease surveillance, data collection and reporting. Thus faster and more accurate diagnoses were made with involvement of health workers’ supervisors [16]. In Rwanda, mobile phone SMS-based system was successfully designed and implemented to track pregnancy, maternal and child outcomes in a resource limited setting [17]. A similar study conducted in rural Bangladesh showed that mobile phone technology is an efficient and effective method for rapidly detecting and treating patients with malaria [19].
Surveillance in NIGRAAN improved the timely follow-up visits by the LHSs. These follow-up visits were meant to provide written or verbal feedback to the LHWs on their diagnosis, classification and management skills. Therefore, through supervisory visits, LHSs were able to objectively comment on case management and counseling skills of their LHWs. As reported elsewhere, these visits in NIGRAAN additionally helped to strengthen supervisory and mentorship skills of LHSs [20].
Comparing mean knowledge scores between visits, a recent facility based study in Nigeria has shown that supportive supervision is an effective intervention in achieving high quality malaria case management [21]. Another qualitative study of factors influencing motivation of community health workers in Mozambique has indicated that an improved supervision system in place was important to enhance motivation and performance of community health workers [22]. A review of impact and implementation issues related to supervision of community health workers in low-income countries has identified that simple, objective and structured methods of supportive supervision were useful and had greater impact on improving performance of health workers than merely improving frequency of supervisory visits [23].
In line with earlier evidence, [11,12] this study also confirmed that despite a good coordination among LHWs and LHSs, lack of transport and supplies (ORS, antibiotics) remain major bottlenecks and hinder LHWs and LHSs to provide the required standard of appropriate CCM for diarrhea and pneumonia [11,12]. The best health workers can do is to refer to the next level of care. Thus it is not surprising that NIGRAAN baseline household survey showed that community prefers other health providers over LHWs when their child is sick [20]. Studies conducted in semi urban areas of Sind also revealed that lack of supplies and compromised management skills of LHSs have been the main cause of high referrals of patients, raising questions over the effectiveness of the program [11]. Studies conducted in countries like Zambia and Bangladesh clearly indicate that adequate supply of essential drugs for health workers is crucial to effectively utilize strategic interventions that aim to complement existing systems of health care delivery at community level [19,24].
With this growing body of evidence it is time to invest in wide scale deployment of mobile phone technology in developing countries where access to good quality health care remains an unachievable goal for the poor and marginalized.
Conclusion
The LHW Programme in Pakistan provides readily available health services at the community level. NIGRAAN based surveillance provides convincing data that coordination through mobile phones has the potential to enhance diarrhea and pneumonia case reporting by LHWs leading to timely feedback provision by LHSs. However, for overall effective case management, mobile phone based strategies have to be complemented with a system that ensures accountability, supply chain management and is responsive to the health care needs of the community.
Source of Funding
Alliance for Health Policy and Systems Research, WHO Geneva.
Conflict of Interest
None
9735
References
- Walker CL, Rudan I, Liu L, Nair H, Theodoratou E, et al. (2013) Global burden of childhood pneumonia and diarrhoea. The Lancet 381:1405-1416.
- Wazny K, Zipursky A, Black R, Curtis V, Duggan C, et al. (2013) Setting research priorities to reduce mortality and morbidity of childhood diarrhoeal disease in the next 15 years. PLoS Med 10:e1001446.
- Black RE, Morris SS, Bryce J (2003) Where and why are 10 million children dying every year? The Lancet 361:2226-2234.
- Bhutta ZA, Das JK (2013) Global burden of childhood diarrhea and pneumonia: what can and should be done? Pediatrics 131:634-636.
- WHO (2007) Health System Profile-Pakistan. Regional Health Systems Observatory-EMRO.
- Rabbani F, Gul AX, P Shagufta (2012) Overcoming the MDG4 implementation challenges: redefining the role of LHS in structured supportive supervision of LHWs. Pak J Public Health 2:52-54
- Rabbani F, Zahidie A, Sangrasi K (2015) Combating Childhood Pneumonia and Diarrhea at Community Level: Potential of m Health to improve interaction among health workers. Infectious Diseases Journal of Pakistan (IDJ) 24:836-837.
- Rabbani F, Perveen S, Aftab W (2015) Investing in universal health coverage for childhood Diarrhea and Pneumonia: Lessons learnt from NIGRAAN Implementation Research. Pak J Public Health 5: 28-30.
- (2009) Lady health worker programme: External evaluation of the national programme for family planning and primary health care. Quantitative survey report. Oxford Policy Management: United Kingdom.
- (2008) National Health System Government of Pakistan. National Integrated Report: Analysis based on HMIS, LHWs-MIS and Other Data Sources. Ministry of Health, Pakistan.
- Afsar HA, Qureshi AF, Younus M, Gulb A, Mahmood A (2003) Factors affecting unsuccessful referral by the lady health workers in Karachi, Pakistan. J Pak Med Assoc. 53:521-528.
- Wazir MS, Shaikh BT, Ahmed A (2013) National program for family planning and primary health care Pakistan: a SWOT analysis. Reprod Health 10:4755-4710.
- Rabbani F, Mukhi AA, Perveen S, Gul X, Iqbal SP, et al. (2014) Improving community case management of diarrhoea and pneumonia in district Badin, Pakistan through a cluster randomised study—the NIGRAAN trial protocol. Implementation Science 9:186.
- (2009) Vital Wave Consulting. m Health for Development: The Opportunity of Mobile Technology for Healthcare in the Developing World. Washington, D.C. and Berkshire, UK: UN Foundation-Vodafone Foundation Partnership.
- Chigona W, Nyemba M, Metfula A (2012) A review on mHealth research in developing countries. The Journal of Community Informatics 28: 9.
- Asiimwe C , Gelvin D, Lee E, Amor YB , Quinto E, et al. (2011) Use of an Innovative, Affordable, and Open-Source Short Message Service–Based Tool to Monitor Malaria in Remote Areas of Uganda. Am. J. Trop. Med. Hyg 85:26-33.
- Ngabo F, Nguimfack J, Nwaigwe F, Mugeni C, Muhoza D, et al. (2012) Designing and Implementing an Innovative SMS-based alert system (RapidSMS-MCH) to monitor pregnancy and reduce maternal and child deaths in Rwanda. Pan African Medical Journal 13: 31.
- (2014) Weekly Epidemiological Bulletin. Disease early warning system and response in Pakistan 5: 17-40.
- Prue CS, Shannon KL, Khyang J, Edwards LJ, Ahmed S, et al. (2013) Mobile phones improve case detection and management of malaria in rural Bangladesh. Malar J 12:10-186.
- Rabbani F (2015) Helping children reach their fifth birthday in Sindh, Pakistan, SCIENTIA, Knowledge Translation Media pp: 52-55.
- Bello DA, Hassan ZI, Afolaranmi TO, Tagurum YO, Chirdan OO, et al. (2013) Supportive supervision: an effective intervention in achieving high quality malaria case management at primary health care level in Jos, Nigeria. Ann Afr Med 12:243-251.
- Ndima SD, Sidat M, Give C, Ormel H, Kok MC, et al. (2015) Supervision of community health workers in Mozambique: a qualitative study of factors influencing motivation and programme implementation. Human resources for health 13:63.
- Hill Z, Dumbaugh M, Benton L, Källander K, Strachan D, et al. (2014) Supervising community health workers in low-income countries–a review of impact and implementation issues. Global health action 8: 7.
- Meankaew P, Kaewkungwal J, Khamsiriwatchara A, Khunthong P, Singhasivanon P, et al. (2010) Application of mobile-technology for disease and treatment monitoring of malaria in the. Malaria journal 9:237.

