Introduction
There is a chronic shortage of skilled health workers globally, and the crisis is most severe in poor countries [1-5]. In Tanzania, the Ministry of Health and Social Welfare (MOHSW) estimated in 2006 that there were 29 000 staff working in government health facilities (65% shortage) and about 6000 staff working in private facilities (86% shortage) [6]. The shortage of health workers is more serious in the rural districts [7-10] which are mainly served by dispensaries – as shown in Figure 1
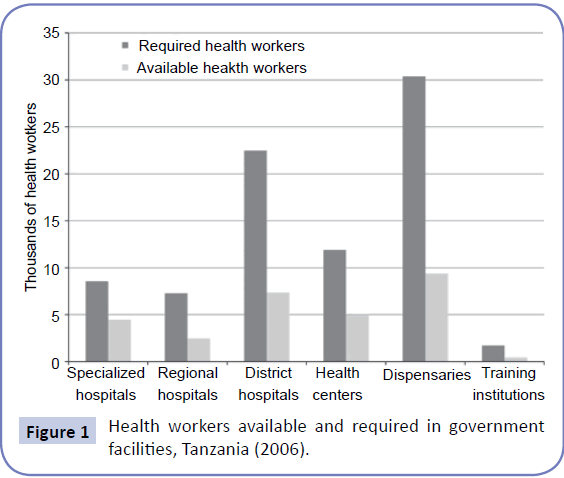
Figure 1: Health workers available and required in government facilities, Tanzania (2006).
Tanzania, like most developing countries, human resource for health is concentrated in major towns and cities at the expense of the rural areas which contain more than 75% of the population (World Bank 2008). It is estimated that rural districts contain about a third of available doctors and nurses. Lindi and Mtwara Regions in the Southern zone of the United Republic of Tanzania are the regions most affected by the Human Recourse for Health crisis. By 2009 the Regions had a shortage of 63.4% health workers [11]. Reluctance among qualified health professionals to work in these regions has resulted in this chronic and critical shortage. The 2009 situation analysis for Human Resource for Health (HRH) showed that 1499 health workers are serving a population of 940,533 in Lindi [12 -14].
In response to the serious shortage of qualified human resources for health in the rural health facilities, the government of Tanzania “silently” adopted a task shifting approach - which refers to a process of delegation whereby relatively less skilled staff are assigned to perform tasks otherwise handled by highly skilled/ specialized professionals [15]. Medical attendants constitute the lowest cadre of health workers but play the roles of clinicians in the rural health facilities facing critical shortage of skilled health staff. However, little is known on the characteristics of these semiskilled health. Therefore, this paper reports on characteristics of medical attendants and related implications for quality of health services in Lindi and Mtwara regions. It is a contribution towards forming the basis for recognizing an important role played by medical attendants and integrating their needs in quality improvement and continuing education programmes.
Methodology
Study Design: The research conducted was essentially a crosssectional, descriptive fact finding study. It was conducted in 2012. Its implementation followed a triangulated methodological approach. Both quantitative and qualitative approaches in data collection and analysis were employed. The review of existing documents and analysis of secondary data from institutions that were consulted also supplemented and strengthened information obtained from the two approaches above.
Sampling: Sampling was done at different levels. The two regions (Mtwara and Lindi) were selected purposively because they have fewer health workers compared to any other region in the country. In addition, these were the two project regions that the research team had to work in.
A strategic or purposive sampling technique was used to select six districts, three from each region. In consultation with regional authorities within the two regions and the Southern Zone Resource Centre, the study sites included those districts and health facilities that most heavily depend on the use of medical attendants, and as comparison, districts and health facilities that manage their health services with less dependence on unskilled cadres. A convenience sampling approach was used to select medical attendants and they were asked to respond to the semistructured questionnaire. Key informants were also selected strategically.
Data collection
Key informant interviews: Key informants at the regional and district levels were purposely selected on the basis of their strategic positions in policy and decision making on HRH recruitment, retention and training. They included regional medical officers, district medical officers, regional and district health secretaries, and district human resource officers. The informants were also recruited on the basis of their experiences and expertise knowledge in specific policies and regulations regarding health worker training, health worker carrier path and development. The aim was to learn in depth about the use of nonand semi-skilled personnel as one of the potential intervention to increase the quantity and quality of health workers in Lindi and Mtwara regions especially in the current times of acute shortages of required health workers. That is, the interviews at these levels sought to collect focused insights that reflect the feasibility of guaranteeing a minimum level of quality using semi- and unskilled cadres in order to create a strong evidence base for improving the quality of these cadres and their suitability for coping with the intervention addressable burden of disease in Lindi and Mtwara
Documentary review: A literature research was conducted with the use of suitable search engines such as google, google scholar, and PubMed to identify studies and evidence on the use of medical attendants or similar cadres and the marginal conditions for ensuring acceptable quality. While the search was in principal global, the focus was on experiences from Sub-Saharan Africa. Documents were reviewed in order to place the experiences in Lindi and Mtwara in a comparative context, and to learn how the existing practices in Lindi and Mtwara can be improved.
Examples of national and local documents that were consulted include: Council and Regional statistical reports; National Health Sector Strategic plan; Human resource policy and strategic plan; National, regional and district training policies and guidelines and other related policies and guidelines concerning training and development of health workers; Overall human resource development policy (for all public servants); and Global and national guidelines on interventions for attracting and retaining health workers especially in underserved remote areas, e.g. WHO Global Guideline on retention of Health workers in the rural areas 2010.
In the processes of reviewing these documents, a focus was on seeing whether they highlight or make any mention of ‘use of medical attendants or similar cadres’ as one of the potential effective interventions to increase the quantity and quality of health workers in places with fewer health workers relative to their actual population’s need.
Semi-structured questionnaire interviews with medical attendants: A semi-structured questionnaire was administered to all medical attendants who were on duty on the survey day to seek information on their socioeconomic and demographic characteristics. It also contained questions meant to inquire on their age, gender, marital status, educational background, training, experience, range of services they are able to offer, motivation, career expectations etc.
Analysis of data
The quantitative component of data analysis was done using SPSS version 15 software. Responses from closed- ended questions in the semi-structured questionnaire were coded before being entered into the computer. Coding of quantitative data was done by two data clerks in order to cross-check the quality of coded data. Primary analysis was performed using the generated categories in order to generate descriptive statistics – frequencies and percentages – that enabled understanding of the pattern of distribution. All important information was produced and presented in different forms including tables and figures.
For qualitative data (from document review and key informant interviews), thematic content analysis was used for their analysis. Tape-recorded key informant interviews were transcribed verbatim, and the information was combined with the responses recorded by note-taking. Then data were analyzed by examination and categorization of respondents’ opinions manually. The analysis took the form of three stages: line-by-line coding of field notes and transcripts; examination and interpretation of codes into descriptive and analytical themes; and development of an overarching theme [16,17]. The coding process involved development of concepts – that is, data were broken into discrete parts to expose thoughts and meanings contained in them. Additionally, two researchers coded qualitative data. They independently went through the analytic process – identification of codes to development analytic themes.
.Ethical consideration
Prior to the study, ethical clearance was sought from the Directorate of Research and Publications of Muhimbili University of Health and Allied Sciences. Moreover, study permission was processed from the respective authorities from whom the study respondents were recruited. Apart from the permission from relevant gate-keepers, this study sought bottom up permission (permission from the respondents) through explaining the aims of the study to each potential respondent. No names or any personal identifiers of the study participants were used in order to maintain confidentiality. Participants were given the opportunity to ask questions. They were also informed of expected duration for interview session to allow voluntary participation and to help participants to rationally decide whether to spend their time in the research or not.
Results
This section presents findings on medical attendants and the staffing profile of facilities that were involved in the survey.
Distribution of respondents by district
Data were collected from six selected districts. These districts and number of visited dispensaries are: Kilwa, Liwale [15], Nachingwea, Mtwara Rural, Newala [17], and Tandahimba. All dispensaries in each select district were targeted. Thus we reached more than 95% of the total number of dispensaries in a district. Few dispensaries could not be reached because of transport difficulties. Distribution of the respondents [medical attendants] in these districts is indicated in Table 1.
| District |
Sex |
Total |
| |
| Female |
Male |
| Kilwa |
40 |
6 |
46 |
| Liwale |
26 |
22 |
48 |
| Nachingwea |
36 |
13 |
49 |
| Mtwara Rural |
32 |
14 |
46 |
| Newala |
16 |
1 |
17 |
| Tandahimba |
28 |
4 |
32 |
| Total |
178 |
60 |
238 |
| |
Table 1: Distribution of respondents by district.
Table 1 shows that a total of 238 medical attendants were interviewed, of whom 178 (74.8%) were women.
The nature of semi-skilled health workers/ medical attendants in Mtwara and Lindi
The findings show that medical attendants are a group of health workers with low educational achievement, and limited or no formal training in health care delivery. This observation is illustrated in the following tables of results.
Table 2 shows that about two thirds, 146 (61.4%), of the total respondents had primary level of education. Most of them at most attended a one-year course in basic nursing, as indicated in Table 3.
| Educational Achievement |
District |
Total |
| Kilwa |
Liwale |
Nachingwea |
Mtwara Rural |
Newala |
Tanda- Himba |
| |
| Primary STD 7 |
22 (47.8%) |
18 (36.7%) |
29 (59.2%) |
40(87%) |
12(75%) |
25(78.1%) |
146 (61.4%) |
| Primary - below Grade 7 |
1 (0.2%) |
0 |
0 |
0 |
0 |
0 |
1(0.4%) |
| Secondary - Form IV |
23 (50%) |
31(63.3%) |
16 (32.6%) |
4(8.7%) |
3(18.8%) |
6(18.8%) |
83 (34.9%) |
| Secondary - below Form IV |
0 |
0 |
4 (8.2%) |
2(4.3%) |
1(6.2%) |
1(3.1%) |
8 (3.4%) |
| Total |
46 |
49 |
49 |
46 |
16 |
32 |
238 |
| |
Table 2: Medical attendants’ educational achievement.
| Skills Development |
District |
Total |
| |
| Kilwa |
Liwale |
Nachingwea |
Mtwara Rural |
Newala |
Tanda- Himba |
| One year Nurse Assistant course |
29 (65.9%) |
45 (93.8%) |
48 (96%) |
39 (86.7) |
14 (82.4%) |
27 (84.4%) |
202 (84.9%) |
| Other forms of basic training |
0 |
1 (2%) |
0 |
0 |
0 |
0 |
1 (0.4%) |
| Never Trained |
17 (34.1%) |
2 (4.2%) |
2 (4%) |
6 (13.3%) |
3 (17.6%) |
5 (15.6%) |
35 (14.7%) |
| Total |
46 |
48 |
50 |
45 |
17 |
32 |
238 |
| |
Table 3: Medical attendants’ skills development.
Table 3 shows that 202 (84.9%) of the respondents attended a one year course in basic nursing. Thus, they constitute a cadre of workers who were formerly called Nurse Assistants. The table further shows that 35 (14.7%) never attended any formal technical training. Among these the majority [17] were from Kilwa district.
Deployment of medical attendants within the health system and what they do
The study has established, through key informants, that Medical Attendants are being deployed to work at all levels of health care delivery – from the Regional Hospitals to the Dispensaries. However, their roles vary depending on the level of health facility. At the regional and district hospitals they have two roles. One, they are the cleaners and are the ones who move patients from one point to another for diagnostic and/or treatment purposes. Furthermore, Medical Attendants are responsible for moving objects such as medicines, medical equipment/ materials, linen, specimens, and documents to and from appropriate hospital units. Two, they fill the gap of shortage of nurses whereby they perform numerous procedures such as drug administration and wound dressing. As we move down the hierarchy, at the Health Centre and Dispensary levels, where shortage of skilled health professionals is more serious, Medical Attendants are increasingly entrusted with duties that require professional skills. Consequently at the dispensary level Medical Attendants are the “Nurses”, “Midwives”, and “Doctors” – administering drugs, dressing wounds, conducting deliveries, and prescribing treatment. Actually, it was learnt that Medical Attendants do conduct duties that are otherwise performed by Nurses/COs/CAs even in the facilities that have the cadres of skilled staff especially during night shifts and when the learned ones travel to the district headquarters for the purpose of attending seminars/workshops.
These findings are illustrated in Table 4 below.
| |
District |
Total |
| |
| Kilwa |
Liwale |
Nachingwea |
Mtwara Rural |
Newala |
Tanda- Himba |
| Yes |
17(54.8%) |
16 (61.5%) |
4 (13.8%) |
0 |
2 (8.3%) |
2 (6.7%) |
41 (24%) |
| No |
14(45.2%) |
10 (38.5%) |
25 (86.2%) |
30 (100%) |
22 (91.7%) |
28 (93.3%) |
129 (76%) |
| Total |
31 |
26 |
29 |
30 |
24 |
30 |
170 |
| |
Table 4: Facilities manned entirely by medical attendants.
Table 4 shows that Kilwa and Liwale districts led by far in having more than half of the studied facilities manned entirely by Medical Attendants.
Examination of competencies of medical attendants versus assigned tasks
As indicated in the preceding sections Medical Attendants try their best to perform duties that would otherwise be performed by COs/CAs, Nurses, and midwives. Again, most of these Medical Attendants attended a one-year course in basic nursing. The competencies they gained are grossly inadequate given the tasks they engage in, as indicated in Table 5.
| A |
Basic Nursing: Competencies attained following completion of 1 year course |
Essential interventions that medical attendants are challenged to engage in |
| |
| |
1. Meeting patients basic needs: |
Integrated Management of Childhood Illnesses (IMCI); Case management and prevention for acute febrile illnesses (AFI) including malaria; Insecticide Treated Nets (ITNs) for prevention of malaria; Intermittent Presumptive Therapy (IPT) for Malaria in Pregnancy, STD Syndromic Management; Safe Motherhood Initiative (SMI); EDP; EPI; TB DOTS; and Injury Care. |
| |
- Feeding the patient orally
|
| |
- Hygiene - bathing the patient, ward/facility cleanliness)
|
- Bed making
|
| |
d) Turning the patient |
| |
e) Lifting patients (body mechanics) |
| |
f) Therapeutic positioning of patients |
| |
- Meeting elimination needs – (giving and removing bed pan)
2. Basic Nursing procedures: a) Monitoring patient’s through taking vital signs – Blood Pressure, Pulse, Respiration, and Temperature. |
| |
b) Medication – The five Rs – right patient, right drug, right dose, right route, right site. c) Injection – intra-mascular (I/M) |
| |
d) Documentation of care provision |
| |
Table 5: Competencies versus assigned tasks.
Table 5 shows that those Medical Attendants who attended basic training in nursing have some skills. The competencies listed in Table 5 are similar to Medical Attendants’ nursing-related responsibilities indicated in the 2009 scheme of service [18].
These are:
• Cleaning work equipment, ward, and the environment.
• Assisting disabled and bed-ridden patients to meet their elimination needs (defecation and urination) and bathing them.
• Feeding a helpless patient.
• Taking linen to the laundry.
• Taking patient diagnostic samples to the laboratory and following up results.
• Preparing equipment and materials for wound dressing.
• Following up patients’ medicines from the store/pharmacy.
• Doing other duties that will be assigned to her/him by the in-charge.
A critical examination of competencies gained from one year basic nursing programme and tasks stipulated in the scheme of service reveals that Medical Attendants stretch themselves too much in handling essential interventions indicated in Table 6. In other words, given tasks that they do particularly in the dispensaries, there are glaring gaps calling for interim measures for improving their work performance. The impact of these gaps could be reduced if there were effective supportive supervision. Respondents were asked if they are ever supervised, Table 6 displays their responses.
| Ever been visited by supervisors? |
District |
Total |
| Kilwa |
Liwale |
Nachingwea |
Mtwara Rural |
Newala |
Tandahimba |
|
| |
| Yes |
45 (97.8%) |
46 (93.9%) |
45 (91.8%) |
41 (89.1%) |
15 (93.8%) |
31 (96.9%) |
223 (93.7%) |
| No |
1 (2.2%) |
3 (6.1%) |
4 (8.2%) |
5 (10.9%) |
1 (6.2%) |
1 (3.1%) |
15 (6.3%) |
| |
|
|
|
|
|
|
| Total |
46 |
49 |
49 |
46 |
16 |
32 |
238 |
| |
Table 6: Responses on whether respondents have ever been visited by supervisors.
Table 6 shows that most of respondents (223 out of 238) have been visited by supervisors. However, further findings show that supervisory visits are irregularly done. But, more importantly, one participant revealed that the kind of supervision that is done is not effective in improving quality of services. She said: “Hawasimamii kazi, wanauliza kama kuna tatizo”. Meaning, “They do not supervise work, they ask if there is a problem”. It was learnt that members of the Council Health Management Team are the ones who irregularly supervise medical attendants, offering limited or no clinical support.
Discussion
This study has documented that Medical Attendants in Tanzania are a group of health workers with low educational achievement, and limited or no formal training in health care delivery. This finding confirms previous reports which show that due to severe and critical shortage of health professionals the government is deploying Medical attendants/semi-skilled health workers for service provision – as an interim measure [19]. Furthermore, this study has revealed that while Medical Attendants are found at every level of service delivery, it is at the lowest level (dispensary) where their role as substitutes of skilled staff is vividly seen. Here Medical Attendants are the “Nurses”, “Midwives”, and “Doctors” – administering drugs, dressing wounds, conducting deliveries, and prescribing treatment. This finding does not match with what has been happening in other countries where the so called lay health workers (LHWs) have mainly served in the communities or have been working in specific programmes – for instance, Prevention of Mother to Child Transmission of HIV (PMTC), treatment of diarrhoea, acute respiratory tract infections (ARI), or malaria - offering non- or less technical components of health services. In these specific programmes LHWs have been mainly engaged in: visiting homes to educate mothers about ARI or malaria; early recognition of symptoms; first line treatment of cases by tepid sponging with anti-malarials or antibiotics; and referral of severe cases to health facilities [20].
This study has found out that Medical Attendants’ competencies are grossly inadequate, given tasks that they do particularly in the dispensaries. That is, the study has demonstrated that there are gaps in the way Medical Attendants perform “extra” responsibilities. This calls for interim measures for improving work performance – including short-term training programmes. The impact of training in improving performance of semi-skilled staff has been demonstrated in Brazil, Zambia, Ethiopia, Malawi, and Mozambique [21,22].
Besides, this study has revealed that supervision of medical attendants is irregularly done and is not supportive. This implies that the design and implementation of supervisory visits have had minimal impact with respect to improvement of Medical Attendants’ performance. The role of supportive supervision and mentoring in making task shifting effective has been emphasized by the World Health Organization [23]. Moreover, Tanzania, particularly Mtwara and Lindi Regions, may benefit by learning from Zambian experience [24,25]. Morris et al. did a study in Zambia and reported that the Zambian Ministry of Health has strongly supported an integrated program of task-shifting among providers. That is, the government of Zambia advocated a comprehensive, three-pronged approach to task-shifting that comprised training, on-site clinical mentoring, and continuous quality assurance.
Limitations of the Study
This study has two main limitations. One, the cross-sectional design constrained ability of the study to establish competencies of medical attendants through observation. Two, this paper lacks information on quality of care provided by medical attendants which was obtained through observation of performance. This gap will be addressed in the second paper to be developed by the same authors. These limitations notwithstanding, this paper sheds light on challenges facing Medical Attendants who work in the rural dispensaries as substitutes for qualified clinicians, and opportunities for improving their performance.
Conclusion
This study has demonstrated that critical shortage of skilled health workers in Lindi and Mtwara has resulted into Medical Attendants performing duties that they were not primarily prepared to do – particularly in the dispensaries. This is essentially an undeclared and unmanaged task shifting. It high time that “silence” was broken on the fact that in more than half of the dispensaries Medical Attendants perform duties that would otherwise be done by COs/CAs, Nurses, and Midwives. Implications of this fact on quality of services rendered to the poor rural residents are overwhelming. Breaking the silence may involve developing a policy and guideline that will recognize the important role played by Medical Attendants and shed light on how their work performance can be improved. This recognition will imply that while efforts for training, recruiting, and retaining qualified staff are going on, interim measures for improving quality of services offered by Medical Attendants are imperative.
It is recommended that: firstly, the Govermnet of Tanzania should consider implementing a three pronged approach to task shifting that comprises: training, on-site clinical training, and continuous quality assirance. Secondly, each facility [dispensary] should be visited by a team of supervisors a least once in a month. These supervisors should be required to participate in attending to patients so that medical attendants can learn from them.
Acknowledgement
This paper is drafted from a Research Report submitted to: EPOS Health Management, as part of Technical assistance to Tanzania/ Germany Programme to Support Health (TGPSH) for Human Resources and Capacity Development in Lindi and Mtwara.
11200
References
- Dussault G, Franceschini MC (2006) Not enough there, too many here: understanding geographical imbalances in the distribution of the health workforce. Human Resources for Health 4: 12.
- Figueroa-Munoz J, Palmer K, Dal Poz MR, Blanc L, Bergström K, et al. (2005) The health workforce crisis in TB control: a report from high-burden countries. Human Resources for Health 3: 2.
- Hanvoravongchai P (2007) Scaling up health workforces in response to critical shortages. The Lancet.
- WHO (2004) Health workforce challenges: Lessons from country experiences. High- level forum on health MDGs, Abuja. Geneva, World Health Organization.
- United Republic of Tanzania, Ministry of Health and Social Welfare (2007) Primary health services development programme–MMAM 2007–2017.
- Kwesigabo G, Mwangu MA, Kakoko DC, Warriner I, Mkony CA, et al. (2012) Tanzania’s health system and workforce crisis. Journal of Public Health Policy 33: S35-S44.
- Sikika (2010) Human Resources for Health in Tanzania, Baseline Report. The Findings from the NHRT trip.
- Musau S, Chee G, Patsika R, Malangalila E, Chitama D, et al. (2011) Tanzania Health System Assessment 2010. Bethesda.
- USAID (2003) HIV/AIDS and the workforce crisis in health in Africa: issues for discussion. Washington DC.
- The United Republic of Tanzania, MOH&SW (2007) A Report on Health Resources Study in Lindi&Mtwara Regions.
- Ministry of Health and Social Welfare (2009) Midterm review CHAI for scaling up.
- Ministry of Health and Social Welfare (2009) Analysis of HRH situation in Lindi.
- Niklaus D, Labhardt ND, Balo JR, Ndam M, Grimm JJ, et al. (2010) Task shifting to non-physician clinicians for integrated management of hypertension and Diabetes in Rural Cameroon: A programme assessment at two years. BMC Health Services Research 10:339.
- 16.Attride-Stirling J (2001) Thematic networks: an analytical tool for qualitative research. QRJ 1: 385-405.
- Thomas J, Harden A (2008) Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol 8: 8.
- JamhuriyaMuunganowa Tanzania (2009) MuundowaUtumishikwaWafanyakaziwaAfya.
- PetitMshanaE (2011) Human Resources Development in Mtwara and Lindi: A roadmap.
- Lewin (2006) Lay health workers in primary and community health care: A systematic review of trials.
- Lehmann U, Damme WV, Barten F, Sanders D (2009) Task shifting: the answer to the human resources crisis in Africa. Human Resources for Health 7:49.
- Morris (2009) Use of task-shifting to rapidly scale-up HIV treatment services: experiences from Lusaka, Zambia. BMC Health Services Research 9: 5.
- WHO (2008) Task shifting: Rational redistribution of tasks among health workforce teams: Global recommendations and guidelines.
- Anyangwe SC, Mtonga C (2007) Inequities in the global health workforce: the greatest impediment to health in Sub-Saharan Africa. Int J Environ Res Publ Health4: 93-100

