Keywords
COVID-19; Intensive care center; Health teams
Introduction
Coronavirus disease (COVID-19), whose etiologic agent is the SARS-CoV-2 virus, belonging to the b-coronavirus family, has been classified as a pandemic since March 11, 2020 by the World Health Organization (WHO). This new pathology causes severe respiratory problems, often leading the infected person to need support in the Intensive Care Unit (ICU) [1,2].
Due to the high virulence and infectivity, the disease in question soon made victims in numbers so high that the amount of ICU beds started to run out, causing chaos in both the scientific team and the public [3]. On the other hand, one of the measures found to try to attenuate the situation was the creation of field hospitals as well as the relocation of ICUs specialized in certain conditions for the treatment of patients with COVID-19 complications, as was the case of Bergamo Cardiology Unit, where 60% of the beds were occupied by COVID-19 positive patients [4], and of Children's General Hospital in Massachusetts, where 14 beds in the pediatric ICU were used for adults [5].
Even so, the level of stress is increasing in the frontline team, which includes ICU doctors, nurses and physiotherapists. For we live in a period of war in which suffering and death shine, both for those who live and for those who die, resulting from the disproportion between the needs of the sick and the available resources [6]. In view of this, stress is defined as the organic, psychic and social response to harmful promoters that an individual experiences [7].
In this circumstance, it is noted that the health team is guided by physical and emotional resistance to face life and death situations, even if their integrity is at risk [8]. Such commitment, especially from doctors, refers to the Hamurabi Code and the Hippocratic Oath. Currently, the primary relationship of this group with society is based on the social contract, putting in jeopardy the expectations of the people for care, competence, altruism, integrity, accountability and generation of the common good by the doctor, given that this one expects for trust, autonomy, social recognition, self-regulation and financing of a health system for the full exercise of their activity. However, the COVID-19 pandemic puts the contract at its extreme by making us question: do the risks experienced by these professionals need a limit? [9].
In view of this, it is necessary to remember that the history of mankind is marked by great outbreaks and epidemics as deadly as the current COVID-19 with devastating results on the psychicorganic health of the workers involved. To exemplify, in 2003, in China and Canada, the SARS-CoV-1 caused in at least 10% of the frontline professionals an increase in the stress level, with mental problems lasting and emerging up to 03 years post trauma, with focus on the somatization of symptoms (dizziness, headache, dyspnea), burnout, anxiety, Post-Traumatic Stress Disorder (PTSD), fear of a future outbreak and, especially, depression [3,7,10-12].
Another relevant contagious infectious disease was the Influenza A (H1N1) epidemic in 2009. Such illness had, as psychiatric consequences in the health team, the increase in anxiety, feelings of anguish and addictions (nicotine and alcohol) [10,12]. Recently, in 2013-2016, Guinea, Sierra Leone and Liberia experienced an outbreak of Ebola virus, causing significant psychological symptoms on health professionals, such as depression, paranoid ideation, fear of death or of having another similar experience and PTSD. Such consequences had a relevant impact on these individuals’ quality of life and work. [3,11,13].
Thus, it is clear that the frontline workers’ mental and physical health has already been pushed to the limit in past situations. In ordinary periods of society, it is known that at least 50% of doctors fight burnout or emotional exhaustion raised by the stress experienced at work [8]. Thus, it is inferred that the healthcare team in the ICU environment brings with themselves scars and marks of personal battles that are fought daily between themselves and the exercise of their work. However, COVID-19 marks the present day by promoting high moral damage associated with psychological suffering arising from actions, or absence of them, that violate the current moral or code of ethics in which the focus is the preservation of human life [12].
Therefore, the objective of this work is to understand the impact that COVID-19 is having on the frontline medical team in the ICU environment, as well as to reveal which proposals are being made to alleviate the harm that this group experiences.
Literature Review
A systematic review was carried out following the PRISMA protocol (Preferred Reporting Items for Systematic Reviews and Meta-Analysis). Through the definition of eligibility criteria, it was possible to organize the selected studies to answer a specific question.
The method allows an integration of studies with a lower degree of bias as well as a condensation of the results presented. The review was directed to answer the study question, constructed by the acronym PICO as follows: P-Health Team, I-ICU, C-Impacts of COVID-19 and O-Mental Health.
To search for studies, the following databases were used: Pubmed and Medline. After a previous analysis in the databases and consulting other studies that referred to the subject, it was possible to identify the following MeSH and DeCS descriptors: Patient Care Team, Psychosocial Impact, Health Impact Assessment, Coronavirus Infections/COVID-19, Intensive Care Units/CTI, Stress Disorders, Post-Traumatic. In order to make the search safer and make reproducibility greater, it was decided to associate all descriptors using the AND OR Boolean operators.
To search for studies, the following databases were used: Pubmed and Medline. After a previous analysis in the databases and consulting other studies that referred to the subject, it was possible to identify the following MeSH and DeCS descriptors: Patient Care Team, Psychosocial Impact, Health Impact Assessment, Coronavirus Infections/COVID-19, Intensive Care Units/CTI, Stress Disorders, Post-Traumatic. In order to make the search safer and make reproducibility greater, it was decided to associate all descriptors using the AND OR Boolean operators.
The manuscripts were evaluated by titles and abstracts initially to identify the initial inclusion criteria, always carried out by two reviewers. In cases of disagreement regarding the inclusion of a certain article, another reviewer was consulted for a final decision. The final inclusion of the articles was carried out carefully by reading the full text of the articles. Biases were analysed using the Cochrane scale.
Results and Discussion
In total, 573 evidences were found. With the subsequent application of the inclusion and exclusion criteria, 31 studies were included for qualitative synthesis. Figure 1 and Table 1 summarize the main methodological features for inclusion or exclusion of searched studies.
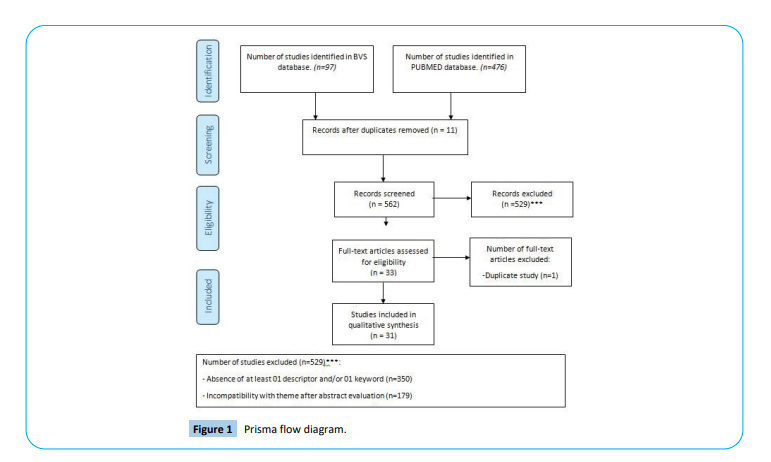
Figure 1: Prisma flow diagram.
| Title |
Author /Year |
Indexed Journal |
Main Findings |
| Attitudes of Anesthesiology Specialists And Residents Toward Patients Infected With The Novel Coronavirus (COVID-19): A National Survey Study |
Dost et al., 2020 |
Surg. Infect. (Larchmt) |
Anesthesiology specialists and residents should be protected during the performance of procedures with exposure to aerosols, associated with the incorporation of guidelines and flowcharts assisting in the approaches addressed, such as maintenance in ventilatory support; promotion of courses aimed at technical improvement in orotracheal intubation in order to guarantee the safety of professionals and the patient, as well as reducing panic to caregivers, which causes anxiety and psychological distress. |
| Reflexiones Derivadas De La Pandemia COVID-19 |
Raurell-Torredàet al., 2020 |
Enferm. Intensiva |
Recommendations for the correct handling of PPE and measures to reduce the contagion of nursing staff during the management of patients are described, such as how to keep a short time during the performance of invasive procedures and procedures with exposure to potentially contaminating material. Moreover it was recognized as an error faced by the Spanish health system during the pandemic the lack of recognition of the medical-surgical specialty of nurses in intensive care, the scarcity of PPE and the work overload faced by involved nurses. |
| COVID-19 Pandemic As A Watershed Moment: A Call For Systematic Psychological Health Care For Frontline Medical Staff |
Zaka et al., 2020 |
Journal Health Psychology |
The frontline professionals present high risk of developing burnout, psychological suffering, depression and post-traumatic stress disorder, among other psychological traumas, due to the exhaustive routine they are experiencing, being necessary to carry out a personal psychological support, directed to the demands of each individual and in the long term, in order to avoid or mitigate these impacts on this group’s social life. |
| COVID-19 experience in Bergamo, Italy |
Senni, 2020 |
European Heart Journal |
Doctors have experienced high stress situations in which it was prioritized the maintenance of these workers’ safety, the adequate supply of personal safety materials, adjusting the hospital organization for the care of positive covid-19 patients, changing the way these patients are screened and acquisition of telemedicine in the care and follow-up of cardiac patients who were managed in the service. |
| Repurposing a Pediatric ICU for Adults |
Yager et al., 2020 |
The New England Journal Of Medicine |
The modification of the care provided by the pediatric ICU team to approach covid-19 adult patients was seen as a great challenge, with gaps in the technical knowledge for approaching new patients, which were solved by the acquisition of therapeutic measures directed at these patients and, mainly, the preservation of the ICU team's constitution was fundamental for the success in the rapid transition and in maintaining the team's morale. |
| Fra cure intensive e cure palliative ai tempi di CoViD-19 |
Romanò, 2020 |
Recenti Progressi In Medicina |
The disproportion in the requirement and availability of ventilators and ICU beds trigger anguish in the medical team. The change in the way the patient is screened and admitted to the ICU in this pandemic moment is the best way to mitigate and try to adjust the work performed to the demand. Clinical criteria such as clinical severity, presence of comorbidities, age, cognitive and functional status and the presence of organ failure are parameters evaluated in association with ethical characters such as equity, equality and distributive justice. In this sense, patients who do not meet these criteria and show a poor prognosis should be submitted to the best palliative treatment; as well as maintaining psychological support for the victims’ families and for workers in order to avoid psychological problems such as PTSD. |
| Psychological stress of medical staffs during outbreak of COVID-19 and adjustment strategy |
Wu et al., 2020 |
Journal of medical virology |
When comparing the level of psychological stress between 2110 medical teams and 2158 university students across Chinese territory, Wuhan health professionals demonstrated higher levels of stress compared to workers in other provinces and students; a higher score was observed for aspects such as thinking of being ill or in constant danger, unsatisfactory sleep, concern for family members’ health, the need for psychological counseling and less hope for the victory of the experienced situation. |
| Preserving mental health and resilience in frontline healthcare workers during COVID-19 |
Santarone et al., 2020 |
The American journal of emergency medicine |
Experiencing a high number of friends’ and patients’ deaths leads to mental exhaustion, which, associated with social self-isolation from the family, contributes negatively to the mental health of frontline workers, putting them at risk of developing depression and suicide. In this sense, attitudes such as reducing workload and providing individualized psychological support and conditions for rest are imperative in order to mitigate these impacts. |
| Medical Professionalism and the Social Contract: Reflections on the COVID-19 Pandemic |
Ferreira et al., 2020 |
Acta Med Port |
It is believed that it is the doctor’s duty to be active in times of crisis. Such idea is consolidated by the social contract, which governs the rights and duties of the medical-society binomial. Thus, support and social recognition are relevant characteristics to stimulate and preserve the resilience of these caregivers, enabling the full performance of their work activities, even when their integrity is at risk. |
| Les professionnels de santé face àla pandémie de la maladie àcoronavirus (COVID-19) : quels risques pour leur santé mentale ? |
El-Hage et al., 2020 |
Encephale |
The identification of factors linked to the pathogen, such as high virulence and little scientific knowledge about it, conditions associated with work dynamics, such as the scarcity of PPE and technologies for the management of affected patients, as well as the psychological implications caregivers of first line are likely to develop, such as depression, PTSD, suicide, anxiety and others, are relevant to dictate the measures that must be taken to help this group face the pandemic and to enable the planning and construction of models of primary and secondary prevention of psychological damage in health workers in the face of future crisis situations. |
| Social support and mental health among health care workers during Coronavirus Disease 2019 outbreak: A moderated mediation model |
Hou et al., 2020 |
PloS one |
Resilience is seen as an individual protective factor and mediator in the relationship between health workers’ social support and mental well-being. In addition, among the 1472 caregivers interviewed, there was a greater dependence and correlation between resilience and psychic integrity in young people compared to middle-aged workers, for whom social recognition and experience acquired in other epidemics are relevant factors for coping with the COVID-19 pandemic. |
| Mitigating the Psychological Impact of COVID-19 on Healthcare Workers: A Digital Learning Package |
Blake et al., 2020 |
International journal of environmental research and public health |
The development of a digital package aimed at the immediate needs of the health team and their families during the pandemic, containing knowledge about communication between leaders and staff, social support, self-care strategies, emotion management and the provision of individual psychological support, was well evaluated by users and indicated as a model for other environments due to the produced benefits, practicality and low cost. |
| Covid-19: Supporting nurses' psychological and mental health |
Maben and Bridges, 2020 |
Journal of clinical nursing |
Nurses are considered the group most negatively affected in their physical, social and mental aspects in the face of the pandemic, given their close contact with patients and the performance of risky tasks, such as changing positions and collecting secretions from the airways of patients. Thus, despite the importance of social support, it is necessary that the premises required by nurses are recognized and attended by their superior, such as the provision of places for rest, reduction of work shifts, guarantee of PPE and preservation of team’s constitution to ensure dialogue between its members, trust and reinforce resilience. |
| Managing mental health challenges faced by healthcare workers during covid-19 pandemic |
Greenberg et al, 2020 |
BMJ (Clinical research ed.) |
Health professionals are more susceptible to moral injury and to develop mental health problems due to actions in face of COVID-19. In this context, it is imperative that healthcare managers take actions aimed at the team’s well-being, be direct and sincere in order to maintain a bond of trust and reduce the caregivers’ tensions, be open to listening to the needs identified by them and promote a long-term psychological monitoring of caregivers in order to identify and treat such psychological problems. Employees who maintain a good relationship with each other are able to cope better with this moment, being important the maintenance of the team. |
| Considerazioni etiche, deontologiche e giuridiche sul Documento SIAARTI “Raccomandazioni de ética clinica per I’ammissone a trattamenti intensivi e per la loro sospensione, in condizioni eccezionali di squilibrio tra necessitàe risorse disponibili” |
Piccinni et al., 2020 |
Recenti Prog Med |
Because of the imbalance between the need and the availability of resources in ICU, the SIAARTI document guides the medical team’s approaches, relieving them of the responsibility regarding the reallocation of resources and exposing to society what criteria are evaluated in these decisions, such as patient's age, comorbidities and current prognosis; allowing the current medical conduct to be considered in the light of ethics and justice that focus on the possibility of saving the greatest number of patients who present clinical conditions for it, in view of the scarcity of materials and high demand experienced nowadays. |
| Psychological stress of ICU nurses in the time of COVID-19 |
Shen et al., 2020 |
Critical care (London, England) |
Because of the high workload, fatigue, disagreements with patients’ family members and social discrimination due to contact with Sars-CoV-2 carriers, nurses, especially the youngest, are more vulnerable to depression, anxiety, suicidal thoughts and low performance at work. To overcome this reality, psychological interventions, stimulating expression of feelings, familiarization with some procedures, encouraging social support, creating online groups to debate approaches and adapting working hours interspersed with leisure time are attitudes that are conducive to promoting mental well-being. |
| How Essential Is to Focus on Physician's Health and Burnout in Coronavirus (COVID-19) Pandemic? |
Shah et al., 2020 |
Cureus |
Naturally, doctors are the professionals with the highest rates of burnout, and COVID-19 is increasing the feeling of exhaustion and mental health problems, such as anxiety, in this group. Thus, the provision of subsidies to rest, study and protect the health of doctors is essential, associated with improved triage of patients, acquisition of updated guidelines directing conducts and new members to compose the medical team, as well as the promotion of telemedicine, telepsychiatry and support for resident doctors are ways to overcome the adversities experienced in this pandemic. |
| Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak |
Rana et al., 2020 |
Asian journal of psychiatry |
Fears, anxieties, panic attacks, social stigmatization, depressive tendencies and sleep problems are some manifestations that Pakistani doctors show and can last in the short- and long-term. Thus, to alleviate these negative conditions in the short term and promote mental health quality, hospitals have modified the shift system and offered accommodation and psychological counseling, while ways of screening these professionals are implemented for a long-term approach supported by a specialized mental health team. |
| Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis |
Pappa et al., 2020 |
Brain, behavior, and immunity |
After the start of the pandemic, the prevalence of anxiety in frontline workers is around 23.2%, while depression is 22.8% and insomnia, 38.9%. In addition, it is perceived that the subgroup of female nurses is the most affected compared to the male gender and to the medical staff. In this sense, the importance of promoting actions aimed at preserving the physical and mental health of caregivers is ratified. |
| The medico-legal implications in medical malpractice claims during Covid-19 pandemic: Increase or trend reversal? |
Zerbo et al., 2020 |
Medico-Legal Journal |
The difficulty faced in current public health encompasses structural issues, knowledge about the activity and manifestations of the coronavirus, shortage of PPE, little experience of the team in the management of the clinical conditions caused by COVID-19 and lack of ICU supplies for all patients. In this way, some medical practices considered neglectful, such as the reallocation of resources to save those patients with better clinical conditions at the expense of the others, are reviewed and must be adapted to the reality of crisis in which it is experienced. It is not appropriate, at this moment, to judge medical conduct based on a non-pandemic situation. |
| Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic |
Walton et al., 2020 |
European heart journal. Acute cardiovascular care, |
Acute stress reactions, moral injury, PTSD are some characteristics that the frontline team can reveal in this pandemic time; however, these manifestations must be approached with caution and should not be considered illnesses as they are typical attitudes of those facing a crisis situation. In this sense, promoting resilience and meeting the team's requirements, through open dialogue with health managers, is essential to overcome these impacts nowadays; associated with the creation of psychological support and screening networks during and after a pandemic to address the persistence of the psychological problems reported by these workers. |
| Mental health and emotional impact of COVID-19: Applying Health Belief Model for medical staff to general public of Pakistan |
Mukhtar, 2020 |
Brain, behavior, and immunity |
The belief model developed in Pakistan aims to promote and increase the resilience of the healthcare team, allowing them to face the adverse conditions of the new routine while the individual has the autonomy to perceive the conditions that can cause mental suffering, formulate ways to express your emotions and create tactics to overcome the obstacles found. |
| Management of icu nursing teams during the covid-19 pandemic. Gestión de los equipos de enfermerÃÂa de uci durante la pandemia covid-19 |
Raurell-Torredà, 2020 |
Enfermeria intensiva |
The disproportion in the number of patients seen during the pandemic and the small number of nurses is one of the main conditions that point to the exhaustion of these professionals. Thus, it is determined that a new dynamic should be carried out in order to equalize the amount of patients and nurses, as well as hiring of physiotherapists specialized in intensive care to reduce the amount of tasks performed by nurses. |
| Ethical recommendations for making difficult decisions in intensive care units in the face of the exceptional crisis situation due to the COVID-19 pandemic: rapid review and expert consensus |
Rubio et al., 2020 |
Med Intensiva |
The allocation of resources or the prioritization of treatment in ICUs becomes crucial elements, and it is relevant to have an ethical structure reference to be able to make the necessary clinical decisions. Thus, algorithms with norms are formulated to improve organizational conditions, availability of resources, characteristics and health status of the patients approached and ethical decisions made; such as the formulation of contingency plans, holistic analysis of the patient, not just considering biological age, and acting based on the principle of distributive justice and proportionality. |
| A cross-sectional study on mental health among health care workers during the outbreak of Corona Virus Disease 2019 |
Cai et al., 2020 |
Asian Journal of Psychiatry |
Frontline caregivers are experiencing a high tendency to psychological abnormality with a focus on interpersonal sensitivity and photic anxiety. Among the 1521 health professionals approached, it is noticed that such impacts are more common in individuals with less training and professional experience, being more dependent on maintaining resilience and social support as assistants in mental well-being. |
| Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19 |
Lian et al., 2020 |
Journal of Psychosomatic Research |
The use of self-assessment scales is a practical and low-cost method to assist in the screening of psychological manifestations such as anxiety and depression. It was perceived that, among doctors, those who are younger (age under or equal to 30 years old) manifest higher levels of depression, requiring greater attention and guidance from doctors to help face their fears and anxieties generated during work in this pandemic. |
| Mental health care for medical staff in China during the COVID-19 outbreak |
Chen et al., 2020 |
The Lancet. Psychiatry |
The institution of psychological approaches was not immediately accepted by medical teams, who denied that they were victims of the mental damage resulting from overwork during the pandemic. Therefore, it is important that health managers initially create an active listening approach to the difficulties faced by workers and, from there, formulate strategies consistent with the immediate needs of the team, such as availability of adequate places to stay during the pandemic period in order to maintain social isolation from the families and not affecting them with the coronavirus, as well as having a range of options in psychological approaches in order to allow each caregiver to choose for themselves the most comfortable way to participate in these activities. |
| The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus |
Kang et al., 2020 |
The Lancet. Psychiatry |
The situation of fighting coronavirus has caused stress, anxiety, depressive symptoms, changes in sleep, denial, anger and fear in medical teams. In view of this, instituting online platforms in order to provide psychological counseling, psychiatric care, exchange of ideas to manage critical patients and reduce the social distance from friends and family is an alternative to assist in the mental health care of these professionals, making it possible to avoid permanent psychic injuries and maintain good productivity. |
| SÃÂndrome post-cuidados intensivos después de la pandemia por SARSCoV- 2 |
González-Castro et al., 2020 |
Med Intensiva |
The coronavirus pandemic brings waves with an impact on global public health, starting with a high rate of morbidity and mortality due to the disease, impacts on the restriction of ICU resources and the interruption of care for patients with chronic diseases and, finally, the promotion of moral damages and psychological problems to frontline caregivers, with a significant increase in depression / anxiety and suicidal thoughts. |
| When health professionals look death in the eye: the mental health of professionals who deal daily with the 2019 coronavirus outbreak |
Neto et al., 2020 |
Psychiatry Research |
The stress arising from the health professionals’ activities in the fight against the coronavirus is associated with increased symptoms of anxiety, depression and physical and mental exhaustion. The ICU teams have a greater association with the aforementioned symptoms, given their contact with end-of-life patients, changes in the usual work structure and decision-making that is costly to the psychological structure of these workers in the face of resource reallocation during this crisis. In an attempt to reduce these consequences, creation of specialized networks for mental care, with psychologists and psychiatrists, willingness to use psychotropic drugs, improvements in working conditions and encouragement for team support are some suitable ways to overcome these impacts promoted by COVID-19 in the caregivers' psyche. |
| SARS CoV-2 (COVID-19): lessons to be learned by Brazilian Physical Therapists |
Pinto and Carvalho, 2020 |
Brazilian Journal of Physical Therapy |
In the face of a pandemic in which the majority of patients require ventilator management in ICUs, it is highlighted the importance of having physiotherapists specialized in intensive care as effective members of the multidisciplinary ICU team in the public health system, in order to improve dynamics in this environment, avoiding overload other professionals, and develop activities of continuous update on ventilator support and complications caused by the coronavirus. |
Table 1: Summary of main findings of the studies included for qualitative analysis in the systematic review based on the PRISMA method.
The impacts of COVID-19 nowadays include the social, political, economic areas and, especially, the whole society’s health. In terms of health, it is known that the pandemic is restructuring the individuals’ cognitive system regarding self-referential control of information and responses to the interaction of external social afferences and the physiological systems of the subject. Thus, the way the current reality is faced, in which the indecision of tomorrow, fear of death, mourning of loss, lack of freedom and internal anxieties are experienced in a unique way by each person, who automatically responds to the stimulus with a change in both physical and mental health [7].
In the face of this emotional pain, the feeling of guilt is humanly understandable. For the fact of witnessing unacceptable situations leads individuals to react, blaming themselves either for the choices made, or for the incapacity to perform some actions; such as looking for non-existent answers while blaming the activities of others, for example, government actions or new medical guidelines [10]. In this perspective, it is seen that the paradox of negative and positive emotions co-exists and the psychic-organic integrity is determined by the way in which each one feeds these emotions. In this sense, not everyone submitted to the same stressor will respond negatively; however, everyone involved is vulnerable, especially those who are on the frontlines in the confrontation against COVID-19 [14].
For army doctors, maintaining sanity is the result, among many aspects, of the number of battles experienced. In this way, the most relevant characteristics of the group in question is to promote the psychophysical protection of the patient, exercise the most humanized care, select the severity of each situation in the light of current scientific knowledge and act with the greatest efficiency in serving as many people as they can help [15]. However, we are experiencing a global health crisis that most closely resembles a war, in which the best prepared fighters are less susceptible to mental damage, while those who are facing their first battle suffer early, particularly nurses [13].
In view of that, ever since the COVID-19 pandemic appeared, the imbalance between the need and availability of resources marks all areas of medicine, especially in intensive care. ICU workers are playing the role of heroes and victims. As they fight for the lives of their patients, the change in routine has had a negative impact on their health [15]. The increase in the workload of doctors and nurses [13,16,17] associated with the exorbitant function of breaking bad news [10,14] are being associated with changes in the sleep-wake cycle, with reports of insomnia [7,17]. This, in turn, has an impact on the poor development of work activities marked by physical and psychological exhaustion [10,12,16,18].
In an associated way, the lack of personal protective equipment (PPE) is a coefficient of anxiety and fear experienced by the frontline team [12,13,16,18]. In this circumstance, the restrictive measures for release of PPE and screening tests created by the United Kingdom were interpreted by second-line nurses as a discriminatory act [Maben and Bridges, 2020]. In view of this, there is an intimate exposure of workers to the virus, which put their lives at risk by maintaining the health of others. It is known that in pre-pandemic stressful situations is common to seek support and comfort in the family. Nowadays, however, for fear of exposing their families to COVID-19, the ICU team is performing self-isolation, aggravating the reduction in social support and resulting in negative repercussions on the team [3,8,10,13,16-20].
At the same time, the increasing number of deaths [10], reinforced by the news of co-workers’ positive diagnosis or deaths, are commented by the current literature as accessory causes of the ICU team’s psychic condition [8,12,20]. Nevertheless, this group of professionals with relevance to nurses, have been victims of social stigmas for being considered carriers or vectors of the coronavírus [10,12,13].
At the same time, although PPE are fundamental for the prevention of the disease, doctors and nurses have reported difficulty in communicating with patients due to the use of these tools [17,21]. Despite that, moments of conflict are extended beyond the doctor-patient binomial, for, in view of the high infectivity, the hospital team follows new guidelines that establishes to be impractical to maintain the practice of family visit to the admitted patients, as well as abolishes the presentation of the deceased to relatives. Thus, disagreements arise between the patient's family, motivated by premature grief, and the ICU team [10,16,22].
Thus, caregivers at the ICU are seen by patients as the only human and affective bond in the midst of the impossibility of contact with their loved ones. This fact is relevant for both parties; as patients create insecure patterns of affable support in care professionals, these develop sentimental links to those. So when there is evidence of healing of someone admitted to the ICU, it is cause for celebration and joy for all who followed this process closely. However, the ineffectiveness of the therapies performed and the clinical decline of a patient promotes pain, grief and anguish in everyone at the ICU who no longer look at that individual as a mere patient, but as a member of the new family cycle created in the midst of the melancholy reality of COVID-19 [10,13,20].
In addition, most nurses report difficulties in adapting to the new protocols of the ICU services, which have become more rigid in view of the current situation [10,12,13]. This scenario is correlated to the multiple tasks that these professionals perform and to the unbalanced distribution of patients under the supervision of a professional [7,17]. For, in usual ICU conditions, the ratio is one nurse to two, or even four, patients and other auxiliary nurse to every 4 beds with the function of giving support due to the excessive workload or in case of any changes due to a professional getting sick [14,21].
In the meantime, a criticism mentioned by the Spanish Society of Intensive Nursing and Coronary Units concerns the lack of recognition of the specialty of this group in intensive care and the negligence from the services in hiring a sufficient number of physiotherapists, usually with one physiotherapist per unit who also suffers with work overload [22,23].
However, in a conflict situation, the existence of an effective leadership is imperative. Thus, another relevant complaint from the ICU team is the negative leadership of managers in certain sectors and, even with increased hours and workload, the financial reward is considered insufficient [17].
At the same time, fear of lack of technical skills and the incomplete knowledge about SARS-CoV-2 virus are expressive coefficients in the mental well-being of caregivers [10,17]. To portray these aspects, a study in Turkey involving 346 people, including anesthesiologists and residents of the area, stated that the residents called to act in the ICU against COVID-19 were more indecisive, with a tendency to make wrong decisions as a consequence of little professional experience [1]. A similar situation occurred with the pediatric ICU team from a hospital in Massachusetts, which started to accommodate COVID-19 positive adult patients. In addition to the lack of information related to the disease in question, these professionals were also challenged in the management of patients with biotype and clinical and laboratorial parameters completely divergent from the usual [5].
On the other hand, the reorganization of the physical spaces of the ICUs directly influences the team dynamics. This is due to the fact that many professionals were relocated to other ICUs, having to work with individuals who were not their fellow team members, and due to new employments for supplementation of the teams. Such factors made the old team feel uncomfortable with the new members, with whom they did not maintain a cohesive bond in the coexistence relationship, with reports of not feeling comfortable to talk about their own emotions, feeling ashamed to question and fear of making a mistake in order to not being judged [10,13,20].
However, one of the main factors in the mental integrity of frontline caregivers is the new ethical dilemmas that the pandemic has brought. Physicians mainly have their cognitive abilities and memory required repeatedly, and in a quick way, under circumstances of high psychological tension; resulting in the common selflessness of these workers regarding their own health [10,12].
In this circumstance, the allocation and screening of resources for the management of the patient in the ICU generates uncertainties and self-questions by doctors about the principles that govern their activity. Thus, acting with justice is not only giving the sick person access to available therapies, but also rationalizing resources. Therefore, some ethical criteria, such as beneficence, non-maleficence, autonomy of patient to make decisions and shared justice, assist in the selection of beneficiaries to use the ICU. However, the pandemic means that these parameters can no longer be reconciled, causing stress to the doctor. Many professionals revealed that the level of management uncertainty is proportional to the clinical complexity of the patients. Thus, for them it is considered as an attitude of high negative psychological impact the suspension of ventilatory support therapy in ICU, in comparison to not activating it and not aggregating the patient in this environment [24,25].
Ratifying this reality, several institutions are screening health professionals to assess the psychic impacts of the pandemic. A cross-sectional survey using the Connor-Davidson resilience scale (CD-RISC) and the Social Support Rating Scale (SSRS), applied to 1521 professionals, obtained a 14.1% prevalence of psychological imbalances [26]. Similarly, a Chinese hospital using the Zung Selfrated Depression Scale (SDS) and the Zung Self-rated Anxiety Scale (SAS), in a group of 23 doctors and 36 nurses, revealed that doctors under the age of 30 years had high scores for depression compared to older people [27].
Therefore, it is clear that the consequences of COVID-19 in the ICU team are diverse. Among the reported outcomes, stress, anxiety, depression, anguish, anger, fear, guilt, insomnia and substance abuse are found [4,12,18,28-30] as well as deficit in labor productivity [14] and manifestations of compulsiveobsessive behaviors, such as excessive hand washing [26]. In this sense, a study evaluating the mental integrity of 85 nurses at the ICU had as a quotient that 59% had reduced eating habits, 55% fatigue, 45% problems related to sleep, 28% irritability, 26% constant crying and 2% suicidal ideations [16].
However, the high predisposition for suicide among doctors is a recognized fact. In the United States, the percentage of doctors showing typical burnout symptoms reaches 54.4% [17]. In this sense, the fear of discrimination and of being labeled, associated with the feeling of shame and denial, lead doctors to avoid talking about their feelings and stressors; as well as not seeking psychological and psychiatric support. Therefore, these attitudes are decisive in the bad outcomes observed on this group [14,18].
Even so, the feeling of guilt is not restricted to the team that actively works at the ICU. That is, the risks are beyond the walls of this environment. Since the professionals of this site, which have underlying diseases or pregnancy status, and were dismissed from their employment practice, refer guilt for not being there during this pandemic time. In addition, the risk of developing PTSD in the ICU team is above 10% of the range considered normal [21]. Moreover, young female frontline caregivers exercising the position of nurses, when compared to doctors, showed more frequent symptoms of anxiety, depression and PTSD; unlike second-line professionals, who show conditions similar to Munchausen syndrome by proxy [10].
In view of this situation, a systematic review with a meta-analysis of 13 cross-sectional surveys and a total of 33062 participants was carried out to assess the prevalence of anxiety, depression and insomnia in health professionals. It was found that, while the Chinese population during the same period of study had fluctuating rates of 22.6%-36.3% for anxiety and 16.5%-48.3% for depression; caregivers had similar figures for anxiety (23.2%) and depression (22.8%); in addition to an average 38.9% prevalence of insomnia after the emergence of the pandemic. In addition, it clarifies the high prevalence of psychological problems in nurses by justifying that the majority of the members of this profession are women; but also because of the more intimate contact with the patient and the routine performance of invasive procedures, such as sputum collection [19].
Despite these alarming data, not everyone who makes up the ICU team will develop such conditions. That is, while it is relevant to screen and evaluate the current psychological situation of frontline caregivers, the individual's physiological responses, such as fear and anxiety, when exposed to a stressful situation should not be conceptualized as a disease. Therefore, even though everyone experience a challenging time, either in your activity, or in their personal integrity, many professionals exhibit resilience and, consequently, the chance of development or persistence of psychic-organic changes in the long-term is small [13,21].
Thus, resilience is defined as the human capacity to face and recover from significant tribulations. Therefore, the characteristics expressed by resilient people are resistance, perseverance and hope. This demonstrates that psychological resilience is a protective factor, acting as a means of primary prevention, against mental pathologies and has the result of enhancing the individual in the face of adversity [11,26].
In this sense, when studying psychological stress in 2110 medical teams and 2158 students called to act against COVID-19 in Wuhan, it was noticed that the first one showed a feeling of confidence superior to the second ones [7]. Such figures validate the hypothesis that the relationship between resilience and mental health is attenuated as the subject ages. In other words, middleaged professionals are less dependent on this aspect, given that greater technical experience, longer employment and having experienced previous outbreaks and epidemics have conditioned a mental state less susceptible to stress and fear. On the other hand, younger people show more anxiety-depression disorders, but with a greater willingness to actively seek help from mental services. In this way, young professionals are more likely to be conditioned to increase their resilience through techniques for managing stress and meditation, being, therefore, a priority group in the actions developed to improve the psychic-organic health of the ICU team [11].
At the same time, another factor related to resilience is social support. In this logic, social support denotes the judgment or experience that the individual has of belonging to a group of people who help each other in a reciprocal way. Therefore, the maintenance of the integrity of the ICU team is a reason that helps to raise the levels of individual resilience, since the friendship with more experienced colleagues makes the caregivers believe in the possibility of obtaining the necessary help to face their stressors, increasing, consequently the belief that they can face adversity. Therefore, cohesion between colleagues and their respective managers is decisive in the way in which the coronavirus will act in the resilience and health of these people [5,11,13,25,26].
Based on the discussion above, health systems take daily actions to prevent psychological damage to their members. One of the main actions is to encourage social support, whether by family members of caregivers or by their bosses. The best way to shorten social distance and avoid viral spread is through online methods, such as video calls [7,12,16,21]. At the same time, good leadership should be encouraged based on active communication between boss-workers, in which fair leaders are considered to be ones who shares their knowledge, anxieties and doubts in a honest way and showing empathy to others; as well as the ones that stimulate the encouragement of their workers to maintain self-care and permeates humanity and humility in their attitudes [7,12,17,21]. In view of this, the effectiveness of trying to maintain the current team is undeniable [3,5,13,16]. In case it is not possible, hiring new members should be done in association with actions that make them familiar with the team and service dynamics [17]. Thus, it is noticed that it is not necessary to have a vast apparatus to improve positively the frontline team performance, with reports in Chinese works of feelings of gratitude from nurses towards the general public who donated them hand moisturizers [10,13].
In addition to these changes, other alternatives are suggested by health workers. Commonly to all, hospitals are asked to provide adequate rest spaces for the teams who try to maintain family isolation and do not have other places to rest [3,18,19,21,28]. Added to that, it is suggested a redefinition of the equivalence between patients and nurses, seeking proportions such as 1:1 or 1:2, respectively, as well as the stimulus for hiring physiotherapists specialized in intensive care [23].
In view of that, several CTIs readjusted their shift dynamics. Thus, a shift rotation model was adopted in which every 4-6 hours of continuous work, caregivers must rest [29,30]. At the same time, the reduction in daily working hours to less than 16h per day revealed a decrease of 18% in the rate of medical errors. Among the suggested mechanisms to reduce stress, the practice of drawing, talking, singing, exercising, breathing deeply and looking out the window were well accepted [31].
At the same time, to solve the insecurity of technical and scientific knowledge, refresher courses are carried out. In this way, as indicated by workers, hospitals provide courses on equipment management, biosafety and training for physiotherapists on the best parameters in the approach to patients in mechanical ventilation [32]. As for the group of physicians residing in anesthesiology, the focus is on offering simulations directed to the techniques of orotracheal intubation and other tasks specific to the specialty. Not being enough, many hospitals also develop education courses in palliative care, helping teams to have a management that is more humanized and appropriate to the patients' emotional state.
Despite that, specialized support for the ICU team’s mental care is necessary. In this context, the mental health team is composed of a psychologist, psychiatrist and family members of the professionals. Some measures are recommended in order to achieve therapeutic success, such as starting the therapy process in spaces considered comfortable and reminiscent of good feelings, in order to obtain confidence in the tasks to be performed, and to encourage teams to perform functions in pairs with the objective of exchanging emotional experiences or doubts about the job between those have a friendly relationship. It is also essential that each team has its own psychologist, either for individualized approaches or for group actions.
However, management through virtual platforms is best indicated for caregivers won by the trust of their therapists or in situations focused on discussing common challenges for the team. It is relevant to emphasize that not all caregivers immediately accept psychological help due to the prejudices and fears brought with them. Thus, there may be obstacles in the implementation of this approach which need to be analyzed and corrected according to the subject's particularities. In addition, it is necessary to demystify and offer to everyone, through telemedicine, consultations with psychiatrists and the use of psychotropics, if necessary [31].
In order to preserve mental integrity, several psychological approaches are reported in the literature. The coping model based on anticipating, planning and deterring serves the same purpose as the health belief model applied to ICU teams in Pakistan. This psychotherapeutic instrument offers the individual the possibility of identifying situations of susceptibility, assessing its severity, perceiving which factors are threatening, looking for what barriers exist and the benefits arising from overcoming them and, finally, stratifying the ways they will use to cope. Therefore, the primary focus of psychological therapies is to act as a means of primary prevention of the impacts generated by COVID-19 on mental health, promoting in caregivers the maintenance of resilience [32].
Despite that, the impact on medical ethics generated by the coronavirus is substantial. In an attempt to improve the moral damage to the ICU doctors, several hospitals create guidelines to guide decisions; it is also relevant that the institutions’ leaders reinforce that the medical decision is not an individual attitude, but the result of the ideals of a team. In view of that, one of the documents used as a reference is the one by the Italian Society of Anesthesia Analgesia Reanimation and Intensive Care (SIAARTI).
This document, published in an update on 06/03/2020, draws up guidelines for hospitalization of patients in ICU, as well as the discontinuation of therapies in the face of imbalance between their availability and insufficiency. Through these paths, it is possible to relieve doctors of their responsibilities, which, nowadays, are emotionally expensive; and also to make it explicit the tactics for allocating instruments at a time of unavailability.
Finally, it is relevant that these actions are no longer harmful to the health of the ICU team. In this view, all the measures that the services perform need to be adapted to the reality and immediate need of the professionals. Taking psychological stress into account, psychological interrogations reveal a poor prognosis when compared to the benefits brought by the institution of desensitization and mental reprocessing practices. Thus, it was seen in the literature that caregivers stated that they dislike selfquestioners, for the reason that they prefer passive reception of information made available for long periods for personal use when required, rather than being tested.
Therefore, it is imperative to monitor the ICU team. In this circumstance, nowadays, it is necessary to identify the most affected or susceptible individuals in order to work on methods of primary prevention of mental damage. At the same time, this monitoring should be extended to post-pandemic periods, in order to hierarchically screen professionals; that is, giving priority to the frontline team. Thus, from this moment on, one can freely use questionnaires aimed at identifying characteristic manifestations of anxiety, depression, exhaustion, mental impact and suffering for the psychic vulnerability resulting from calamities such as the current one is a provider for pathological grief and PTSD. Therefore, an extra investment is needed to properly carry out psychological follow-up from 6 to 12 months post-pandemic.
Limitations
Among the limitations found in the preparation of this work, the small number of published studies with the application of standardized questionnaires for the assessment of the psychological consequences in the evaluated subjects stands out, resulting, consequently, in heterogeneous results. In addition, some studies have their methodology based on the acquisition of self-reports and this can be a bias factor, so their results should be analysed with caution. In this sense, future research must be carried out in order to demonstrate the ways in which the protection actions aimed at the medical team are having effects, such as a more detailed assessment of the physical, mental and social repercussions that the pandemic will promote in the lives of these individuals.
Conclusion
During the COVID-19 pandemic period, the structure of ICU activities changed rapidly. The medical team in this environment is the first to suffer the consequences that this disease promotes. The disproportion between the need for technological supplies in intensive care and their scarcity promotes, among many factors, psychological stress. Anxiety, irritability, insomnia, fear and anguish are some sensations experienced by this group. In this sense, promoting actions with the purpose of mitigating such psychic-organic impacts is essential. In addition, such care should be maintained and screening for mental illness in this group in the post-pandemic period should be carried out in order to identify and reverse these consequences as soon as possible.
Funding
The Suicidology Research Group from Universidade Federal do Ceará (UFC) and Brazilian National Council for Scientific and Technological Development (CNPq) – institution linked to the Brazilian Department of Science, Technology and Innovation to encourage research in Brazil.
Conflicts of Interests
All the authors have declared that they have no conflict of interest
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Acknowledgements
Department of Health Science, Medical School, State University of Santa Cruz, Ilhéus, Brazil and Medicine/Universidade Federal do Cariri –UFCA.
34394
References
- Dost B, Koksal E, Terzi Ö, Bilgin S, Ustun YB, et al. (2020) Attitudes of Anesthesiology Specialists and Residents toward Patients Infected with the Novel Coronavirus (COVID-19): A National Survey Study. Surg Infect (Larchmt) 21: 350-356.
- Raurell-Torredà M, Martínez-Estalella G, Frade-Mera MJ, Carrasco Rodríguez-Rey LF, Romero de San Pío E (2020) Reflexiones derivadas de la pandemia COVID-19. Reflexiones derivadas de la pandemia COVID-19. Enferm Intensiva 31: 90-93.
- Zaka A, Shamloo SE, Fiorente P, Tafuri A (2020) COVID-19 pandemic as a watershed moment: A call for systematic psychological health care for frontline medical staff. J Health Psychol 25: 883-887.
- Senni M (2020) COVID-19 experience in Bergamo, Italy. Eur Heart J 41: 1783-1784.
- Yager PH, Whalen KA, Cummings BM (2020) Repurposing a Pediatric ICU for Adults. N Engl J Med 382: e80.
- Romanò M (2020) Fra cure intensive e cure palliative ai tempi di CoViD-19. Recenti Prog Med 111: 223-230.
- Wu W, Zhang Y, Wang P, Zhang L, Wang G, et al. (2020) Psychological stress of medical staffs during outbreak of COVID-19 and adjustment strategy. J Med Virol 92: 1962-1970.
- Santarone K, McKenney M, Elkbuli A (2020) Preserving mental health and resilience in frontline healthcare workers during COVID-19. Am J Emerg Med 38: 1530-1531.
- Ferreira MA, Carvalho Filho MA, Franco GS, Franco RS (2020) Profissionalismo Médico e o Contrato Social: Reflexões acerca da Pandemia de COVID-19. Acta Med Port 33: 362-364.
- El-Hage W, Hingray C, Lemogne C, Yrondi A, Brunault P, et al. (2020) Les professionnels de santé face à la pandémie de la maladie à coronavirus (COVID-19): quels risques pour leur santé mentale?. Encephale 46: S73-S80.
- Hou T, Zhang T, Cai W, Song X, Chen A, et al. (2020) Social support and mental health among health care workers during Coronavirus Disease 2019 outbreak: A moderated mediation model. PloS one 15: e0233831.
- Blake H, Bermingham F, Johnson G, Tabner A (2020) Mitigating the Psychological Impact of COVID-19 on Healthcare Workers: A Digital Learning Package. Int J Environ Res Public Health 17: 2997.
- Maben J, Bridges J (2020) Covid-19: Supporting nurses' psychological and mental health. J Clin Nurs 29: 2742-2750.
- Greenberg N, Docherty M, Gnanapragasam S, Wessely S (2020) Managing mental health challenges faced by healthcare workers during covid-19 pandemic. BMJ (Clinical research ed.) 368: m1211.
- Piccinni M, Aprile A, Benciolini P, Busatta L, Cadamuro E, et al. (2020) Considerazioni etiche, deontologiche e giuridiche sul Documento SIAARTI “Raccomandazioni de ética clinica per I’ammissone a trattamenti intensivi e per la loro sospensione, in condizioni eccezionali di squilibrio tra necessità e risorse disponibili”. Recenti Prog Med 111: 212-222.
- Shen X, Zou X, Zhong X, Yan J, Li L (2020) Psychological stress of ICU nurses in the time of COVID-19. Crit Care 24: 200.
- Shah K, Chaudhari G, Kamrai D, Lail A, Patel RS (2020) How Essential Is to Focus on Physician's Health and Burnout in Coronavirus (COVID-19) Pandemic?. Cureus 12: e7538.
- Rana W, Mukhtar S, Mukhtar S (2020) Mental health of medical workers in Pakistan during the pandemic COVID-19 outbreak. Asian J Psychiatr 51: 102080.
- Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, et al. (2020) Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun 88: 901-907.
- Zerbo CBS, Perrone G, Malta G, Argo A (2020) The medico-legal implications in medical malpractice claims during Covid-19 pandemic: Increase or trend reversal?. Med Leg J 88: 35-37
- Walton M, Murray E, Christian MD (2020) Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur Heart J Acute Cardiovasc Care 9: 241-247.
- Mukhtar S (2020) Mental health and emotional impact of COVID-19: Applying Health Belief Model for medical staff to general public of Pakistan. Brain Behav Immun 87: 28-29.
- Raurell-Torredà M (2020) Management of ICU nursing teams during the COVID-19 pandemic. Enferm Intensiva 31: 49-51.
- Gestión de los equipos de enfermería de UCI durante la pandemia COVID-19. Enfermería Intensiva 31: 49-51.
- Rubio O, Estella A, Cabre L, Saralegui-Reta I, Martin MC, et al. (2020) Recomendaciones éticas para la toma de decisiones difíciles en las unidades de cuidados intensivos ante la situación excepcional de crisis por la pandemia por COVID-19: revisión rápida y consenso de expertos. Med Intensiva 44: 439-445.
- Cai W, Lian B, Song X, Hou T, Deng G (2020) A cross-sectional study on mental health among health care workers during the outbreak of Corona Virus Disease 2019. Asian J Psychiatr 51: 102111.
- Liang Y, Chen M, Zheng X, Liu J (2020) Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J Psychosom Res 133: 110102.
- Chen Q, Liang M, Li Y, Guo J, Fei D, et al. (2020) Mental health care for medical staff in China during the COVID-19 outbreak. Lancet Psychiatry 7: e15-e16.
- Kang L, Li Y, Hu S, Chen M, Yang C, et al. (2020) The mental health of medical workers in Wuhan, China dealing with the 2019 novel coronavirus. The lancet. Psychiatry 7: e14
- González-Castro A (2020) Síndrome post-cuidados intensivos después de la pandemia por SARSCoV- 2. Med Intensiva 44: 522-523.
- Neto M, Almeida HG, Esmeraldo JD, Nobre CB, Pinheiro WR, et al. (2020) When health professionals look death in the eye: the mental health of professionals who deal daily with the 2019 coronavirus outbreak. Psychiatry Re 288: 112972.
- Pinto TF, Carvalho C (2020) SARS CoV-2 (COVID-19): lessons to be learned by Brazilian Physical Therapists. Braz J Phys Ther 24: 185-186.


