Keywords
supportive supervision, supervisors, health workers, Record Keeping
Introduction
Supervision is one of the most relevant tasks in health systems management [1] and is particularly essential to enhance delivery of quality services [2]. In low-income settings supervisors are pivotal to the performance of health workers as sometimes they are their only link with the health system [3]. However, too often they lack skills, useful tools, transportation, and are burdened with administrative duties [2,4]. In these contexts, HRM practice (such as supervision, training and promotion) is often reduced to mere ritual [5] and supervision takes the limited form of inspecting performance against checklists, a process characterised by fault finding and reprimanding [2]. Improving the attitudes of supervisors towards health workers and the quality of their interactions, using the existing workforce, is a relatively inexpensive approach [6]. Previous interventions aimed at improving supervision tend to focus on training supervisors alone, an approach that has proven less than effective in improving performance [7]. If properly done, supervision can provide professional development to health workers, improve motivation as well as job satisfaction [8].
Health programmers and providers are increasingly favouring other forms of supervision that focus on addressing problems in service delivery [9]. Supportive supervision is one such approach and is defined as “an approach to supervision that emphasizes joint problem-solving, mentoring and two-way communication between the supervisor and those being supervised [2]. Evidence from programme evaluations and research studies in various countries suggests that supportive supervision promotes service quality. In six countries– Bangladesh, Brazil, Honduras, Kenya, Nepal, and Tanzania–the introduction of supportive supervision as part of service improvement initiatives yielded promising results in both service quality and provider performance [2]. In particular multifaceted interventions, for example training plus supervision, which address multiple determinants of performance, can increase the capacity of supervisors to support their staff [10]. A rigorous evaluation carried out in Kenya to reinforce adherence to supportive guidelines after health workers took part in training and workshops resulted in significant gains in the knowledge and practice scores gained, compared to those gained through training alone [11]. Similarly, an intervention in Honduras that incorporated participatory workshops with supervisors to develop vision and strategies of supervision resulted in increased open dialogue between supervisors and supervisees leading to high achievement of performance goals [8]. Increasing the frequency and duration of supervision, changing activities assumed during supervision, involving multidisciplinary teams in supervision, as well as incorporating tools such as guidelines and checklists are more likely to improve performance than single interventions [2].
Tools and techniques of supportive supervision, such as structured guidelines for external supervision and selfassessment instruments, are readily usable by health workers and supervisors in a wide range of settings [12]. National guidelines for supervision are in place in most low income settings [13,14] but studies show that the use of such tools during supervisory visits is more the exception than the rule [4]. Guidelines and checklists can support supervisors to understand what they are to do and how to do it and can facilitate supportive supervision to assess working conditions and the technical competence of staff [2]. Studies from low-income settings indicate that structured observation using checklists and immediate feedback can result in improved performance [11]. But while such tools can be effective in systemizing supervision, they may actually hinder supervision, particularly if they are lengthy leading to fatigue and mechanical use [4,15]. For example, study conducted with supervisors in Zimbabwe to measure the quality of supervisorprovider interactions concluded that supervisors viewed checklists as inventory tools and hence tedious and unnecessary for routine supervision [4]. The use of guidelines and checklists may support the supervision process, but may not be enough to effect change in the long- term, unless complimented with agreed set of priorities, budget, follow-up, audit and feedback to lead to changes and influence performance [16].
Good record-keeping is fundamental to professional practice but often regarded as tedious and left to be done at the end of a shift. Lack of records, for example absentee registers for staff is common. Absenteeism is a major problem; key staff members may spend most of their time attending trainings or report ill frequently [17] resulting in low health worker performance and outputs. Inadequate staffing levels may be compounded by a high level of absenteeism which reduces access to services [18]. It has been noted that a fair and accurate performance review may begin with tracking employee behaviours and patterns [19] for example introducing registers of arrival and departure time. Adequate supervision could reduce absenteeism and mitigate some factors that reduce health workers productivity [20]. The application of health worker management strategies through supportive supervision, improved supply of essential goods and integrated on the job training could reduce absenteeism and non- productivity [20]. Staff training, monitoring and regular supervision are important to successful improvement in records keeping.
Productivity of health staff in developing countries is often described as sub-optimal and that personnel are under-utilized [21,22]. A shortage of employees particularly in developing contexts means that available professionals are often deployed to work in areas not related to their skills. This represents a form of wastage, especially if shortages of those skills exist in the country [17]. Health workers’ job descriptions are often unavailable [18] and workloads do not match staffing levels [17]. A substantial portion of staff time may be spent on administrative duties [17] as opposed to treatment and caring activities [22]. A study from Malawi reported that many staff and facilities in their study lacked written job descriptions and, even when present these tended to be generic [23]. But even when job descriptions are available other studies [24] have found that the actual tasks staff did were not necessarily reflected in these documents [23].
The objective of this study was to assess the effect of supportive supervision strategy on implementation of HRM processes following a cluster controlled trial intervention, STEM (Support, train and empower managers). This approach differed from other supportive supervision approaches in two ways. First, it addressed the role of managers in motivating and retaining staff, an aspect that has largely been ignored in pervious interventions, and second, the STEM intervention specifically addressed managers’ performance, an aspect still relatively rarely addressed in resource constrained settings. This intervention sought to show that it is possible to improve the working environment by targeting managers and their approach to HRM. Our systematic approach was informed by the Medical Research council’s synthesis of best practice approach in the development, implementation and evaluation of complex interventions [25]. As this was a complex trial with multi-level quantitative and qualitative measures, it would have been impossible to report all the results in one paper and hence this study focuses on the perceptions of supervisors on the implementation of supportive HRM processes and how these influenced the supervision practice. The study reports on the implementation of the following processes: supportive supervision guidelines; job descriptions for staff; personnel files, and absenteeism registers, processes that were deemed most effective in improving the supervision process.
The situation in Tanzania
In Tanzania, mid-level cadres are well established within the public health systems and studies provide strong evidence for their clinical efficacy [26] and economic value [27]. However, Tanzania’s health system faces several constraints; The country has a health worker shortage, and has documented problems with health worker motivation [28] heavy workload for providers [29] and marked inequalities in the distribution of health workers are prevalent in terms of per capital distribution and rural urban imbalances [30,31]. The country reports an average of 1.4 health workers per 1000 people in the country, but this varies greatly between districts [31]. Factors including low output of new health workers by medical schools, out migration of health workers to other sectors or more lucrative countries, or remuneration and adverse working conditions [32,33] are attributable to health worker shortage and performance. In Tanzania, supervision at the regional level is supported by Council Health Management Teams (CHMTs) and supportive supervision is viewed as a necessary part of HRM process [23]. But effective integration and implementation of supportive supervision still remains a challenge [34]. Recent studies showed that health workers complained that the supervision was not supportive as it only engaged with the person in charge and did not provide direct feedback to other health workers. CHMTs face various challenges in providing supportive supervision to peripheral health facilities including workload, staff shortage, financial constraints, and lack of vehicles or even unavailability of fuels. Improved supervision is likely to require timely disbursement of funds, sufficient staff, prior notification of visits, appropriate training for supervision and improved supervision of CHMTs by regional and national level staff [18].
To address the human resource constraints Tanzania has adopted various strategies: The Tanzanian HRH Strategic Plan (2008-2013) committed to targeting urgent performance management and productivity issues by focusing on improved supervisory support and employee relations [35]. In addition the Open Performance Review and Appraisal System (OPRAS) for the public service was introduced, to provide an open, formalised system for benchmarking and assessing staff performance [35]. Tanzania’s new supportive supervision guidelines [13] underline supportive supervision which is based on utilising problem solving as an approach to improving quality and meet the client needs. The guidelines contain information for assisting health care providers and supervisors to conduct supervisory activities. A study focusing on supervision in Tanzania noted that a supervision matrix and checklist based on these national guidelines checklists was not comprehensive enough to cover all necessary aspects, or lacked sufficient space to adequately capture all the issues. In addition job descriptions are not widely available and performance indicators not generally agreed in Tanzania. In addition, although job descriptions were provided, the actual tasks staff did were not necessarily reflected in these documents [23]. A key lesson from successful quality and performance improvement interventions is that for change to be sustained and institutionalized there must be an internal enabling environment conducive to initiating, expanding, and sustaining the change [2].
Methods
Study design
To address the gap between HRM policy and practice we designed a cluster controlled trial intervention, STEM (Support, train and empower managers), to provide a structure and skill set that would put HRM policies into practice, with follow up, monitoring and evaluation informing subsequent practice. The trial was designed as a focused, intense, systematic effort to improve support and supervision and to measure the impact of this improvement. The intervention was described as follows; element a) entailed workshops with the reproductive and child health personnel on the District Health Management Teams (DHMT) and obstetric care facility managers on HRM - raising awareness of importance of HRM and increasing skill levels in planning, monitoring and controlling of HRM activities, b) entailed intensive training in supervisory and support skills for managers directly engaged in supervision, both at district and facility level and c) Action learning sets (ALS) for staff at district and facility level engaged in supervision and mentoring of emergency obstetric care health workers. A learning set is a group comprising 5 to 8 people, who meet regularly to support one another in their learning in order to take purposeful action on work issues led by a professional set facilitator. The purpose of these facilitated learning sets was to support collaborative learning and problem solving and support supervisors in the implementation of the framework. In two districts all facilities received elements a) and b); two districts received elements a), b) and c. The project was implemented in Tanzania by Ifakara Health Institute in collaboration with the Centre for Global Health, Trinity College Dublin, Ireland. The project then carried out an evaluation 12 months post intervention to evaluate the changes in supervisory experience and service delivery employing both quantitative and qualitative methods.
Study setting
The study was carried out in three geographical regions - Iringa, Tabora and Tanga in Tanzania. These three regions were selected on the basis of previously collected data measuring the average level of job satisfaction with supervision in the facilities within those regions. This data enabled us to categorise regions according to high, medium, or low health worker satisfaction. Within each region we conducted a cluster controlled trial, assigning two districts as control districts. We selected a further 4 districts within each region for the intervention. In each of these districts all facilities providing emergency obstetric care were included in the study. A total of 45 health facilities were sampled 15 from each of the three geographical regions. Within each region, five health facilities were sampled from each of three districts. The sampled health facilities included 21 health centres and 24 dispensaries.
Research participants
Research participants comprised only supervisors that had been part of the STEM intervention. A total of nine focus group discussions (FGDs) were conducted, six in a+b+c districts and three in a+b districts. The sample comprised 48 respondents with 4-8 participants per focus group and included clinical officers, registered nurses/midwives and elementary level cadres (medical attendants/MCH aides, enrolled nurses/midwives). The FGDs were conducted by a STEM research officer with one of the research assistants doing the note taking. Research assistants were recruited from Ifakara Health Institute (IHI) and selection was based on a good track record on previous research projects, good computer skills and experience with both qualitative and quantitative data collection including a good command of both English and Swahili.
Data collection
This exploratory mixed-methods study was carried out as part of the larger STEM project with supervisors who had taken part in the STEM intervention. We employed focus group discussions (FGDs) as we were interested in learning about supervisors’ interpretations of the STEM intervention as a group and on interpretations of events that reflect group input [36]. One of the indicators was evidence of facility managers implementing HRM policies in their facilities following the intervention and hence it was decided that the most effective way to measure this was to collect data directly from facilities and at district level on the types of HRM processes in use. To supplement FGDs data, facilities were presented with a list of processes and were asked whether the listed HRM policies/processes were currently operational and if they had been added or revised during the STEM project’s lifetime. The FGDs data also served to validate quantitative data [37] collected as part of the larger study. A reflective meeting was conducted every evening with research team to discuss the progress, challenges, and the way forward. The feedback from the research assistants indicated that most questions were easily understood without clarifications from the interviewer.
The interview guide was grouped into eight sections with a set of open-ended questions. The questions were designed to generate discussion on the impact of being part of STEM on the supervisor’s practice and on internal supportive supervision systems/processes at facility level. The key thematic areas related to supervisory practice and skills; impact on relationships, communication, leadership and authority; changes to internal supportive supervision practices in the facility; and perceptions of the utility of the ALS. At the time of data collection the intervention had been running for 12 months and data collection took place from 23rd March 2014 to 24th April 2014 (Figure 1).
Data analysis
The FGDs were carried out in the local language Swahili and each interview was recorded transcribed and translated to English by research assistants fluent in both languages. The information from the transcripts was analysed using themes which derived from the research questions and prompts developed in the interview guide, and some which emerged from the analysis itself. The research notes were managed and analysed in QSR International’s NVivo software, using thematic analysis. Emerging themes were developed through inductive and deductive processes.
Ethics
The study received ethical approval from the Institutional Review Boards of Trinity College Dublin and Ifakara Health Institute (IHI). All data collection was carried out adhering to standard ethical procedures. The objectives of the study were explained and confidentiality was assured. Informed, signed consent was obtained from every respondent and all data and records were rendered anonymous through the use of a unique identity number. Prior to the data collection each of the nine selected councils was informed about tentative dates for data collection. As such, the relevant staff (the District Health Secretary, District Medical Officer (DMO), and District Reproductive and Child Health (RCH) Coordinator) at the council level were aware and prepared to receive the IHI research team. This facilitated planning and logistical arrangements for data collection. In every district data collection began after a brief introduction of the STEM team to the relevant council top officials i.e. the District Executive Director, District Medical Officer, and District Health Secretary
Results
In this section we will explore supervisors’ perceptions of the STEM intervention and in particular how HRM processes had impacted the supervision process.
Recording Keeping Systems
Overall, substantial changes occurred in STEM intervention facilities, and few occurred in STEM control facilities. Table 1 summarizes the changes (or lack of changes) recorded in four selected processes (supportive supervision; job descriptions for staff; personnel files for each staff; and absentee registers for each staff member). For example, supportive supervision guidelines were present and active in 12 of the 15 intervention a+b facilities (80%) and 10 of the 15 intervention a+b+c facilities (66.7%) at end-line data collection. Similar results were seen across other processes (personnel files, Job descriptions) but few facilities had implemented absentee registers for each staff member in all intervention facilities (a+b (5/15;33.3%) and a+b+c (4/15;26.7%).
| Item |
Intervention group |
Not present or active |
Became present and active during STEM |
Present and active since before STEM |
Valid N |
| Personnel files |
Control |
14 (93.3%) |
1 (6.7%) |
0 (0%) |
15 |
| a+b |
6 (40%) |
7 (46.7%) |
2 (13.3%) |
15 |
| a+b+c |
6 (40%) |
8 (53.3%) |
1 (6.7%) |
15 |
| Job descriptions |
Control |
14 (93.3%) |
1 (6.7%) |
0 (0%) |
15 |
| a+b |
3 (20%) |
9 (60%) |
3 (20%) |
15 |
| a+b+c |
6 (40%) |
8 (53.3%) |
1 (6.7%) |
15 |
| Supportive supervision guidelines |
Control |
14 (93.3%) |
1 (6.7%) |
0 (0%) |
15 |
| a+b |
2 (13.3%) |
12 (80%) |
1 (6.7%) |
15 |
| a+b+c |
5 (33.3%) |
10 (66.7%) |
0 (0%) |
15 |
| Absenteeism registers for staff |
Control |
14 (93.3%) |
1 (6.7%) |
0 (0%) |
15 |
| a+b |
2 (13.3%) |
5 (33.3%) |
8 (53.3%) |
15 |
| a+b+c |
6 (40%) |
4 (26.7%) |
5 (33.3%) |
15 |
Table 1: Changes or lack of changes to internal supportive supervision and HRM during STEM.
The main themes resulting from the focus group discussions are presented in Figure 1. The results clearly show that STEM had a positive impact from the CHMTs’ perspective. CHMT respondents in the a+b+c districts were particularly impressed by the systems that had been introduced by STEM trainees, such as improved record-keeping systems and files, A FGD respondent maintained, “…when we now visit the facilities under STEM project and compare to the facilities that are not under STEM, we get well-documented records in the facilities that are under STEM project.” (P1) Another respondent noted “STEM has been of so much help in the whole process of supervision from the facility level to the CHMT level, supervision has really been simplified, because records are kept in order and easy to find.” (CMUF4) Acquired record keeping skills were attributed to the STEM intervention and believed to have had an impact on external supervision as well, “. But again we do receive supervision from the council level…with the help of these records we keep it has been easy for them as well to conduct supervision using a less time than before when we did not have skills of keeping records.” (AI1) Other respondents maintained “What I can say is that, the impact of STEM in the facility has really simplified our work of supervision. At first we used to go to the facility and spend a lot of time searching for records…But after STEM came in…it hardly takes 5 minutes until you are given the records. So this has really helped us.” (P2). In addition introduction of recordkeeping systems had led to improved communication between internal supervisors and external supervisors, “…I did my best in keeping my records well; … since after the training supervisors come and find my records of data are well arranged, they changed and came with peace. I have learned from that to keep my records well” (AT4).
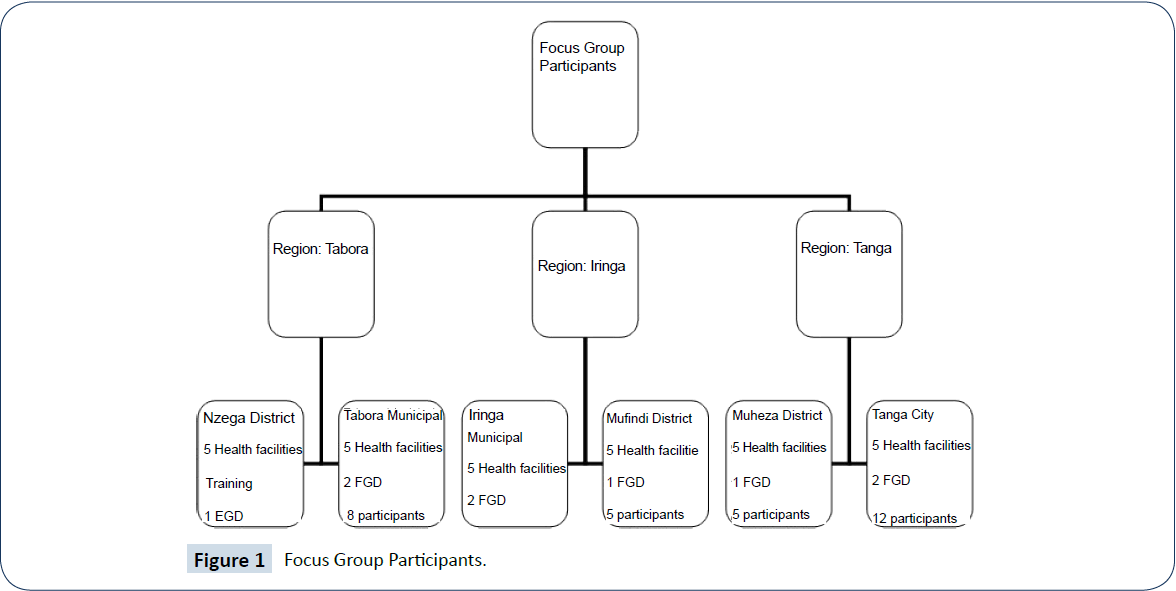
Figure 1: Focus Group Participants.
The introduction of personnel files was regarded as a new process in most facilities as only 2/15(13.3%) and 1/15(6.7%) in a+b and a+b+c facilities respectively had staff files in place pre intervention. CHMTs were impressed with the introduction of files for each staff member “…we have seen how useful the project has been to the facilities involved. For example, the issue of files for every staff at the facility is something so rare to find in facilities, but this project has managed to introduce that to the facilities and it is easy for us to visit a facility and get information on staff by checking his/her file.” (P2) Similarly, it was clear that the intervention had made supervision easier by saving time according to another CHMT member; “I can also say it has brought new strategies that have been so helpful in the supervision process, for example the introduction of files to keep records of each staff. So there is no more chasing to search for information that will take much time. You just get a file and all information is found.” (CI3) Another FGD respondent noted; “There is a lot that has changed after the STEM training even when visiting to facilities you can see there are files of staffs information and there are posters of elaboration of different cases. So there are a lot that has really changed.” (CMUF3)
The introduction of guidelines for recording supervision were regarded as instrumental in reorienting the supervisory encounter and these were almost non-existent prior to the STEM intervention in most facilities; Only 1/15 intervention facilities (a+b) reported having guidelines in place prior to the STEM intervention. CHMT respondents highlighted the contribution brought about by the introduction of supportive supervision guidelines “with the help of these record we are now able to conduct supervision using less time than before when we did not have skills of keeping records’’ (AI1).
In addition, a significant change was observed after the introduction of registers to monitor staff movement into and out of the facility, reducing unexplained absences and unauthorised movement from the facility during the working day. As noted introduction of this system had improved punctuality “It has even helped the punctuality of staff at the facility and solving of problems at the facility level’’ Al1.
Job Descriptions
A key section of the STEM training had focused on job descriptions as a performance management tool. The greatest improvement in the use of job descriptions was noted in a+b+c districts where only 1/15 (6.7%) were in place pre-intervention, increasing to 8/15 (53.3%) post intervention. In the FGDs job descriptions were embraced by supervisors following the STEM training “… ever since we received the training, we have given each other power of telling the duties to which everyone is assigned. After sitting with the one whom we lead, everyone knows her borders of work, to whom should she report…” (AT4). In some facilities, these job descriptions were viewed as a new strategy ‘ We came with the knowledge and introduced new things that did not exist in the facility, one of them is the introduction of job description and files for each staff in the facility, which we never had before” (Table 1).
(RATC5) An overall outcome of the intervention was managers and in-charges acquiring a suite of skills to implement internal supportive supervision, backed up by knowledge of relevant HRM systems that would support them (Figure 2).
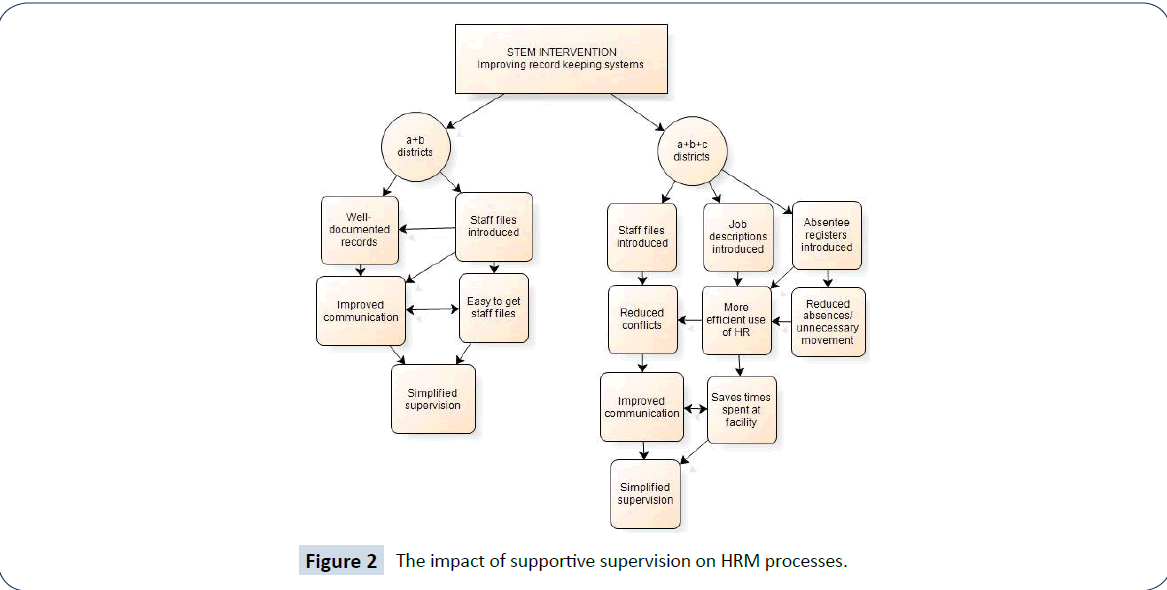
Figure 2: The impact of supportive supervision on HRM processes.
Discussion
Over all, the STEM multifaceted intervention that coupled supervision with training and ALS elicited important insights into the gaps inherent in record keeping systems within three selected regions in Tanzania. Facility records in this study revealed that most HR processes were not in place in facilities prior to the implementation of STEM. Pre and post-assessment of the control and intervention districts showed clear differences in terms of active HR policies and practices, with improved performance in the intervention districts. Inadequate job descriptions, inadequate supervision and poor regulation and monitoring can affect health workers performance and ultimately the quality of the care provided [38,39]. The findings from facility checklists support the statements from FGDs that the intervention had introduced new processes or revived the use of inactive processes in facilities.
Central to STEM’s intervention was to show that it is possible to improve the working environment by targeting managers and their approach to HRM. A critical component of the work environment, and one which has clear impacts on the satisfaction levels and retention of health workers is management support and supervision. STEM’s introduction of HRM processes in the work place, in particular job descriptions, supervision guidelines, personnel files and absentee registers were deemed most instrumental in supporting the supervision process. This study and others suggest that supportive supervision can improve service quality and increase the capacity of supervisors to support their staff.
One of the key benefits of the STEM intervention was the record keeping skills that CHMTs had acquired. Systematic record keeping systems led to an improved work environment, improved communication between health providers and supervisors. Inturn this eased the supervision process and saved on time spent supervising staff. However, it was noted that while the record keeping system was welcome, it was difficult to implement in some locations due to lack of finances to buy filing materials. A shortage of resources at the workplace has implications as it makes it very difficult for health workers to reach their targets. In settings where the availability of resources is severely compromised, health workers’ motivation becomes particularly vital for performance [40].
This study showed that guidelines for recording supervision were regarded as instrumental in reorienting the supervisory encounter. It has been shown that tools and techniques of supportive supervision, such as structured guidelines for external supervision and self-assessment instruments, are readily usable by health workers and supervisors in a wide range of settings [12] and was highlighted by FGD participants. While other studies collaborate this finding [11] others [15] note that such tools, if lengthy, could actually hinder supervision by causing fatigue and mechanical use [4].
High levels of absenteeism and low productivity of existing health workers in facilities in Tanzania and elsewhere have been reported [18,31,41,42]. A significant change articulated by FGD participants was observed after the introduction of registers to monitor staff movement into and out of the facility, reducing unexplained absences and unauthorised movement from the facility during the working day, although the introduction of absenteeism registers was less frequently mentioned in FGD of a+b facilities. Other studies [20] corroborate this finding noting that adequate supervision could reduce absenteeism and mitigate some factors that reduce health workers’ productivity. Absentee registers may be more difficult than other HR processes to implement, because they are more likely to lead to staff resistance. We suggest that improved communication between healthcare providers had the benefits of reduced conflicts in the work environment and the possibility of fewer unexplained absences. It is also likely that the support of peers that resulted from the ALS empowered supervisors to tackle these more difficult processes within their facilities.
This study showed that many staff had embraced the training from STEM that entailed the introduction of job descriptions as a performance management tool. Clear job allocations had been instigated in the facilities and health workers were aware of their responsibilities and for how long they were expected to work in a particular section. The latter was beneficial in-terms of providing health workers with experience and having clear job descriptions and this led to more efficient use of the workforce. CHMTs noted the benefits of having job descriptions in place, including the fact that it had reduced conflicts between health workers and supervisors evoking a peaceful working environment. In general CHMTs were positive about the reduction in their workload, which they attribute to the positive impacts of STEM on the facilities.
Our study has indicated that supervisors in resource constrained settings can benefit immensely from multifaceted interventions that place particular emphasis on empowering them to support their staff. Despite clear supervision national guidelines in Tanzania to support supervision this study highlighted gaps between practice and policy at the district level. It is not surprising that CHMTs embraced the STEM intervention approach, but expressed concern about non-intervention sites being placed at a disadvantage and suggesting that the STEM intervention ought to be implemented across all facilities. Participants in this study articulated the need to scale up this intervention to other areas in the country, as they not only realised the benefits, but were aware of the challenges in other areas of the country. However, simply scaling up interventions in weak health systems that deliver poor quality services is likely to waste resources and fail to accrue the anticipated benefits [43]. Implementation and roll-out of such supportive interventions will require concerted commitments at the national level [43].
There are some limitations in our study that need to be considered: some of the information required to assess elements of the project’s impact (e.g. absenteeism records) were not systematically available in all health facilities. What is more, some challenges were experienced during data collection; in some areas FGDs had to be rescheduled twice because participants did not turn up as anticipated.
Conclusion
This study was designed to identify perceptions of supervisors following the STEM intervention that sought to improve and support managers in low-income settings. The results clearly show that not only has it improved supervisors’ skill set but it has also had positive impacts on record keeping and the implementation of HR policies. The impact of the training on the importance of record keeping and the maintenance of HR records for staff clearly made a difference. In addition CHMTs were positive about the reduction in their workload, which they attributed to the positive impacts of STEM on the facilities and to improved documentation and record keeping skills.
Author Contributions
PM drafted the paper, EM designed the study, participated in data collection and analysis, and contributed to the paper. HMollel participated in the design of the study, data collection, and data analysis. OU participated in the co-ordination of the study and data analysis. HMasanja participated in the design, data analysis, and coordination of the project. All authors read and approved the final manuscript.
18339
References
- Iles V (1997) Really Managing Health Care. BMJ-British Medical Journal-International Edition 314:1424.
- Marquez L, Kean L (2002) Making supervision supportive and sustainable: new approaches to old problems, Maximizing Access and Quality (MAQ) Washington, DC, pp: 4.
- Flahault D, Piot M, Franklin A (1988)The supervision of health personnel at district level. Geneva: World Health Organization.
- Tavrow P, Kim YM, Malianga L (2002) Measuring the quality of supervisor–provider interactions in health care facilities in Zimbabwe. International Journal for Quality in Health Care 14:57-066.
- Manafa O, McAuliffe E, Maseko F, Bowie C, MacLachlan M, et al. (2009) Retention of health workers in Malawi: perspectives of health workers and district management. Human resources for health7:1.
- McAuliffe E, Bowie C, Manafa O, Maseko F, MacLachlan M, et al. (2009) Measuring and managing the work environment of the mid-level provider–the neglected human resource. Human resources for health7:1.
- World Health Organization (1994) Programme for Control of Diarrhoeal Diseases: ninth programme report, 1992-1993. World Health Organization, Diarrhoeal Diseases Control Programme, Switzerland.
- Management Sciences for Health. Family Planning Management Development (1993) Improving supervision: A team approach. Fam Plan Manager2:1-18.
- Agyepong IA (1999) Reforming health service delivery at district level in Ghana: the perspective of a district medical officer. Health Policy and Planning14:59-69.
- Marquez L (2001) Helping healthcare providers perform according to standards. Operations Research Issue Paper 2:1-34.
- Stanback J, Brechin S, Lynam P, Toroitich-Ruto C, Smith T, et al. (2001) The effectiveness of national dissemination of updated reproductive health/family planning guidelines in Kenya. Final report. Family Health International pp: 9.
- Lynam P, Rabinovitz L, Shobowale M (1992) Use of self-assessment in improving the quality of family planning clinic operations: The experience with cope in Africa.Association for voluntary surgical contraception.
- Ministry of Health and Social Welfare Tanzania (2010) National Supportive Supervision Guidelines for Quality Healthcare Services. Dar es Salaam: Ministry of Health and Social Welfare.
- Ministry of Health Malawi (2004) A Joint Programme of Work for a Health Sector Wide Approach (SWAp) 2004–2010: Republic of Malawi. Ministry of Health.
- Center for Human Services (1987) Solving Operational Problems in Primary Health Care 1981–87: Final Report of the PRICOR Project. Maryland.
- Leong C, Buising K, Richards M, Robertson M, Street A (2006) Providing guidelines and education is not enough: an audit of gentamicin use at The Royal Melbourne Hospital. Internal medicine journal36:37-42.
- Dovlo D (2005) Wastage in the health workforce: some perspectives from African countries. Human Resources for Health 3:1.
- Manzi F, Schellenberg JA, Hutton G, Wyss K, Mbuya C, et al. (2012) Human resources for health care delivery in Tanzania: a multifaceted problem. Hum Resour Health 10:3.
- Sparkes S, Ohiri K, Vujicic M (2009) Working in Health: Financing and Managing the Public Sector Health Workforce. World Bank.
- Frimpong JA, Helleringer S, Awoonorâ€ÂÂÂÃÂWilliams JK, Yeji F, Phillips JF, et al. (2011) Does supervision improve health worker productivity? Evidence from the Upper East Region of Ghana. Tropical Medicine & International Health16:1225-33.
- Dominick A, Kurowski C (2005) Human resources for health–an appraisal of the status quo in Tanzania mainland. Dar es Salaam: Ifakara Health Research Development Centre/The World Bank/the London school of hygiene and tropical medicine.
- Bryant M, Essomba RO (1995) Measuring time utilization in rural health centres. Health Policy and Planning10:415-22.
- Bradley S, Kamwendo F, Masanja H, de Pinho H, Waxman R, et al. (2013) District health managers’ perceptions of supervision in Malawi and Tanzania. Human Resources for Health 11:43.
- Wiedenmayer KA, Kapologwe N, Charles J, Chilunda F, Mapunjo S, et al. (2015) The reality of task shifting in medicines management- a case study from Tanzania. Journal of Pharmaceutical Policy and Practice8:1-8.
- Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, et al. (2008) Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ337:a1655.
- McCord C, Mbaruku G, Pereira C, Nzabuhakwa C, Bergstrom S, et al. (2009)The quality of emergency obstetrical surgery by assistant medical officers in Tanzanian district hospitals. Health affairs (Project Hope) 28:w876-85.
- Kruk ME, Galea S, Prescott M, Freedman LP (2007) Health care financing and utilization of maternal health services in developing countries. Health Policy and Planning22:303-10.
- Stringhini S, Thomas S, Bidwell P, Mtui T, Mwisongo A, et al. (2009) Understanding informal payments in health care: motivation of health workers in Tanzania. Human Resources for Health 7:1.
- Simba D, Mwangu N, Msamanga G (2004)Rationalising human resource deployment in the wake of reforms: the need for measuring health workers workload. Tanzania Medical Journal19(2).
- Olsen OE, Ndeki S, Norheim OF (2005) Human resources for emergency obstetric care innorthern Tanzania: distribution of quantity or quality? Human Resources for Health3:1.
- Munga MA, Mæstad O (2009) Measuring inequalities in the distribution of health workers: the case of Tanzania. Human Resources for Health7:1.
- Serneels P, Lindelow M, Montalvo JG, Barr A (2007) For public service or money: understanding geographical imbalances in the health workforce. Health Policy and Planning 22:128-38.
- McCoy D, Bennett S, Witter S, Pond B, Baker B, et al. Salaries and incomes of health workers in sub-Saharan Africa. The Lancet 371:675-81.
- National Audit Office (2008) Aperformance audit report on the management of primary health care: Acase study of health centres. Dar es Salaam: Office of the controller and auditor general of Tanzania.
- Ministry of Health and Social Welfare (2012) Human resource for health strategic plan 2008 – 2013. Midterm evaluation draft report.
- Frey JH, Fontana A (1993) The Group interview in social research. In: Successful focus groups: Advancing the State of the Art. SAGE Publications pp: 20-35.
- Lofland J, Lofland LH (1984)Analyzing Social Settings: A Guide to Qualitative Observation and Analysis. [4 edn] Wadsworth Publishing Company.
- Ahmed AM, Desta A, Tekle K, Mweta EA (1993)Pursuing better health care delivery at district level. World Health Forum 14: 360-366.
- Salem BB, Beattie KJ (1996) Facilitative supervision: a vital link in quality reproductive health service delivery. AVSC International.
- Songstad NG, Moland KM, Massay DA, Blystad A (2012) Why do health workers in rural Tanzania prefer public sector employment? BMC health services research 12:1.
- Chen L, Evans T, Anand S, Boufford JI, Brown H, et al. (2004) Human resources for health: overcoming the crisis. Lancet 364: 1984-1990
- Kruse GR, Chapula BT, Ikeda S, Nkhoma M, Quiterio N, et al. (2009) Burnout and use of HIV services among health care workers in Lusaka District, Zambia: a cross-sectional study. Human Resources for Health 7:1.
- Rowe AK, Savigny D, Lanata CF, Victoria CG (2005) How can we achieve and maintain high-quality performance of health workers in low-resource settings? Lancet 366: 1026-1035.

