Keywords
Closed abdominal trauma; Diagnosis; Laparocenteza
Introduction
Among the most important tasks of modern public health in all countries of the world declining, as injuries and deaths resulting from mechanical damage in all age groups of the population. This is due to the fact that against the background of the progression of the mechanization of the working and rest time occurs and the rapid growth of various types of injuries in the home, the workplace, transportation, during sports, school, etc. Financial losses from the increased injuries huge and not only this, but also that people are dying and, especially, often at a young age. There is a need not only for effective injury prevention among the general population, but also to the timely diagnosis of closed injuries, including abdominal organs. Mortality from injury 10 years ago was 55, 42 to 100 thousand. of the population, with males of working age she was at 11.4% to 24.5% higher compared to overall mortality. The death rate from injury in peak 30-39 years. At this age, compared with children, dies in 10 times more people. The second increase in mortality from trauma begins with 47 years, reaching a peak among persons 80-84 years that related to the general deterioration of health status from year to year. Men are dying from injuries in 2 times more often than women, while in the age group 20-29 years 5.7 times, and in the 30-39 years, 5.9 times. Out of the total number of fatalities from accidents had alcohol 58% to 68%, while the 1/3 misfortune happened through the fault of the drunk driver [1,2]. People with elevated blood alcohol noticeably lose orientation in space and it dulled critical reflection of their conduct. Often it just interferes with a survey. Fatal injuries most often occur in everyday life (44.9%), then during traffic accidents-33.2%, rail-9.9%-6.0% manufacturing, Street-3.3%, other-2.7% 4 month at hot (June-September) accounted for 40.6% of all deaths. However, injuries (15%), street most often occurs in October and November (The main cause of ice). The greatest number of fatal injury in the last days of the week-on Friday-Sunday (14.8-15.6%). Of the total number of injured persons at the pre-hospital stage perishes 56.1% and at home 10.5% [3].
Distinguish between isolated, combined and multiple closed mechanical damage to the abdominal organs. In a stand-alone injured only one body, with multiple-other bodies, but the same system, with the concomitant-tissues and organs of other systems. In closed traumas the integrity of skin and mucous membranes. These lesions can be full (Both damaged parenchyma, and capsule) and incomplete when torn or only the capsule, or parenchyma of the body with the formation of podkapsul noj hematoma, which may in the future or to organize, or break into the free abdomen, that is going to happen, so called dvuhmomentnyj its gap. The condition most commonly occurs when the spleen injury. Links razmozjenie distinguished body, his legs from vascular avulsion, damaging one of the poles and break through the gates of the body. Such closed insulated and multiple injuries accompanied by symptoms of traumatic shock and acute blood loss, which makes it easier to diagnose. When combined the same injuries, of which the most frequent fractures of various bones Osteoarticular and traumatic brain injury, the severity of the condition affected increases dramatically. It should be noted that sometimes the symptoms that accompany the combined damage externally manifest themselves more manifesto compared with symptoms from the trauma of abdominal organs, which can cause serious medical error, both in terms of early diagnosis and formulating rational treatment algorithm. In this process, certain negative role plays and concomitant intoxication. The issues rose in the medical literature, in our view, not enough attention has been devoted. Dominated by a wait-and-see tactic that could lead to serious consequences, although it has been known for a simple and quick way of recognition of abdominal catastrophe is laparocenteza.
In recent years, the frequent observation of natural and man-made disasters when hospitals immediately come to ten and more victims to all rescue and a limited number of health care workers and they have sort of affected the principle of providing assistance to those most in need first, and then really rest [1-3]. Of particular importance in this regard belongs to the techniques that enable you to quickly understand the health status of the incoming person. To methods such as times and dates laparocenteza, which allows for a few minutes to recognize a catastrophe in the abdominal cavity. However, the traditional method of laparocenteza carries a certain danger [4,5]. In fact, the proposed zone entrance needle or tracer into the abdomen does not guarantee the safety of the bladder and other organs from this tool. All surgical guides recommend puncture the abdominal wall to the white line in the middle of the distance from the junction of the lanugos and to the navel [6-8], but the trauma of the abdomen muscles bladder lose their airway and bladder urine becomes saturated and it’s the bottom can reach up to the navel and even higher. And then, when the specified zone punctures, damage to the wall of the bladder, urinary peritonitis [9,10]. Not only may the end of the tool not penetrate into the free abdomen as distended bubble slipped up the peritoneum. In this zone there are no muscles, and the skin to aponevroza evil is present, and that to the peritoneum and following through the puncture can long trickle liquid that can result in infection of the abdominal cavity. There are other dangerous reasons to abandon the traditional area of the puncture. Having said that, we use another zone for laparocenteza.
Materials and Methods
Of the 565 affected with closed abdominal injuries in different hospitals in the Krasnodar region, 106 (28.7%) difficulties in diagnosis. the age of the victims was from 17 up to 72-years-old, of whom 80 were men (75.4%). Patients with isolated injury was 92 (86.6%), with concomitant-14 (13.4%), of which fracture of ribs to the left was a 6-2, sternum, left shoulder-2, and 4 there was a severe brain injury while intoxicated was 48 (45.2%) man All of these victims was made of them laparocenteza 66 (63%) According to the traditional method and 40 (37%)-modernized (Figure 1). The main groups of patients (40 people) is made through the puncture laparocenteza troche (1) of the anterior abdominal wall to -2.01.5 cm below and to the left of the navel (2). Part 1 shows the entry point of the tracer in the anterior abdominal wall. Part 2 shows a channel passage tracer from entry points on the skin to rubcovomu ring from the abdominal cavity, where soldered peritoneum. Where 3 skin, 4-Aponeurosis front sheet, 5-Aponeurosis rear leaf, 6-peritoneum. Procedure performed under local anaesthesia. Puncture the abdominal wall produced through direct muscle belly in the slanting towards the navel. In this zone the peritoneum sarashina with scar tissue and does not exfoliate when passing through the instrument. Penetration of the end of the trocar into the abdominal cavity is clearly felt. This eliminates the desire to promote the end of tool deep into the cavity. Once the moment of puncture of peritoneum, stiletto is removed and the study of abdominal effusion occurs. If it is not, is an audit this cavity to Berkutovu [2,4,5]. For this purpose from disposable intravenous fluid system vykraivaetsja tube length 50-60 cm. At its end is made two or three openings, and this end is inserted in the cavity in different directions (sharjashhij catheter). If the proceeds of the liquid not, intra-abdominal enter 250-300 ml of saline solution, which then flows by gravity to the outside according to the law, capillarity. Actively suck it back is not recommended because it causes and podsasyvaniju to the tube loops of intestines. If blood, bile, gastric contents and other liquids much, then perform a laparotomy, but if little, laparoscopy, and only after that the question about abdominal surgery.
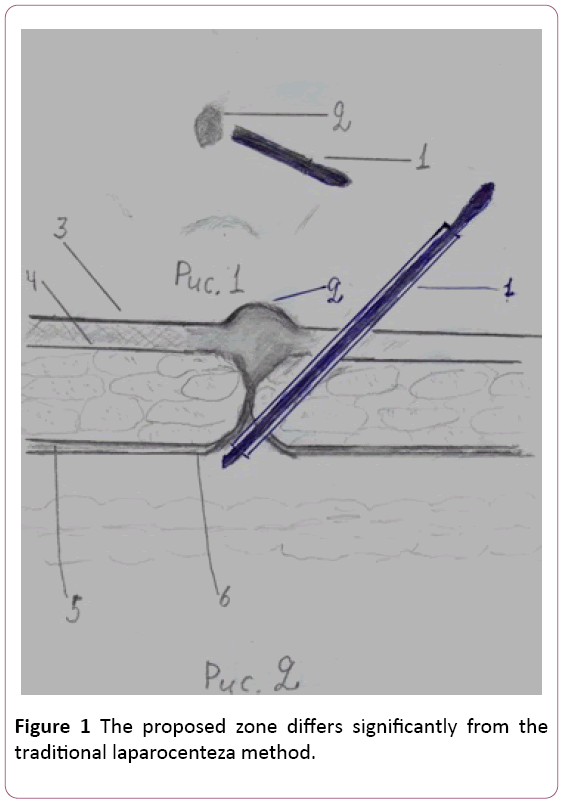
Figure 1: The proposed zone differs significantly from the traditional laparocenteza method.
Result
Of 40 observations, none of them was injured abdominal organs in entering the end of trocar in free abdominal cavity. At 26 (65%) patients described method allows users to determine the availability of closed injury of spleen, liver and other organs and they performed emergency surgery polostnaja. Others 14 (25%) patients did not need it that confirmed upon further observation. Previously, when executed laparocenteza traditional way, the damage to the bladder and other organs located in the pelvic cavity 3 have occurred (4.5%). When an isolated injury mortality was 2.1% (from 92 patients died 2), and in concomitant-14.2% (14 patients died 2 from brain injury).
Discussion
Laparocenteza need to include effective diagnostic tool for closed abdominal injury. It allows you to quickly determine whether the patient had injuries this cavity, which is very important when bulk flow of victims. However, it must be careful not to injure your bladder and pelvic organs. Most have to do it properly through the zone that is safe for puncture is -21.5 cm left and thinner belly button. Puncture tissues should be implemented in the slanting towards the navel. In this section of the abdominal peritoneum srashhena with navel and scar tissue does not exfoliate with the passage of the trocar. The bladder is not damaged because it is below the seat topographically puncturing the abdominal wall.
The proposed zone differs significantly from the traditional laparocenteza method. It significantly reduces the risk of trauma of abdominal organs. This is important when mass assignment of this procedure. It's easy to perform even novice surgeons. When doctors it will find its rightful place in the diagnosis of abdominal injuries.
Conclusion
In case of closed trauma of abdominal organs need to resort more frequently to laparocenteza. Subject to the necessary caution he safe because available. For its implementation does not require expensive tools and finding the resuscitation Ward, that when bulk flow affected the medical institution is of paramount importance. This method allows you to quickly and accurately perform medical triage towards determining the urgency of the surgery a victim. It must be on the left and below the navel on -2.01.5 cm, not to injure the bladder, if he is in a State of paresis and overflowing with urine.
Conflict of Interest
The authors declare no conflict of interests.
23490
References
- Ermolov AS (2006) Abdominal trauma/AS ermolov, MM abakumov. Guide to emergency abdominal surgery. Clinic and diagnostics. Triada-X, Moscow pp: 425-433.
- Lebedev NV (2002) Diagnosis abdominal injuries in associated trauma/NV Lebedev, MM Abakumov, VN Malyarchuk. surgery 12: 53-58.
- Cepa LS (1998) Damage to spleen/LS Cepa. Clinical surgery, Reference guide for doctors under the editorship of Ym Pancyreva-ÃÂÂÃÂÂœ: medicine pp: 346-347.
- Abdulaev AG (2013) Hospital surgery. Sindromalogija. Tutorial. GEOTAR- media.


