Mohammed Ibrahim1*, Norbert Friedel1, Christoph Erdmann1, Claus Steppert2 and Bernd Linsmeier1,*
1 Department of Cardiothoracic Surgery, Bayreuth Hospital, Bavaria, Germany
2 Clinic of Pulmonology, Thoracic Oncology, Sleep and Respiratory Medicine, Bayreuth Hospital, Bavaria, Germany
- *Corresponding Author:
- Mohammed Ibrahim
Department of Cardiothoracic Surgery,
Bayreuth Hospital, Bavaria, Germany.
Tel: 0921 400-5902
E-mail: mohammed.ibrahim@klinikum-bayreuth.de
Bernd Linsmeier
E-mail: thoraxhirurgie@klinikum-bayreuth.de
Received date: May 16, 2018: Accepted date: May 21, 2018; Published date: May 28, 2018
Citation: Ibrahim M, Friedel N, Erdmann C, Steppert C, Linsmeier B (2018) Unilateral Reexpansions Pulmonary Edema after Thoracic Drainage Insertion in Patient with Extensive Para-pneumonic Pleural Effusion. J Univer Surg. Vol.6 No.2:13
Keywords:
Pulmonary edema; Atelectatic lung; Pleural effusion; Thoracic
Case Report
A 24-year-old patient with tetraparesis presented herself in the Emergency Department of our Hospital with dyspnea and fever of 38.9°C late in the evening.
Clinical, Laboratory and Radiological Values
The laboratory chemistry showed increased infection parameters of leucocytes 38.7/nl and CRP of 31.8 mg/dl.
In X-ray of thorax total shading on left. When empyema was suspected, a chest CT scan was performed with a complete left atelectatic lung and extensive pleura effusion (Figures 1a and 1b).
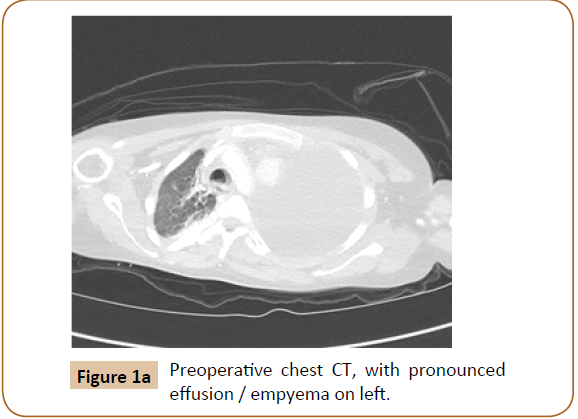
Figure 1a: Preoperative chest CT, with pronounced effusion / empyema on left.
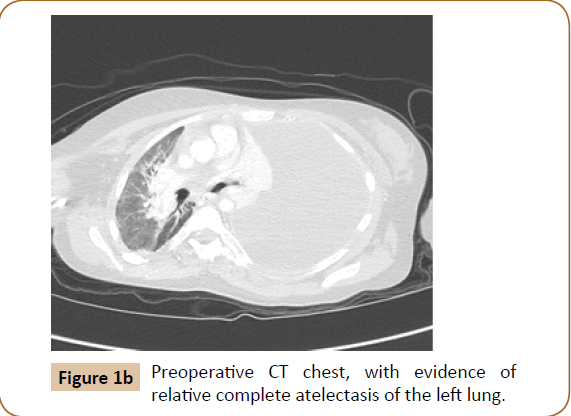
Figure 1b: Preoperative CT chest, with evidence of relative complete atelectasis of the left lung.
Therapy
As therapy, the immediate insertion of a 24 CH chest tube in local anesthesia in the 6th ICR was performed in the middle axillary line with an initial suction of -20 cm H2O. It spontaneously deflated nearly 950 ml of putrid secretions (Figure 2).
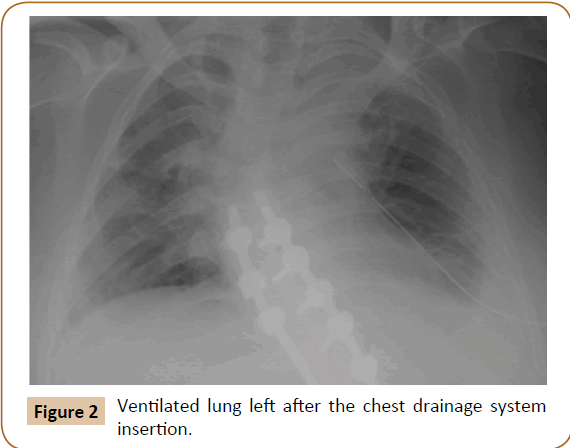
Figure 2: Ventilated lung left after the chest drainage system insertion.
Follow
The X-ray chest radiograph after chest tube insertion showed fully extended lungs on both sides without evidence of pneumothorax and correct location of chest tube. In the first 24 h, the drainage pumped about 2000 ml purulent secretions.
After 24 h, the condition worsened and the patient complained of increased dyspnoea, tachypnoea, tachycardia, respiratory insufficiency, with necessary for intubation and mechanical ventilation. The X-ray thorax follow-up showed a pronounced ipsilateral (left) shadow. Thoracic drainage was open and not stenotic with fibrin or old blood coagulation; bronchoscopic revealed a few mucous secretions endobronchially left. This confirmed the diagnosis of the full image of re-expansion pulmonary edema (Figure 3).
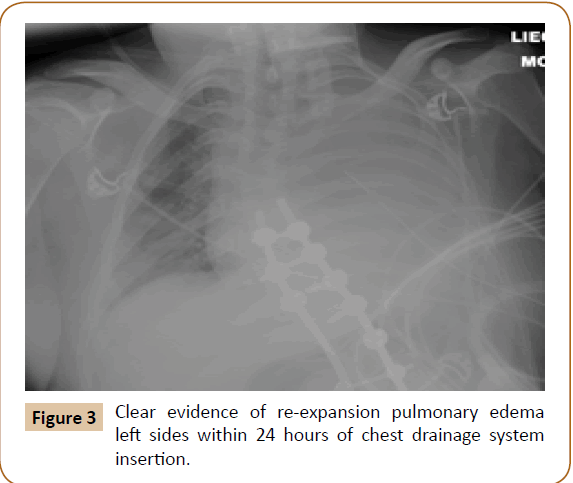
Figure 3: Clear evidence of re-expansion pulmonary edema left sides within 24 hours of chest drainage system insertion.
The weight-adapted administration of prednisolone, mechanical ventilation, PEEP of 7, a FiO2 of 45% and diuretic therapy showed a significant improvement in the generalized status of the patient.
The X-ray done on the following day showed a complete extended lung with significantly declining shadowing without infiltration (Figure 4).
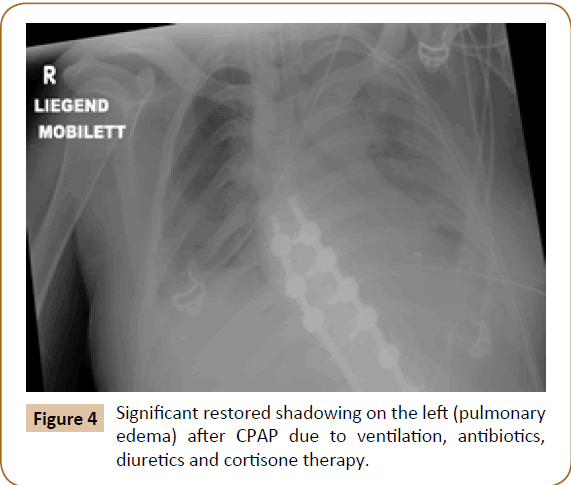
Figure 4: Significant restored shadowing on the left (pulmonary edema) after CPAP due to ventilation, antibiotics, diuretics and cortisone therapy
After stabilization of the patient's condition, an operation has been done, as VATS (Video Assisted ThoracoScopy) left sides with decortication. Because of further respiratory insufficiency it has been performed a plastic tracheotomy.
Discussion
The occurrence of re-edema is a rarity (<1%), although in some international literature it has been described in some case reports.
Unilateral re-expansive edema is described as a rare complication in pneumothoracic therapy as well as in the treatment of extensive pleural effusion, with a lethality of up to 20% [1].
The clinical and radiographic manifestations vary from a pale radiographic finding with an asymptomatic patient to a fulminant course with respiratory insufficiency and shock symptoms. Main risk factors are:
- Young patient age.
- Larger and longer existing pneumothorax (>24 h).
- Relative total lung atelectasis pleura effusion or empyema-related compression.
- Rapid re-expansion of the lungs.
In case of fulminant progressions as in the case described; however, invasive or non-invasive CPAP ventilation may become necessary.
With a corresponding risk profile, it is recommended for prophylaxis to prevent the direct connection of the thoracic drainage to the suction pump with high suction negative – 20 cm H2O pressure and to initially use only the bottle water system - drainage unit or connection to suction pump with physiological weak pressure – 8 cm H2O. This can ensure a slower re-expansion of the lung [2].
Conclusion
Although there are no major studies on the risk factors and on the management of extensive pneumothorax or increased effusion, empirical evidence suggests that relieving the pleura of more than two liters of air or effusion significantly increases the risks of re-expansion lung edema.
Re-pulmonary edema is a non-cardiac unilateral pulmonary edema observed after treatment of pneumothorax or after drainage of large-volume pleural effusions.
Pathogenesis is unclear, most likely a permeability pulmonary edema in which as micro vascular injury occurs due to mechanical stress associated with lung expansion (capillary leaks).
Conflict of Interest
The authors declare that there is conflict of interest.
22959
References
- Schmidt-Horlohé N, Azvedo CT, Rudig L, Habekost M (2008) Fulminant unilateral pulmonary edema after insertion of a chest tube: A complication after a primary spontaneous pneumothorax. Dtsch Arztebl Int 105: 878–881.
- Huber LC, Wieser S (2013) Re-expansion lung edema. Schweiz Med Forum 13: 349–350.

